0035
How chronic cortical hypoperfusion affects choroid plexus in patients with moyamoya disease?1Department of Neurosurgery, Tokyo Medical and Dental University, Tokyo, Japan, 2Department of Radiology, Juntendo University Graduate School of Medicine, Tokyo, Japan, 3Department of Radiology, Toho University Omori Medical Center, Tokyo, Japan
Synopsis
Keywords: Neurofluids, Ischemia, moyamoya disease
Motivation: How chronic cortical hypoperfusion affects choroid plexus, an important structure to maintain neurofluid dynamics, has rarely reported.
Goal(s): To investigate changes of choroid plexus after revascularization surgery to improve chronic hypoperfusion in patients with moyamoya disease.
Approach: Eighteen adult patients with moyamoya disease were evaluated with T1WI and ASL before and one year after surgery. Choroid plexus volume and cortical perfusion were compared before and one year after the surgery.
Results: After the surgery, choroid plexus volume decreased (1.65 (0.55) ml vs. 1.52 (0.51) ml; P=0.014), while cortical perfusion improved (P=0.001).
Impact: Choroid plexus may be hyperactivated and proliferated when cortical hypoperfusion and decreased glymphatic system function exist. After the revascularization surgery and restoration of cortical perfusion and glymphatic system function, choroid plexus may shrink to the normal function.
Objective/background
The Choroid plexus is an important organ that produces cerebrospinal fluid (CSF) and maintains the blood-CSF barrier. Recent studies have shown choroid plexus has been affected by many physiological conditions and neurological diseases1. However, choroid plexus changes under chronic cerebral ischemia are rarely reported. Moyamoya disease is a rare cerebrovascular disease causing intracranial arterial stenosis and chronic cortical hypoperfusion2.The aim of this study was to investigate the choroid plexus changes under chronic cortical hypoperfusion in patients with moyamoya disease.
Materials and Methods
ParticipantsThis study was approved by the ethical committee of local institutes. Eighteen patients with moyamoya disease were prospectively included in this study (Table 1). All patients received revascularization surgery and were evaluated with magnetic resonance imaging (MRI) protocol before and one year after the surgery.
MRI protocol
Images were acquired by 3 T systems (Signa HDxt; GE Healthcare, Waukesha, WI for arterial spin labeling (ASL) and MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany for others). Three-dimensional T1 weighted imaging was acquired by rapid acquisition with a gradient echo sequence; TR=1700 msec; TE=2.61 msec; flip angle=10°; inversion time (TI)=800 msec; voxel size=1×1×1 mm; parallel acquisition technique=GRAPPA; and acceleration factor=2. ASL was acquired with TR=4521 msec; TE= 9.812 msec; field of view=24 cm; matrix size= 512×512); voxel size=1.88 x 1.88 x 4.0 mm3; number of slices=30; number of excitations=3; bandwidth=62.50 Hz; labelling time=1.5 sec; and post-labelling delay= 1525 msec3.
Image and statistical analysis
The presence of the postoperative development of extracranial arteries and the regression of white matter hyperintensity were visually assessed on magnetic resonance angiography and fluid-attenuated inversion recovery.
Using FreeSurfer version 6.0 (https://surfer.nmr.mgh.harvard.edu/), choroid plexus in the lateral ventricles, lateral ventricles, cerebral cortex, and white matter was automatically segmented and their volumes were recorded. The accuracy of region-of-interests (ROIs) was visually inspected and manually checked for quality. The choroid plexus ROIs were applied to ASL in each patient to calculate choroid plexus volume after manual correction if necessary.
Cortical perfusion was measured using a standard atlas of middle cerebral artery region4 after reverse normalization to each patient’s native space. As an index of cortical perfusion, we used spatial coefficient-of-variation (ASL-CoV) calculated as the standard deviation divided by the average value within the ROI3; as cortical hypoperfusion becomes more severe, ASL-CoV increases. We used ASL-CoV because ASL-CoV reflects hypoperfusion status more accurately compared to the average regional value that was affected by elongated arterial transit time in patients with moyamoya disease3.
Paired T-test was used to compare preoperative and postoperative volume and perfusion measured above.
Results
Fig.1 shows a representative case. All operated hemispheres revealed the development of extracranial arteries and anastomosis to cortical arteries, and five (33%) patients showed postoperative regression of white matter hyperintensity. The choroid plexus volume per patient was significantly reduced after the surgery (1.65 (0.55) ml vs. 1.52 (0.51) ml; Fig. 2). No significant postoperative difference was observed in the volumes of lateral ventricles, cerebral cortex, and white matter (P=0.44-0.67).Cortical ASL-CoV values significantly decreased after the surgery (1.27 (0.33) vs. 0.98 (0.25)). On the other hand, the choroid plexus perfusion remained unchanged (37.8 (17.9) vs. 40.3 (12.7) ml/min/100g; Fig. 2).
Discussion
In previous studies, choroid plexus perfusion has been increased in preoperative patients with moyamoya disease compared to normal controls and decreased after the revascularization surgery5, 6. Although we did not find perfusion changes, we found a significant decrease in choroid plexus volume after postoperative improvement of cortical perfusion.The increase of choroid plexus volume might be a compensatory mechanism to maintain neurofluid dynamics under cortical hypoperfusion. Under normal aging or Alzheimer’s disease pathology, choroid plexus volume increases and perfusion decreases, and these changes are regarded as degenerative changes of choroid plexus7. On the contrary, we observed a decrease in choroid plexus volume after revascularization to restore cortical hypoperfusion. In patients with moyamoya disease, previous studies have revealed an increased number of enlarged perivascular spaces8 and decreased diffusivity along the perivascular space9 under cortical hypoperfusion in patients with moyamoya disease. Under arterial stenoocclusive changes and cortical hypoperfusion, the activity of the glymphatic system10 and the intramural peri-arterial drainage system11 were disrupted, and the accumulation of waste deposits negatively affects neurofluid dynamics. Therefore, it is possible that the choroid plexus is hyperactivated and proliferated under cortical hypoperfusion to compensate for the decreased activities of other systems. After the revascularization surgery and restoration of cortical perfusion, the choroid plexus may shrink and return to normal function.
Further studies are necessary to investigate microstructural and functional changes that occur in the choroid plexus under chronic cortical hypoperfusion.
Acknowledgements
No acknowledgement found.References
1. Liu R, Zhang Z, Chen Y, et al.
Choroid plexus epithelium and its role in neurological diseases. Front Mol Neurosci 2022;15:949231
2. Ihara M, Yamamoto Y, Hattori Y, et al. Moyamoya disease:
diagnosis and interventions. The Lancet
Neurology 2022;21:747-758
3. Hara S, Tanaka Y, Inaji M, et al. Spatial coefficient of
variation of arterial spin labeling MRI for detecting hemodynamic disturbances
measured with (15)O-gas PET in patients with moyamoya disease. Neuroradiology 2022;64:675-684
4. Mutsaerts HJ, van Dalen JW, Heijtel DF, et al. Cerebral
Perfusion Measurements in Elderly with Hypertension Using Arterial Spin
Labeling. PLoS One 2015;10:e0133717
5. Johnson SE, McKnight CD, Lants SK, et al. Choroid plexus
perfusion and intracranial cerebrospinal fluid changes after angiogenesis. J Cereb Blood Flow Metab
2020;40:1658-1671
6. Johnson SE, McKnight CD, Jordan LC, et al. Choroid plexus
perfusion in sickle cell disease and moyamoya vasculopathy: Implications for
glymphatic flow. J Cereb Blood Flow Metab
2021;41:2699-2711
7. Eisma JJ, McKnight CD, Hett K, et al. Choroid plexus
perfusion and bulk cerebrospinal fluid flow across the adult lifespan. J Cereb Blood Flow Metab 2023;43:269-280
8. Kuribara T, Mikami T, Komatsu K, et al. Prevalence of and
risk factors for enlarged perivascular spaces in adult patients with moyamoya
disease. BMC Neurol 2017;17:149
9. Hara S, Kikuta J, Takabayashi K, et al. Diffusivity Along
the Perivascular Space is Decreased and Related to Hypoperfusion in Adult
Moyamoya disease. ResearchSquare 2023
10. Iliff JJ, Wang M, Zeppenfeld DM, et al. Cerebral arterial
pulsation drives paravascular CSF-interstitial fluid exchange in the murine
brain. J Neurosci 2013;33:18190-18199
11. Albargothy NJ, Johnston DA, MacGregor-Sharp M, et al.
Convective influx/glymphatic system: tracers injected into the CSF enter and
leave the brain along separate periarterial basement membrane pathways. Acta neuropathologica 2018;136:139-152
Figures
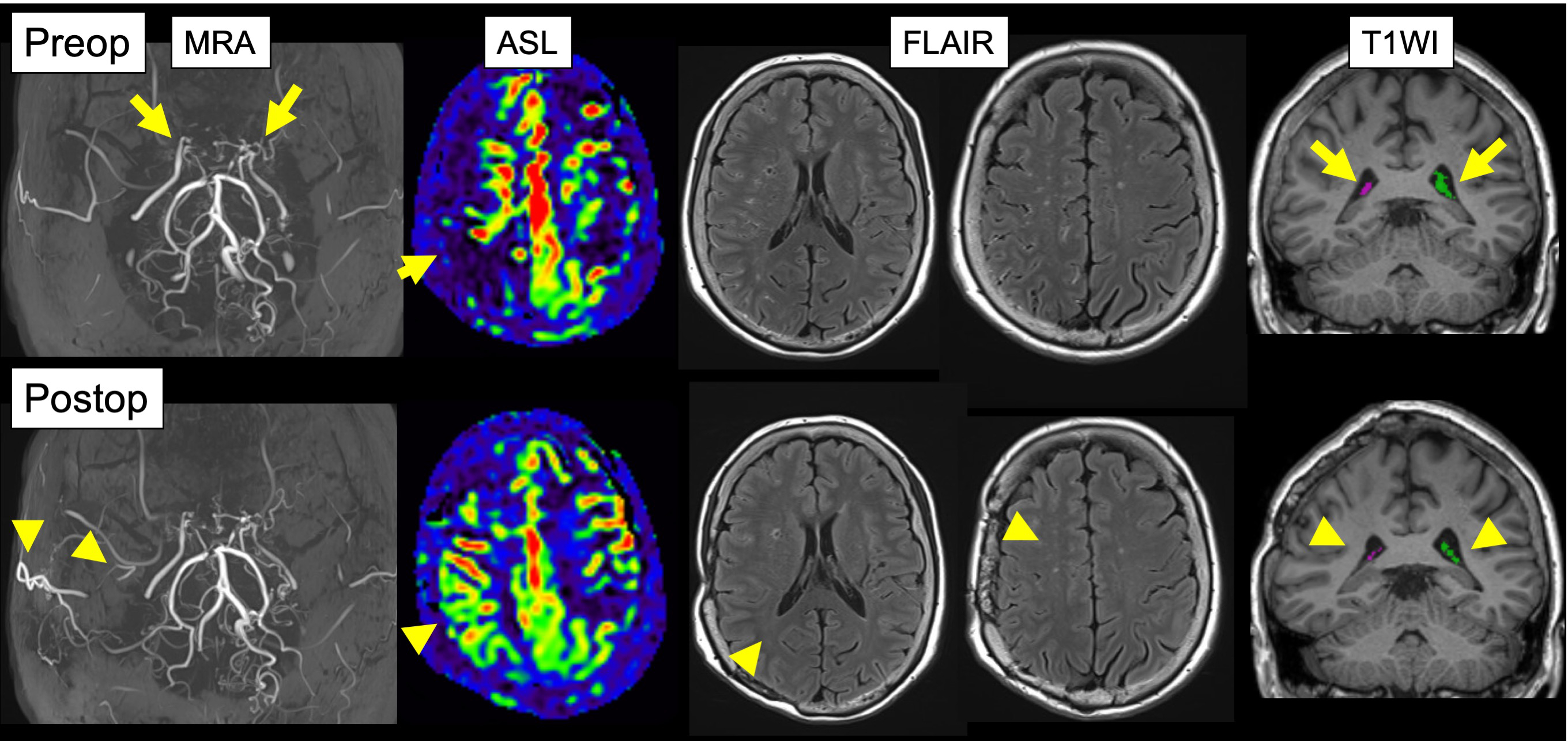
Figure 1. A 55-year-old female was treated with right-sided revascularization. One year after the surgery, anastomosis from the extracranial arteries have developed on magnetic resonance angiography (MRA), cortical hypoperfusion on arterial spin labeling (ASL) has improved, and some white matter hyperintensity on fluid attenuation inversion recovery (FLAIR) has disappeared. Compared to those before the surgery, choroid plexus segmented on T1 weighted images (T1WI) was small after the surgery.
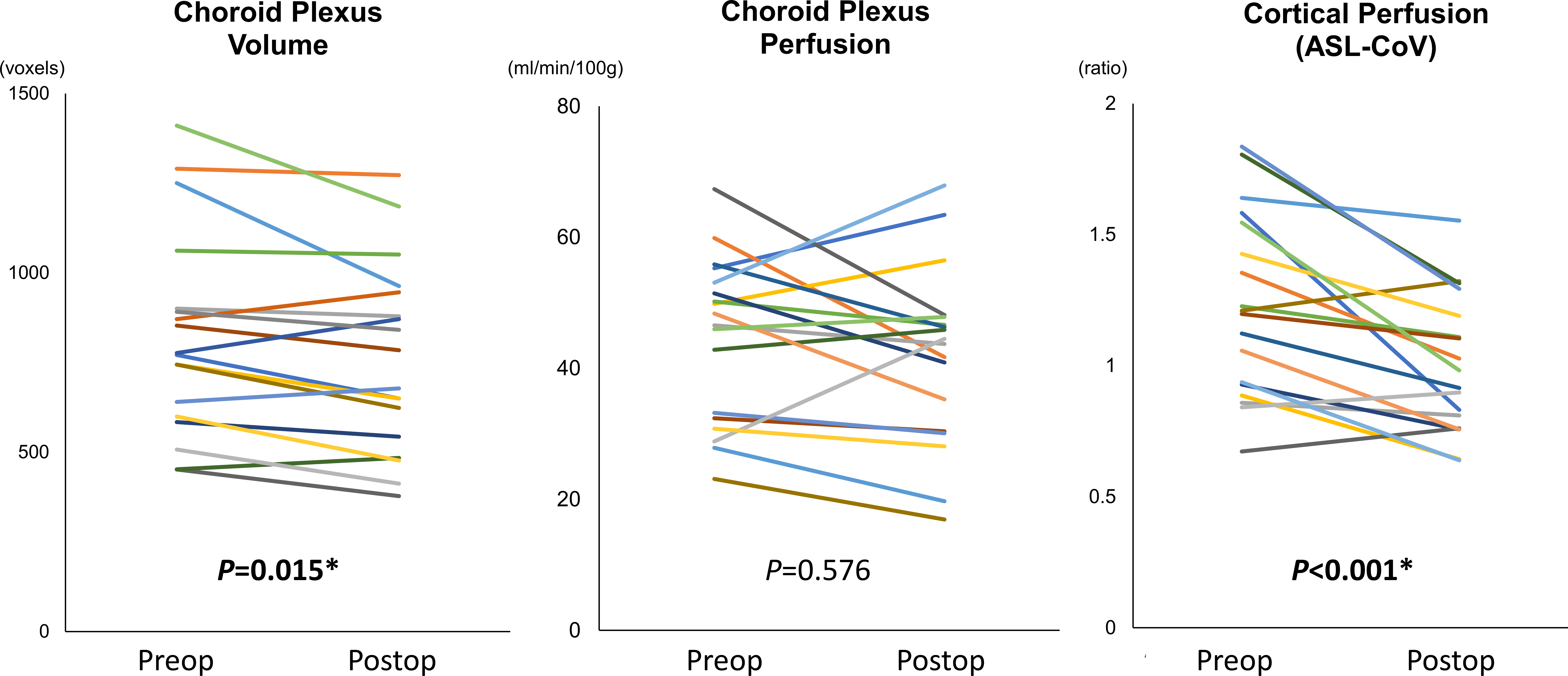
Figure 2. Preoperative and postoperative values of choroid plexus volume, perfusion, and cortical perfusion.
ASL-CoV, spatial coefficient-of-variation of arterial spin labeling MRI.
*P<0.05 (two-sided paired T-test)