0034
Cerebrovascular reactivity in choroid plexus1University of Maryland, Baltimore, Baltimore, MD, United States, 2University of Texas at Dallas, Richardson, TX, United States, 3Johns Hopkins University, Baltimore, MD, United States, 4University of Texas Southwestern Medical center, Dallas, TX, United States
Synopsis
Keywords: Neurofluids, Arterial spin labelling, Aging, Blood vessels, Neuro, Neurofluids, Perfusion, Vascular
Motivation: Choroid plexus (CP) plays an important role in the production of CSF and the formation of the blood-CSF barrier, but its vascular function is unclear.
Goal(s): We aim to quantify cerebrovascular reactivity (CVR) of CP in normal controls.
Approach: We applied PCASL with 5%CO2 inhalation in 92 subjects and compared CVR in gray matter, white matter and CP between young and old subjects.
Results: CVR of CP was significantly lower than that of gray and white matter, but showed no age-related difference.
Impact: This work provides a reference for future studies on CVR changes of CP in pathological conditions.
Introduction
Choroid plexus (CP) is a highly vascularized secretory tissue in the ventricles of the brain, which plays an important role in the production of brain cerebrospinal fluid (CSF) and the formation of the blood-CSF barrier1, 2. CSF production has also been linked to the recently discovered glymphatic waste clearance system of the brain3, which is thought to have a major role in neurodegenerative diseases such as the Alzheimer’s disease. Although our understanding of CP anatomy is increasing, little is known about the normal CP physiology which is critical in understanding CP function. Recently, arterial spin labeling (ASL) perfusion MRI has been suggested to be a potential non-invasive tool for the quantification of CP perfusion4, but the vasodilatory function of CP remains unclear. Therefore, in this study, we aim to use pseudo-continuous ASL with hypercapnia challenge to evaluate cerebrovascular reactivity (CVR), the dilatory function of blood vessels, in CP in a large cohort of healthy subjects and explore potential age differences.Methods
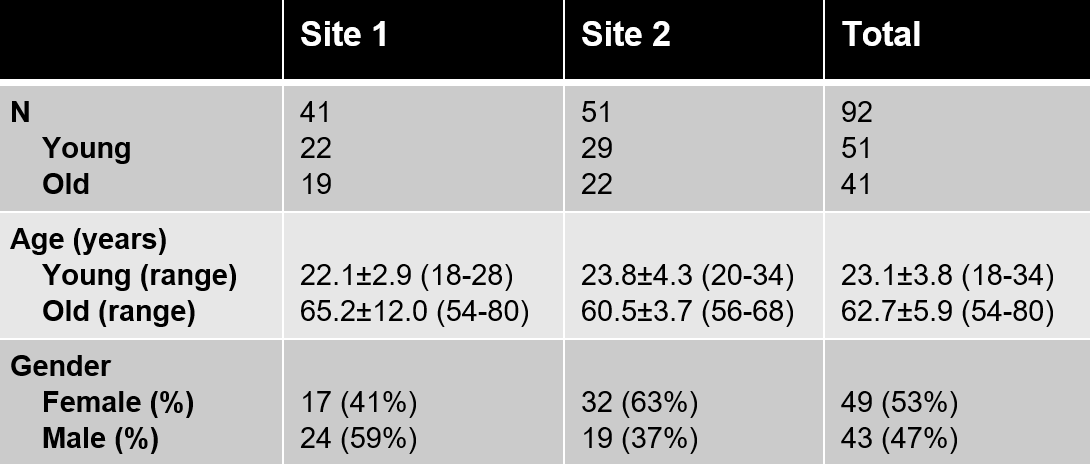
Participants:A total of 92 healthy participants were enrolled at two sites and studied on identical-model 3T Philips MRI scanners after IRB-approved informed consents were obtained. The participants were divided into the younger (N=51, 18-34 y.o.) and older (N=41, 54-80 y.o.) groups.
MRI:
The MRI session started with a 12-min breathing task during which the subjects wore a nose clip and mouthpiece inside the scanner and were administered room air for the first 5min followed by hypercapnia gas (5%CO2, 21%O2 and 74%N2) for the next 7min. During the breathing task, a 1-min phase-contrast (PC) MRI was performed first followed by a 10-min dual-echo ASL/BOLD sequence. At 4 min into the ASL/BOLD sequence the inspired gas was switched to hypercapnia gas stored in a Douglas bag. After the ASL/BOLD sequence, a second PC-MRI was performed in the hypercapnic state. End-tidal CO2 (EtCO2) was continuously measured through the duration of the experiment. The two PC-MRI scans (TR/TE/FA=20ms/7ms/15°, 0.7x1.2x5mm3 resolution, encoding velocity (Venc)=80 cm/s, 2D imaging slice parallel to AC-PC line at 20 mm above sinus confluence) were performed to measure blood flow through the superior sagittal sinus5. The dual-echo ASL/BOLD sequence used the following parameters: TR/TE1/TE2=4006/13/30ms, 3.44x3.44x6mm3 resolution, labeling duration=1400ms, post-labeling delay=1450-2010ms[HL1] )5. ASL data obtained from the first echo were used to quantify CBF in this study. A T1-MPRAGE scan (at 1x1x1mm3 resolution) was performed for tissue segmentation.
Data processing:
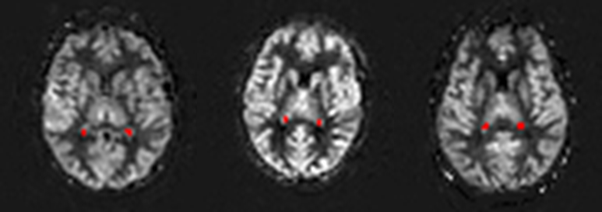
Following the procedure described previously6, CBF-weighted images were obtained from control and label images using surround subtraction and averaged for the first and last 4min to obtain CBF-weighted maps at room air and hypercapnia, respectively. Global flow values from PC-MRI were used to correct for individual differences in pCASL labeling efficiency during hypercapnia using procedures described previously7. Bilateral CP ROIs were manually drawn on the 10min-averaged CBF map of each subject (see Figure 1 for example). Gray and white matter ROIs were obtained by segmenting T1-MPRAGE images and then coregistered to the CBF maps. CVR was calculated as (CBFhypercapnia- CBFroom air)/ CBFroom airx100%/(EtCO2hypercapnia-EtCO2room air), and compared between the young and old groups after accounting for gender and site effects.
Results
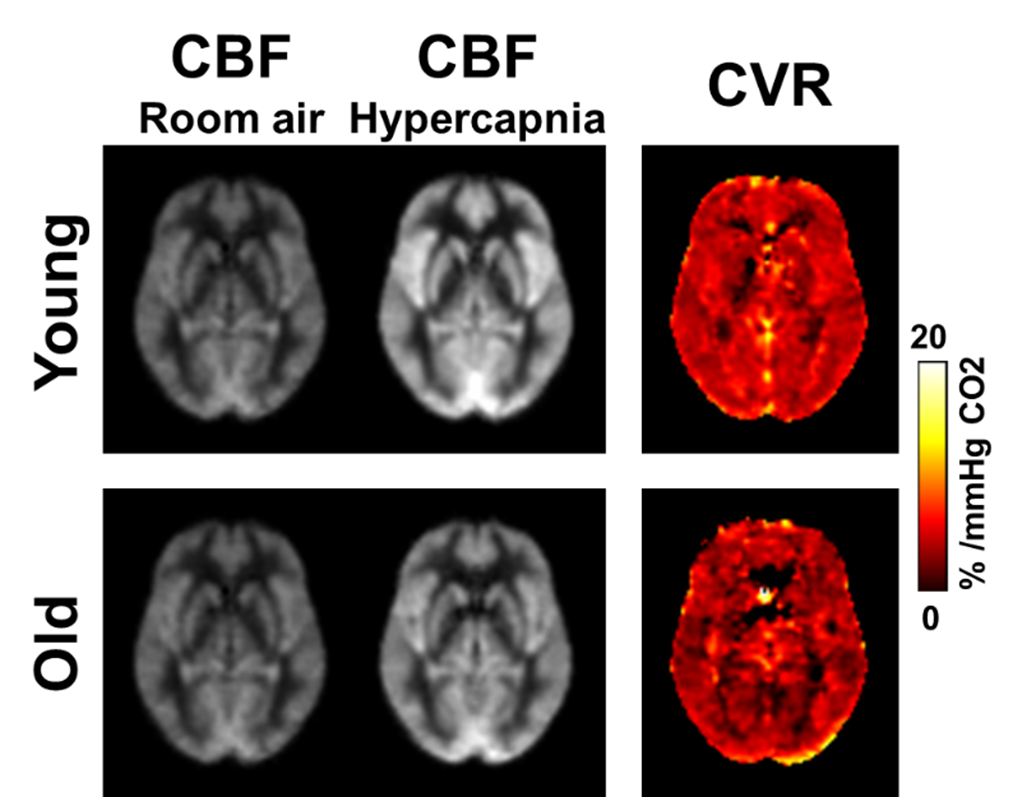
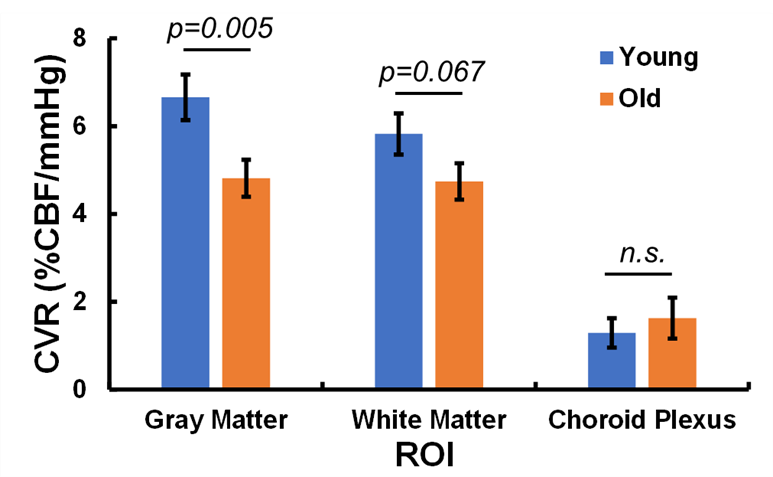
Table 1 summarizes the participant demographics of the two sites. Group-averaged CBF and CVR maps for younger and older subjects are shown in Figure 2. Visual inspection reveals lower CVR in the older subjects compared to the younger group, as expected. Figure 3 shows the CVR values of each ROI in both groups. The CVR of CP was 1.29±2.39%/mmHg and 1.63±2.98%/mmHg for the younger and older groups, respectively. This was significantly lower (p<0.0001) than the CVR in gray matter (6.66±3.69%/mmHg for young and 4.81±2.70%/mmHg for old) and white matter (5.82±3.36%/mmHg for younger and 4.74±2.63%/mmHg for older). Gray matter CVR was significantly different between younger and older (p=0.005) and white matter CVR also showed a trend of age-difference (p=0.068). We did not find age-related differences in CVR for CP (p=0.55).Discussion
To the best of our knowledge, this is the first report on absolute quantification of CVR in choroid plexus in a large cohort of normal controls. CVR in CP was found to be only about 20-30% of that in gray matter, consistent with the notion that CP vessels have no smooth muscle cells. No significant difference was found between younger and older subjects, suggesting that the vascular function in CP was likely preserved well during normal aging. This work may provide a reference for future studies on CVR changes of CP in pathological conditions such as neurodegenerative disease.Acknowledgements
No acknowledgement found.References
1. Emerich DF, Skinner SJ, Borlongan CV, Vasconcellos AV, Thanos CG. The choroid plexus in the rise, fall and repair of the brain. Bioessays 2005; 27(3): 262-74.
2. Christensen J, Li C, Mychasiuk R. Choroid plexus function in neurological homeostasis and disorders: The awakening of the circadian clocks and orexins. J Cereb Blood Flow Metab 2022; 42(7): 1163-1175.
3. Iliff JJ, Wang M, Liao Y, Plogg BA, Peng W, Gundersen GA, Benveniste H, Vates GE et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med 2012; 4(147): 147ra111.
4. Zhao L, Taso M, Dai W, Press DZ, Alsop DC. Non-invasive measurement of choroid plexus apparent blood flow with arterial spin labeling. Fluids Barriers CNS 2020; 17(1): 58.
5. Turner MP, Zhao Y, Abdelkarim D, Liu P, Spence JS, Hutchison JL, Sivakolundu DK, Thomas BP et al. Altered linear coupling between stimulus-evoked blood flow and oxygen metabolism in the aging human brain. Cereb Cortex 2022; 33(1): 135-151.
6. Hutchison JL, Lu H, Rypma B. Neural mechanisms of age-related slowing: the ΔCBF/ΔCMRO2 ratio mediates age-differences in BOLD signal and human performance. Cereb Cortex 2013; 23(10): 2337-46.
7. Aslan S, Xu F, Wang PL, Uh J, Yezhuvath US, van Osch M, Lu H. Estimation of labeling efficiency in pseudocontinuous arterial spin labeling. Magn Reson Med 2010; 63(3): 765-71.
Figures