0021
Integrated MRI radiomics, tumor microenvironment, and clinical risk factors improving survival prediction in patients with glioblastoma1Lanzhou University Second Hospital, Lanzhou, China
Synopsis
Keywords: Tumors (Post-Treatment), Neuro
Motivation: The patients with glioblastoma (Gb) with poor prognosis and quality of life.
Goal(s): To construct a comprehensive model for predicting the prognosis of patients with Gb using a radiomics method and integrating tumor microenvironment .
Approach: In total, 149 patients with isocitrate dehydrogenase wild-type Gb were enrolled retrospectively. Selected the best feature combination related to Gb overall survival. Clinical-radiomics-TME models were established.
Results: Lasso-Cox analyses were used to screen the factors related to OS in patients with Gb, including age, peritumoral edema, tumor purity, tumor-associated macrophages, and the 21 radiomics features. The clinical-radiomics-TME model had the best survival prediction ability, the C-indices was 0.727.
Impact: Considering the poor prognosis of IDH wild-type Gb, we explored additional prognostic risk factors and established a survival prediction model. The clinical-radiomics-TME comprehensive model showed a significant improvement compared to other models and was most effective in predicting patient survival.
Introduction
Glioblastoma (Gb) is the most common primary malignant tumor of the brain, the incidence of Gb is 3.26/100000[1]. The newly released WHO CNS tumor classification system, IDH wild-type Gb is WHO grade 4[2]. The 1-year and 2-year survival rate of Gb is less than 40% and 18%, respectively[3]. Most patients relapse within 10-12 months after the initial diagnosis and treatment, with poor prognosis and quality of life[4]. Clinicians monitor patients with varying risk levels by exploring the components and functions of the Gb tumor microenvironment (TME), identifying reliable and independent prognostic factors.The main prognostic factors included age, Karnofsky Performance Status score, the extent of surgical resection, and WHO grade, among others[5]. Tumor purity (TP) is defined as the percentage of tumor cells in solid tumor samples[6]. Additionally, the prognosis of tumors also correlation to non-tumor cells, especially the degree of immune cell infiltration[7]. In Gb tissues, TAMs are the most abundant immune cells. M2 phenotype TAMs play a dominant role in the immune microenvironment of gliomas. CD163 is a reliable marker of M2 macrophages and has been used to evaluate the infiltration of M2 macrophages into various tumors[8].Image-based radiomics features are highly specific and non-invasive and can evaluate the spatial heterogeneity, microenvironment, and biological function of tumors. These features can improve the accuracy of diagnosis and prognosis[9]. Digital pathology is a new method for predicting the survival of patients with gliomas [10]. MRI-based radiomics and pathomics complement each other in evaluating tumor heterogeneity. Therefore, this study aimed to construct a robust predictive model to analyze the prognosis of patients with IDH wild-type Gb by integrating clinical factors, TP and TAMs, and radiomic features.Methods
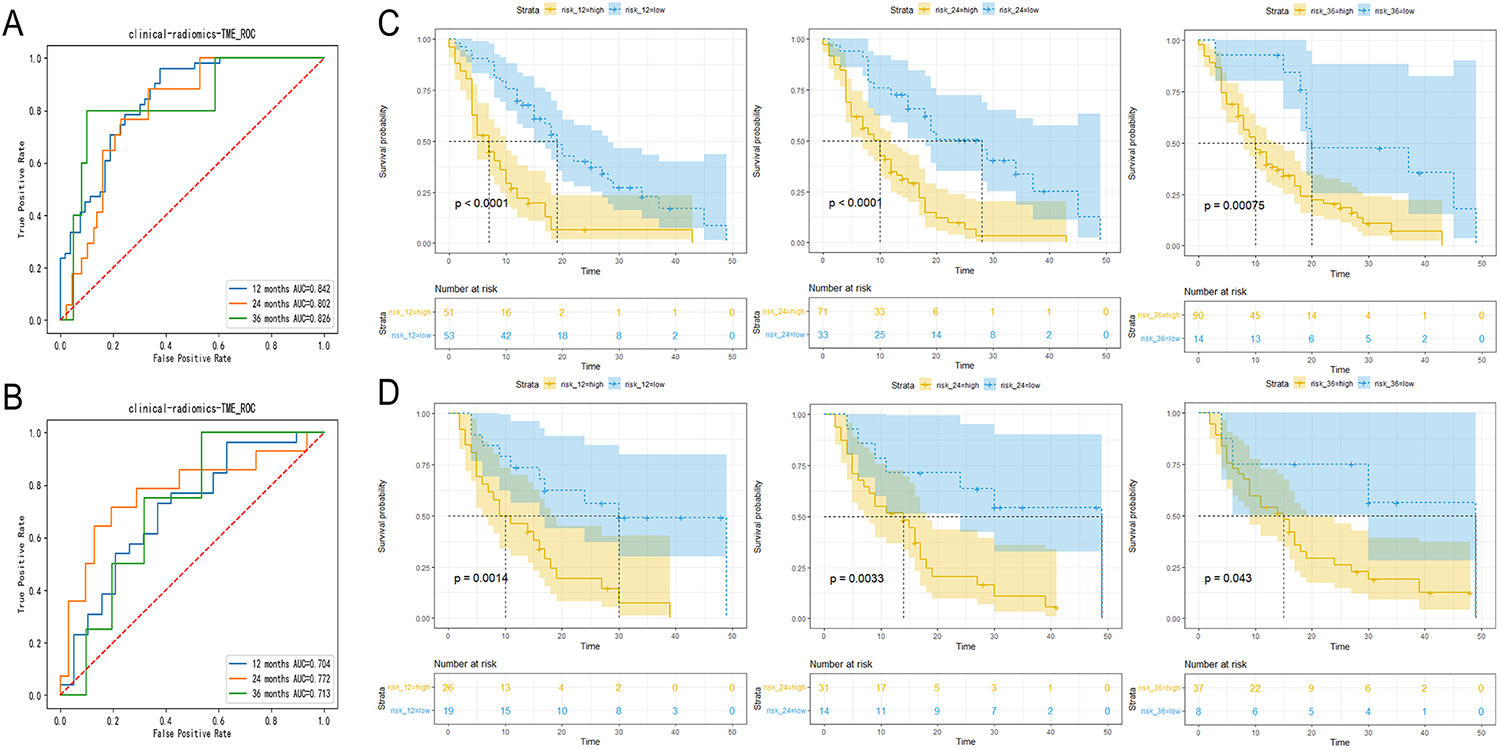
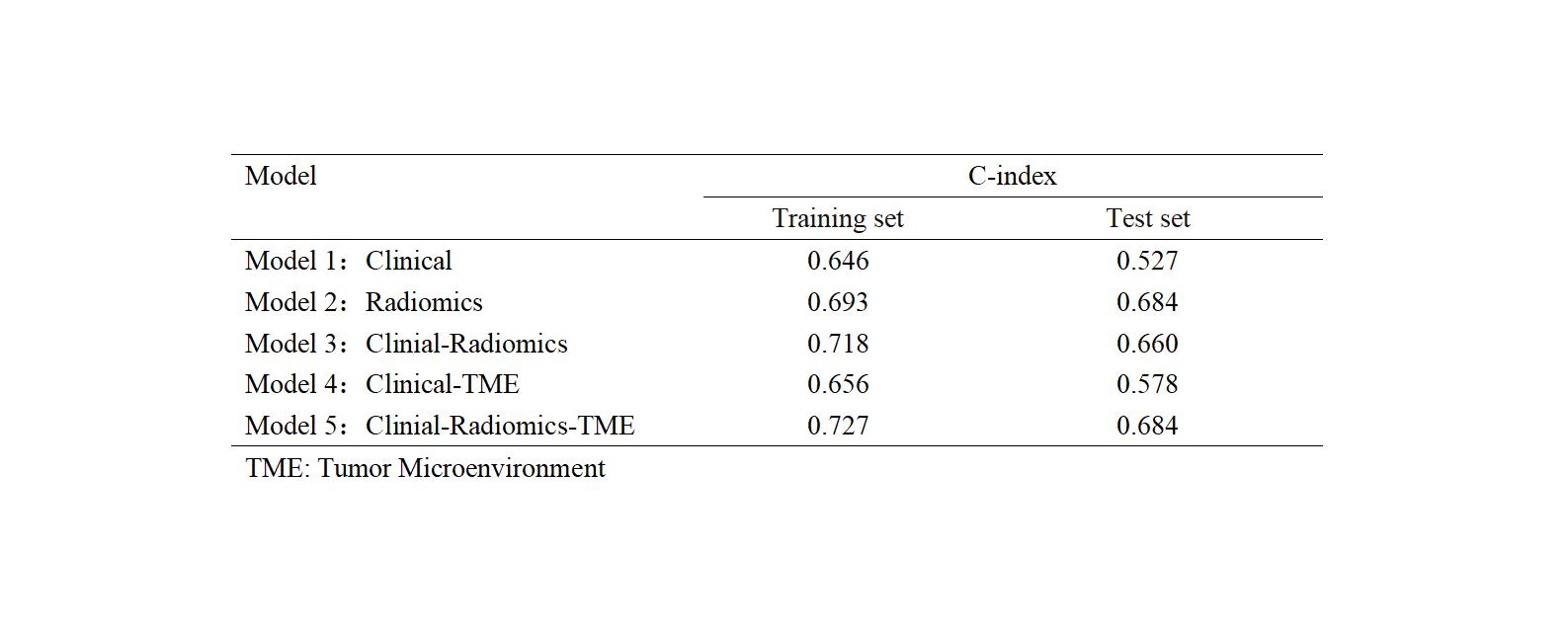
149 patients with isocitrate dehydrogenase (IDH) wild-type Gb were enrolled retrospectively. They were randomly divided into the training (n=104) and test (n=45) sets. We selected the best feature combination related to Gb overall survival (OS) using Lasso-Cox regression analyses. Clinical, radiomics, clinical-radiomics, clinical-TME, and clinical-radiomics-TME models were established. The models’ concordance index (C-index) were evaluated. Survival curve was drawn using Kaplan–Meier method, and the prognostic stratification ability of the model was tested.Results
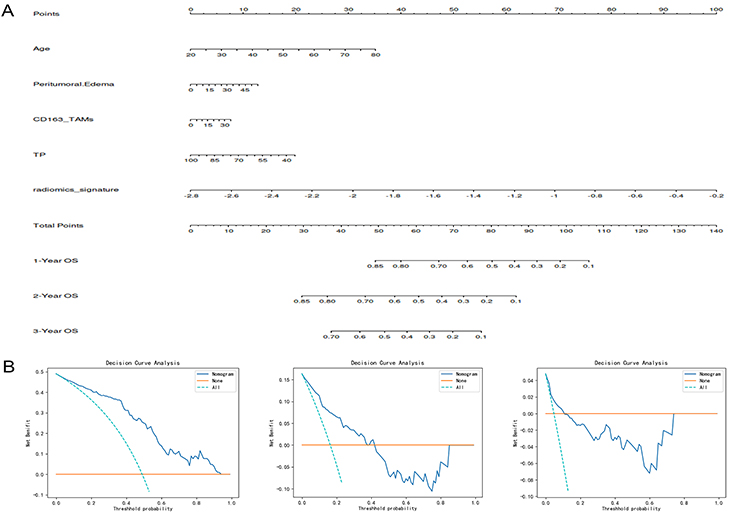
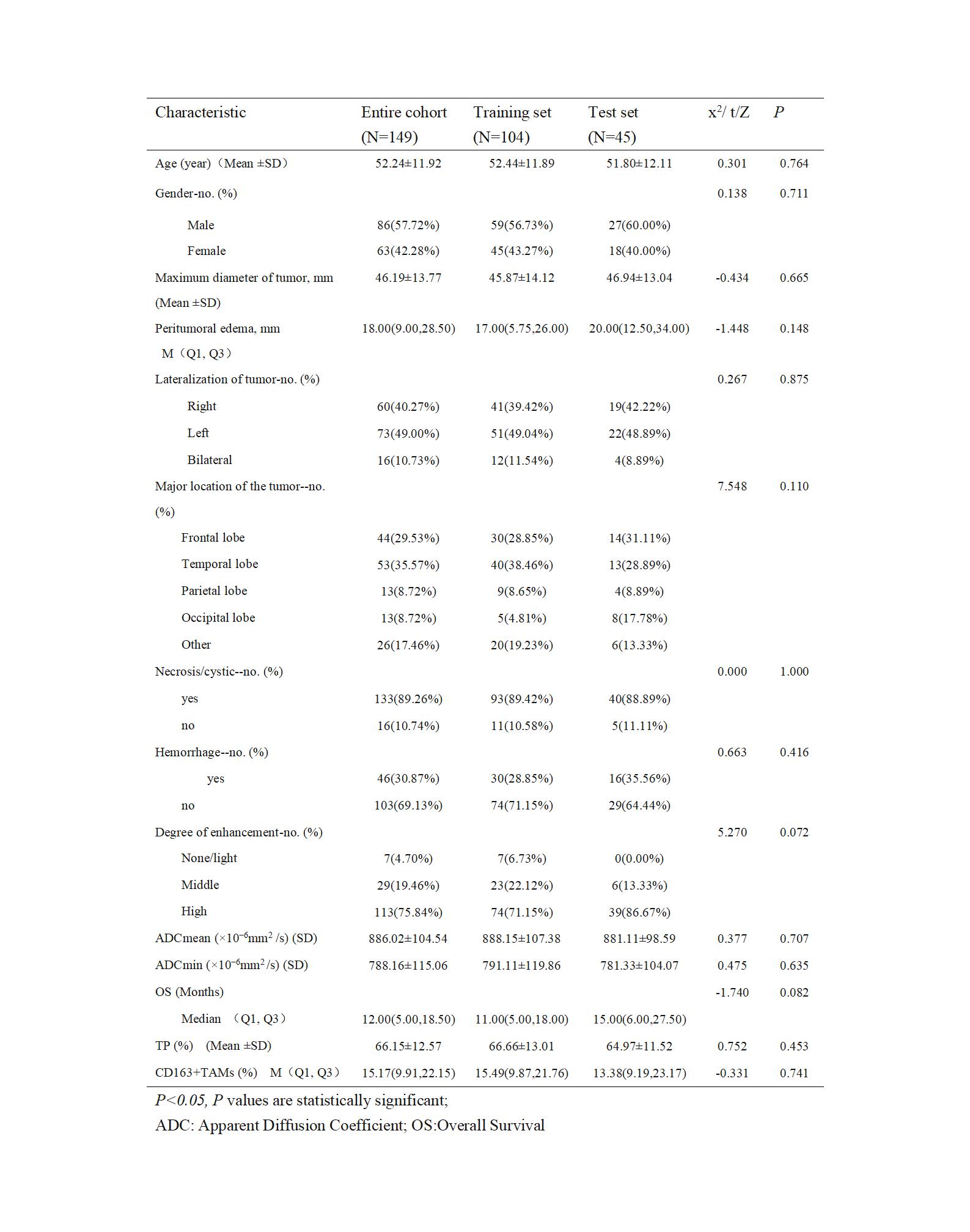
In total, 149 patients, included 86 males and 63 females, mean age, 52.24 ±11.92 years(Table 1). Lasso-Cox analyses were used to screen the factors related to OS in patients with Gb, including age (Hazard ratio (HR)=1.021; 95% CI, 1.004-1.038; P=0.018), peritumoral edema (HR=1.015; 95% CI, 1.003-1.027; P=0.012), tumor purity(TP) (HR=0.978; 95% CI, 0.963-0.993; P=0.003), tumor-associated macrophages (TAMs) (HR=1.027; 95% CI, 1.003-1.052; P=0.024), and the 21 radiomics features. The clinical-radiomics-TME model had the best survival prediction ability(Fig.1), and the C-indices was 0.727. The AUC of 1-Year, 2-Year, and 3-Year OS prediction in the training set was 0.842, 0.802, and 0.826, respectively(Fig. 2).Discussion
We integrated clinical imaging factors (including age and peritumoral edema), 21 radiomics features, and TP and CD163+ TAMs to establish a prognostic prediction model. The comprehensive clinical-radiomics-TME model performed the best (C-index, 0.727).Further comparison between models showed that the efficiency of the model was improved.First, we found that age and peritumoral edema were significantly correlated with OS in patients with Gb, can be used as predictors of Gb survival. And our study temporal lobe tumors were found to be the most common, the tumor location may be a po tential prognostic factor. Glioma infiltration on high b-value DWI is an independent predictor of poor prognosis in glioma patients[11].Low ADCmin predicted a poor prognosis compared with high ADCmin[12]. Our study analyzed the ADCmean and ADCmin values; We believe that DWI has the potential to be used for survival prediction.It has been shown that the radiomics features are related to the OS of Gb.[13].In our study, 21 radiomics features extracted and selected from T2WI and CE-T1WI sequences were fused, and a radiomics model was established, which were better than those of the clinical model. The radiomics model was able to categorize patients with Gb into high- and low-risk groups with good survival stratification.We quantitatively analyzed the expression of TP and M2 phenotype TAMs in Gb based on WSI and added them as prognostic risk factors in Gb to construct a prognostic model. Demonstrating the feasibility of the quantitative evaluation of CD163. CD163+ TAMs are independent and clinically valuable prognostic biomarkers for HGG. Our comprehensive model combined different levels of multidimensional information. The results revealed that the clinical-radiomics-TME model performed best among all models. In similar studies, clinical models, genetic models, radiomics models, and combined models were established to predict the OS of Gb[14], and it was found that multivariate combined models improved prognosis prediction.Conclusions
The clinical-radiomics-TME comprehensive model showed a significant improvement compared to other models and was most effective in predicting patient survival. Additionally, the radiomic features, TP, and TAMs play major roles in predicting the survival of patients with Gb.Acknowledgements
This work was supported by National Natural Science Foundation of China (grant number 82071872, 82371914 ); Science and Technology Program of Gansu Province (grant number 21YF5FA123); China International Medical Foundation (grant number Z-2014-07-2101).References
1 Ostrom QT, Price M, Neff C, Cioffi G, Waite KA, Kruchko C, et al. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015-2019. Neuro Oncol 2022;24(Suppl 5):v1-v95.2 Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol 2021;23(8):1231-1251. 3 Janjua TI, Rewatkar P, Ahmed-Cox A, Saeed I, Mansfeld FM, Kulshreshtha R, et al. Frontiers in the treatment of glioblastoma: Past, present and emerging. Adv Drug Deliv Rev 2021;171:108-138.4 Mallick S, Benson R, Hakim A, Rath GK. Management of glioblastoma after recurrence: A changing paradigm. J Egypt Natl Canc Inst 2016;28(4):199-210.5 Chen H, Li C, Zheng L, Lu W, Li Y, Wei Q. A machine learning-based survival prediction model of high grade glioma by integration of clinical and dose-volume histogram parameters. Cancer Med 2021;10(8):2774-2786.6 Qin Y, Feng H, Chen M, Wu H, Zheng X. InfiniumPurify: An R package for estimating and accounting for tumor purity in cancer methylation research. Genes Dis 2018;5(1):43-45.7 Wang XX, Cao H, Zhai Y, Deng SZ, Chao M, Hu Y, et al. Immune Gene Signatures and Immunotypes in Immune Microenvironment Are Associated With Glioma Prognose. Front Immunol 2022;13:823910.8 Skytthe MK, Graversen JH, Moestrup SK. Targeting of CD163(+) Macrophages in Inflammatory and Malignant Diseases. Int J Mol Sci 2020;21(15).9 Tan Y, Mu W, Wang XC, Yang GQ, Gillies RJ, Zhang H. Improving survival prediction of high-grade glioma via machine learning techniques based on MRI radiomic, genetic and clinical risk factors. Eur J Radiol 2019;120:108609.10 Zhao R, Krauze AV. Survival Prediction in Gliomas: Current State and Novel Approaches. 2021.11 Zeng Q, Ling C, Shi F, Dong F, Jiang B, Zhang J. Glioma infiltration sign on high b-value diffusion-weighted imaging in gliomas and its prognostic value. J Magn Reson Imaging 2018.12 Qin L, Li A, Qu J, Reinshagen K, Li X, Cheng SC, et al. Normalization of ADC does not improve correlation with overall survival in patients with high-grade glioma (HGG). J Neurooncol 2018;137(2):313-319.13 Sun Q, Chen Y, Liang C, Zhao Y, Lv X, Zou Y, et al. Biologic Pathways Underlying Prognostic Radiomics Phenotypes from Paired MRI and RNA Sequencing in Glioblastoma. Radiology 2021;301(3):654-663.14 Choi Y, Nam Y, Jang J, Shin NY, Lee YS, Ahn KJ, et al. Radiomics may increase the prognostic value for survival in glioblastoma patients when combined with conventional clinical and genetic prognostic models. Eur Radiol 2021;31(4):2084-2093.Figures