0037
Four-dimensional iterative motion correction (iMoCO) for isotropic stack-of-spirals cine imaging at 0.55T1National Heart, Lung and Blood Institute, Bethesda, MD, United States, 2Case Western Reserve University and University Hospitals, Cleveland, OH, United States, 3University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Image Reconstruction, Cardiovascular, Image Reconstruction, Low-Field MRI, Data Acquisition
Motivation: Three-dimensional (3D) isotropic cine imaging can be resliced and resampled for clinical diagnosis and planning for structural interventions. Currently, these 3D cine approaches are hampered by long scan times.
Goal(s): To demonstrate cardiac-resolved iterative motion compensation (iMoCo) for a free-breathing stack-of-spirals 3D cine with optimized acquisition ordering at 0.55T
Approach: The 3D cine was acquired in five healthy volunteers and one patient, reconstructed with cardiac-resolved iMoCo, and compared to a reference 2D cine.
Results: The proposed method yielded high quality 3D cines. Volumetric measurements had good agreement with reference data (-2.3 ± 2.8% and 3.9 ± 10.4% in diastole and systole respectively).
Impact: A gaussian-distributed stack-of-spirals sampling scheme paired with an iMoCo reconstruction improves image quality and sharpness for isotropic three-dimensional cines. This technique can be a useful tool for interventional planning and assessment or as a one-stop shop for diagnostic cardiovascular MRI.
Introduction
Isotropic three-dimensional cardiac cine imaging can be retrospectively resliced into arbitrary slice orientations, aiding clinical diagnosis in patients with complex anatomy and forming pre-procedural planning for structural heart interventions. Previous studies have demonstrated isotropic 3D cines using Cartesian and radial sampling1-3, however, spiral imaging can leverage the field homogeneity at 0.55T to improve sampling efficiency. In this study, we investigate a free-breathing, stack-of-spiral acquisition for 2mm isotropic coverage of the left ventricle at 0.55T. Here we optimize the sampling distribution and develop a cardiac-resolved iterative motion correction (iMoCo) technique to include data from all respiratory states4-5.Methods
Institutional review board approval and informed consent was obtained for imaging studies. Healthy volunteers (n=5), and a patient with non-ischemic cardiomyopathy (n=1) were imaged at 0.55T (prototype MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany).The iMoCo technique4 was expanded to a 3D+t reconstruction, with an additional cardiac dimension, using the Gadgetron framework5 (Fig. 1). First, the respiratory navigator signal was extracted from the center of k-space (“DC signal”) and used to reconstruct 8 respiratory phases using constrained reconstruction with spatio-temporal TV constraints. Deformation fields were subsequently extracted from these images using an optical flow-based image registration6,7 and used in the iterative motion-corrected reconstruction4-5, to reconstruct cardiac-resolved images with data from all respiratory positions using the following cost function:
$$ argmin_X \sum_{n,k,c}^{N_c,K,C} \lVert W_{k,c} (FS_nM_kX-d_{n,k,c})\rVert_2^2 + \lambda_sTV_s(X) + \lambda_tTV_t(X)$$
where dnkc is motion-resolved multi-channel data, X is the end-expiration cardiac resolved images to be reconstructed, Mk is estimated motion field across respiratory positions, Sn is coil-sensitivity of the nth channel, F is the non-uniform Fourier transform, Wk is the density compensation weight for each respiratory and cardiac motion states, and TV is the spatial and temporal total variation term. Nc represents total number of channels, K is the total number of respiratory states, and C is the total number of cardiac phases. Twenty-five cardiac phases were retrospectively binned using the recorded ECG. The iMoCo cine reconstruction was compared to respiratory averaged and end-expiration images using the previously described stable binning8 (which uses 40% of the data).
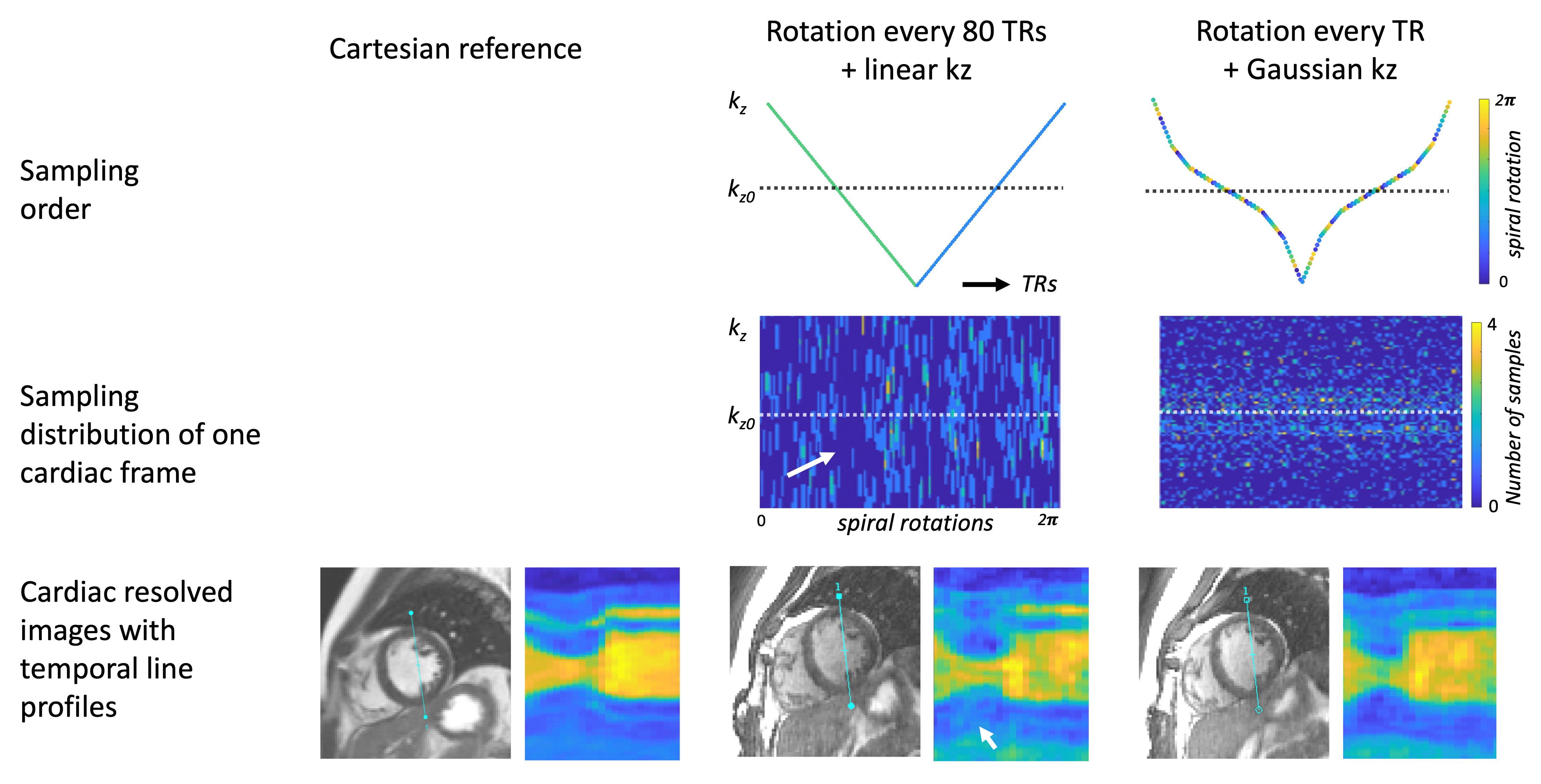
Free-breathing bSSFP 3D stack-of-spirals acquisitions were acquired in a short-axis orientation (2.0 mm isotropic, TE/TR=1.1/4.5ms, flip-angle=50°, 64 partitions with 25% over-sampling, total acquisition time ~6 min). For slice (kz) sampling, we compared a linear distribution to an approximated Gaussian distribution. A pseudo golden step was used between interleaves, which occurred every 80 TRs for the linear ordering scheme designed to minimize eddy currents, whereas this occurred every TR for the Gaussian distribution (Fig. 2).
We compared our images to reference free-breathing 2D cine stack (acquired voxel-size=1.9x2.5x8.0mm, TE/TR=1.3/3.2ms, flip-angle=80°, 11 slices with 25% gap, total acquisition time ~3.5 min), reconstructed with a real-time motion compensation9.
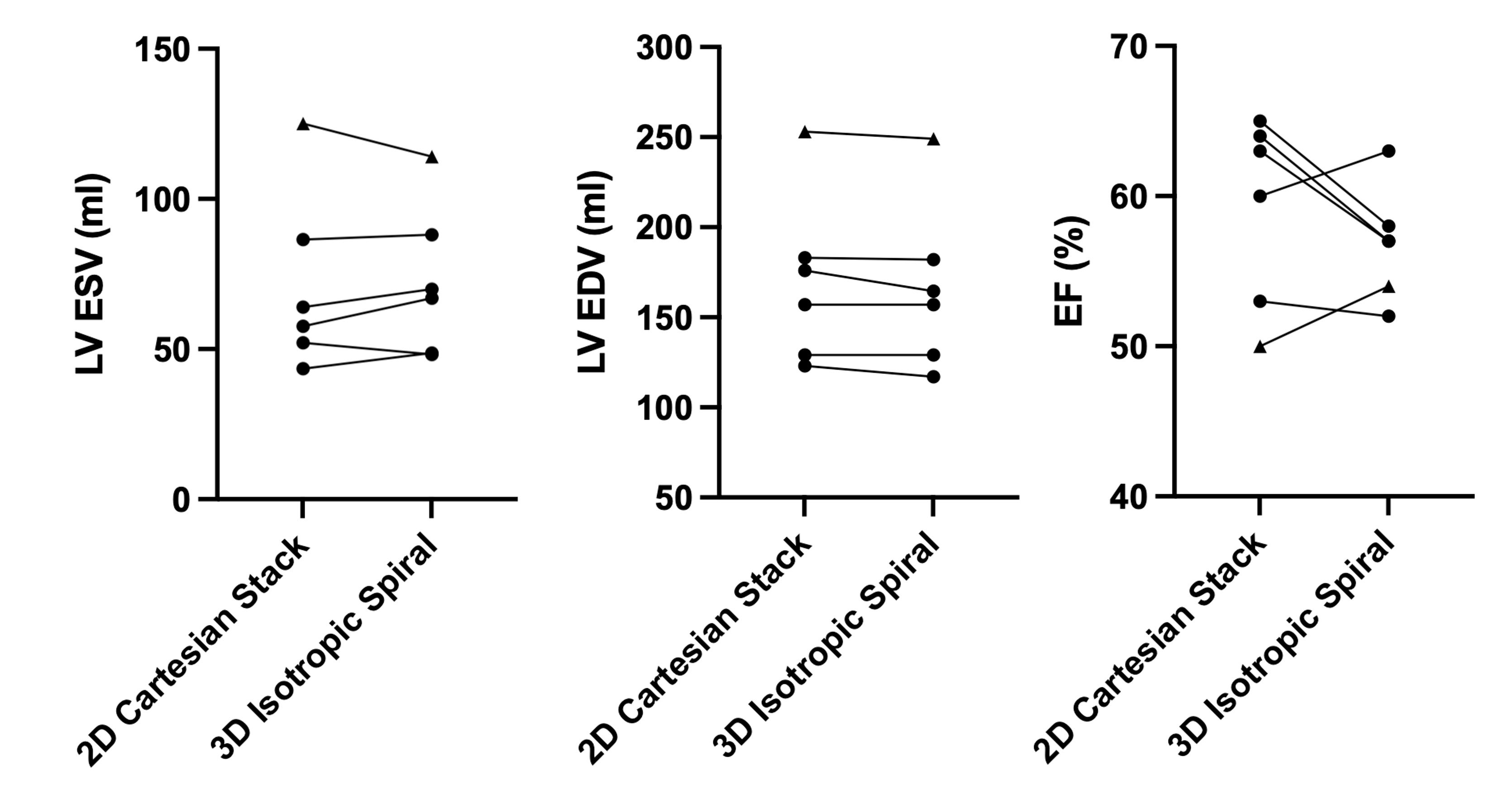
2D and 3D cine datasets were semi-automatically segmented in SuiteHeart (NeoSoft, Pewaukee, Wisconsin, USA) to compare left-ventricular end-systolic volume (LV-ESV), end-diastolic volume (LV-EDV) and ejection fraction (EF), for Bland-Altman analysis.
Results and Discussion
The stack-of-spiral 3D isotropic (2mm) cine acquisition exhibited improved dynamic image quality when using a Gaussian kz sampling scheme (Fig 2), in comparison to the linear sampling scheme. This is likely a result of the center of k-space being smoothly filled across cardiac phases.The isotropic cine acquisition with 25 cardiac phases was feasible with a 6 minute acquisition in all healthy volunteers. As expected, the 3D iMoCo reconstruction improved image quality over respiratory averaged acquisitions (Fig 3). Some acquisitions did exhibit residual streaking artifacts that were aligned with fat signal and may be reduced with further image reconstruction optimization.
Isotropic 3D cine provided good blood-myocardium contrast and compared well with reference acquisitions and maintained good quality cines when resliced to typical cardiac planes (Fig. 4).
The mean LV-ESV difference was -1.3 ± 7.5 ml, the mean LV-EDV difference was 3.8 ± 4.5 ml and the mean EF difference was 2.3 ± 5.1 % (Fig. 4), similar to previous cine comparison studies2,3,10.
Conclusion
In this preliminary study, we demonstrated an isotropic free-breathing 3D cine with an optimized stack-of-spiral sampling scheme. We implemented a novel cardiac-resolved iMoCo reconstruction, which, to our knowledge, has not been reported before. 3D isotropic cine imaging can be used as a ‘one-stop’ acquisition for diagnostic volume and function measurements, or can inform pre-procedural planning for intervention by facilitating efficient patient-tailored image reformatting akin to CT.Acknowledgements
This work was supported by the NHLBI DIR (Z01-HL006213, Z01-HL006257). We would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T under an existing cooperative research agreement between NHLBI and Siemens Healthcare.References
1. Feng, L., et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn. Reson. Med., 2016; 75:775–788.
2. Usman, M. et al. Free breathing whole-heart 3D CINE MRI with self-gated Cartesian trajectory. Magn. Reson. Med., 2017; 38:129–137
3. Küstner, T., et al. Fully self-gated free-running 3D Cartesian cardiac CINE with isotropic whole-heart coverage in less than 2 min. NMR in Biomedicine, 2021;34:e4409.
4. Zhu, X., et al. Iterative motion‐compensation reconstruction ultra‐short TE (iMoCo UTE) for high‐resolution free‐breathing pulmonary MRI. Magn. Reson. Med., 2020; 83:1147-1527
5. Javed, A., et al. Improved 3D stack-of-spiral UTE pulmonary imaging at 0.55T using iterative concomitant field and motion corrected reconstruction (iCoMoCo). Proc. Intl. Soc. Magn. Reson. Med., 2022; 31:1397.
6. Zachiu C, et al. An improved optical flow tracking technique for real-time MR-guided beam therapies in moving organs. Phys. Med. Biol. 2015;60:9003 doi: 10.1088/0031-9155/60/23/9003.
7. Ozenne V, et al. 3D motion strategy for online volumetric thermometry using simultaneous multi-slice EPI at 1.5T: an evaluation study. Int. J. Hyperth. 2023;40 doi: 10.1080/02656736.2023.2194595.
8. Javed, A., et al. Self-gated 3D stack-of-spirals UTE pulmonary imaging at 0.55T. Magn Reson Med . 2022;87(4):1784-1798
9. Xue, H., et al. Distributed MRI reconstruction using gadgetron-based cloud computing. Magn. Reson. Med., 2015; 73 (3):1015-1025
10. Bandettini W.P., et al. A comparison of cine CMR imaging at 0.55 T and 1.5 T. J Cardiovasc Magn Reson. 2020;22(1):37.
Figures