0020
Radio-pathomic signatures within and beyond FLAIR hyperintensity predict prognosis in glioblastoma following gross total resection1Biophysics, Medical College of Wisconsin, Milwaukee, WI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, glioma, neuro-oncology
Motivation: Glioblastoma (GBM), a highly lethal brain tumor, poses a significant threat to patient survival, even after gross total resection (GTR).
Goal(s): This study explored whether radio-pathomic features from autopsy-trained models could predict survival in GTR-treated GBM patients.
Approach: The relationship between cell density and tumor probability (TPM) beyond the FLAIR hyperintense (FH) region, as well as a habitat-based labeling within FH was investigated. Cox regressions evaluated the impact of habitat volume and radio-pathomic characteristics within FH on survival.
Results: The study revealed that radio-pathomic features of FH predicted overall survival, suggesting the ability to identify infiltrative tumor ultimately missed by surgery.
Impact: In GTR-treated GBM patients, the presence of infiltrative tumor cells within and beyond FLAIR hyperintensity may predict patient prognosis and could be used for optimizing treatment.
Introduction
Glioblastoma (GBM) is a highly aggressive, heterogenous primary brain tumor with a median overall survival (OS) of 14-20 months (1). Gross total resection (GTR), the complete resection of contrast enhancing tumor on MRI, has been shown to increase survival outcomes; however, eventual recurrence and patient death ultimately occur (2). Autopsy studies have previously found tumor beyond the primary T1 enhancement and FLAIR hyperintense (FH) region, which may impact patient prognosis. Previously published radio-pathomic maps of tumor probability (TPM), using autopsy tissue aligned to imaging as ground truth, have been successful at identifying areas of non-enhancing tumor missed by surgery (3). Therefore, this study tested the hypothesis that radio-pathomic features, derived from autopsy-based tissue trained models, could predict prognosis for GBM patients following a GTR. We additionally tested the hypothesis that these features outside of the FH region on pre-surgical MRI would be associated with a worse OS in GBM patients following GTR.Methods
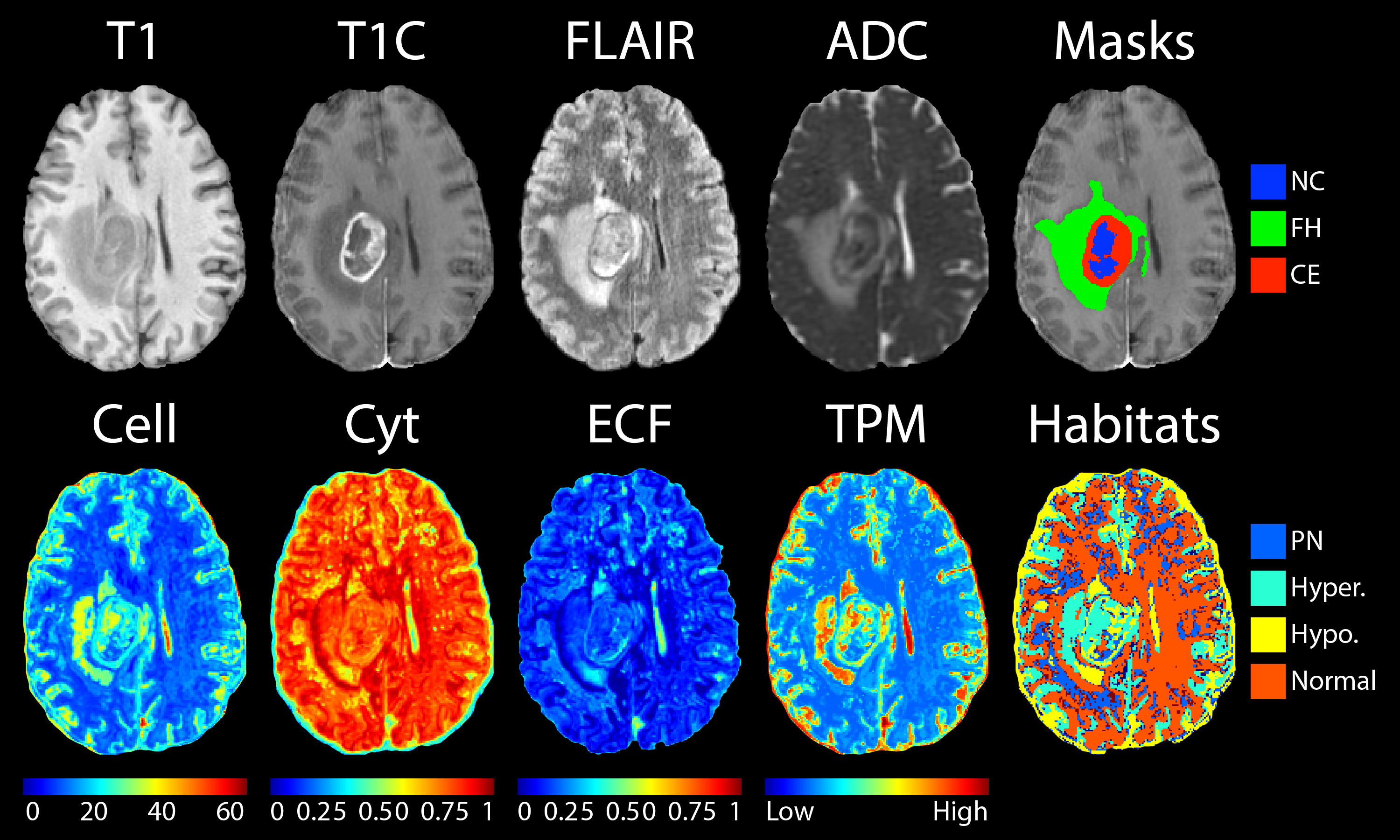
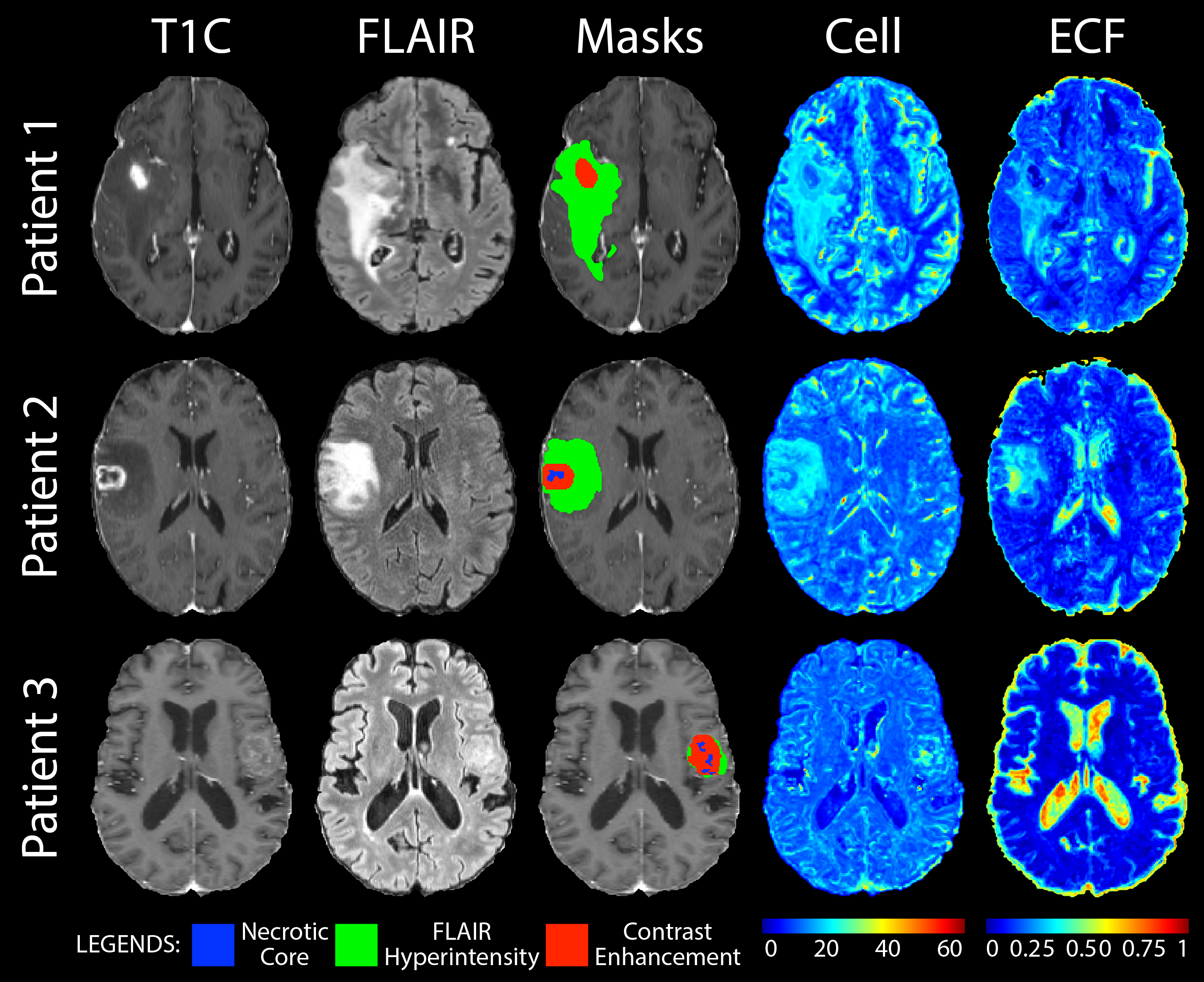
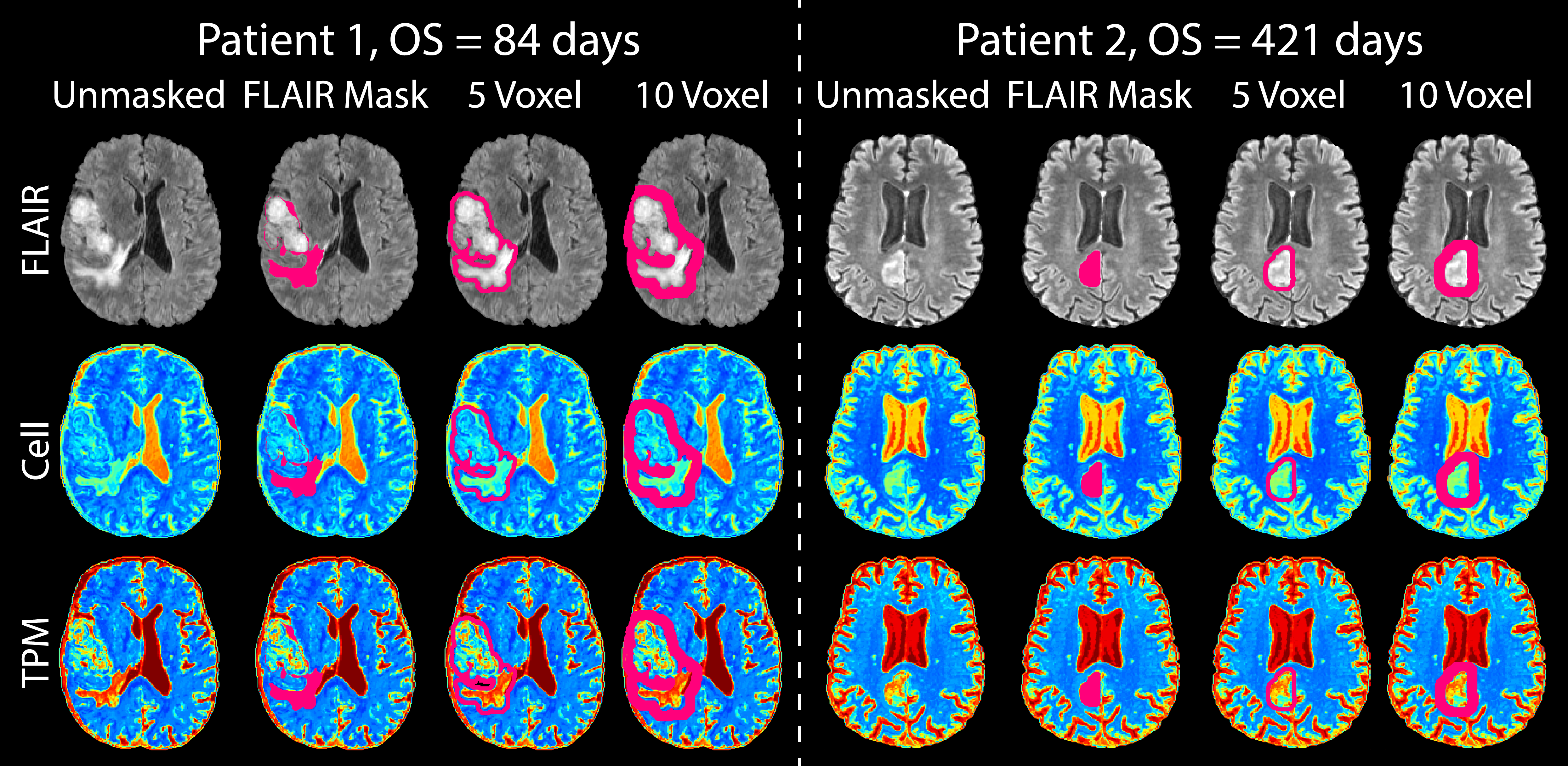
The publicly available UCSF-PDGM (4) dataset was analyzed for this study. Inclusion criteria were GBM patients who underwent GTR, resulting in a total of 218 patients (n = 92 female, mean age 62 ± 11.7 years). All patients were IDH-wildtype. Radio-pathomic maps of cell density (Cell), extracellular fluid (ECF), and tumor probability (TPM) were generated using pre-surgical T1, T1C, FLAIR, and ADC images as input to a previously published autopsy tissue trained model (4) (Figure 1). A habitat-based approach was used to create binary maps by categorizing voxel intensities in the ECF and Cell maps using manually defined cutoff values. A hypercellular habitat was defined as having a cellularity >1,900 cells/mm2 and an ECF density <0.25; conversely, a hypocellular habitat was defined as having a cellularity <1,800 cells/mm2 and an ECF density >0.25. Pseudo-palisading necrosis (PN) habitat was defined as having a cellularity >1,900 cells/mm2 and an ECF density >0.25. Voxels that were unable to classify into one of these habitats were considered normal tissue (Figure 2). These thresholds created an equal split of patients between each habitat group. Volumes of these thresholded maps were calculated within annotated tumor regions provided in the dataset, including contrast enhancement (CE) and FH. To test the association of Cell and TPM outside of FH, the FH mask was dilated by 5 and 10 voxels, and the original mask and ventricles were subtracted. Mean intensity within the original and dilated masks was calculated for regions of the masks within the brain (i.e., excluding dilation masks extending outside of the brain) (Figure 3). Cox proportional hazards models were used to assess the impact of high or low habitat volume via median split, as well as the association of Cell and TPM outside FH, on survival. Kaplan-Meier curves were additionally plotted to visualize survival differences (Figure 4).Results
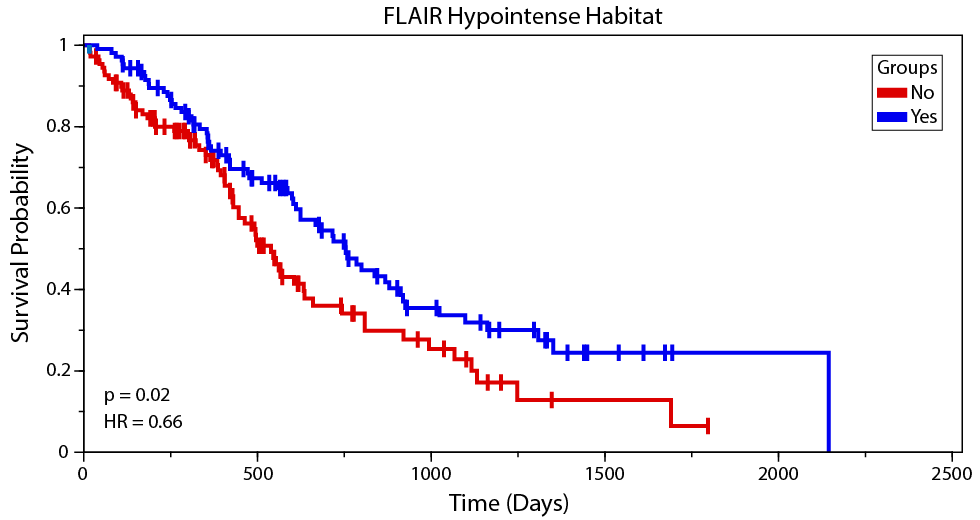
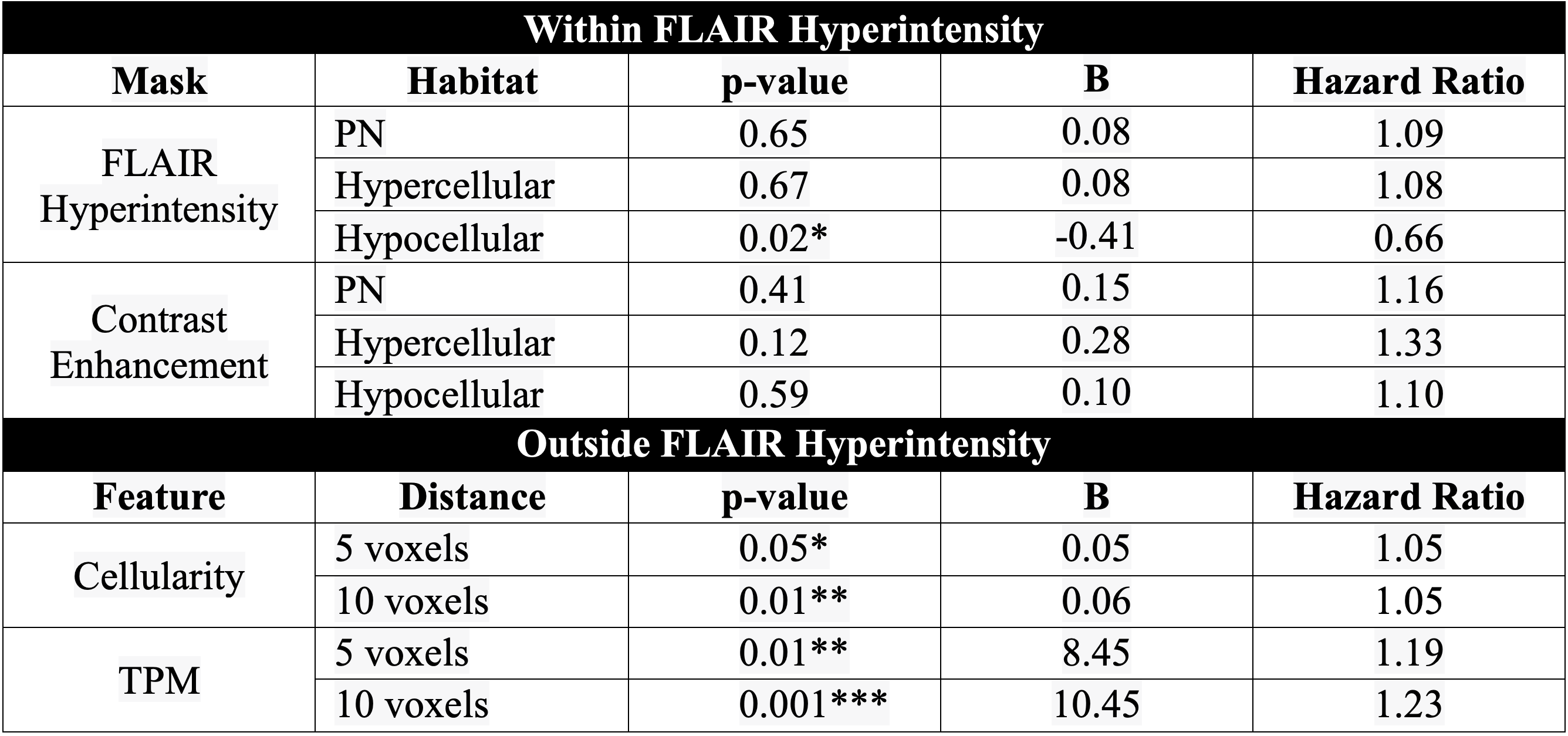
Within contrast enhancement, no significant trends were found across the three habitats (i.e., hypercellular, hypocellular, or PH). In FLAIR, however, hypocellular habitat volume was found to be significantly associated with worse OS (HR=0.66, p = 0.02). Outside of FH, an increased TPM was associated with poorer OS at both 5 and 10 voxels outside of FH (HR=1.19, p=0.01; HR=1.23, p=0.001, respectively). Likewise, at 5 and 10 voxels outside of FH, elevated cell density was associated with worse OS (HR=1.05, p=0.05; HR=1.18, p=0.01, respectively).Discussion
These results suggest that radio-pathomic habitats may provide additional information about patient survival, specifically hypocellular habitat volume within FH, suggestive of necrosis. Additionally, we found that radio-pathomic features calculated outside the margins of FH are associated with a poor prognostic outcome in GBM patients undergoing GTR. Together, these results suggest potential indicators of patient survival after GTR may lie within and around flair hyperintensity. Future research is warranted to better delineate tumor boundaries to increase tumor resection and thus improve survival outcomes (Table 1).Conclusion
This study demonstrated that in a cohort of 218 GBM patients undergoing GTR, pre-surgical cell density within and around FLAIR hyperintensity may allude to survival outcomes. Specifically, hypointense volume within and increased cellularity and tumor probability around FH are associated with worse patient prognosis.Acknowledgements
No acknowledgement found.References
1. Ostrom QT, Shoaf ML, Cioffi G, et al. National-level overall survival patterns for molecularly-defined diffuse glioma types in the United States. Neuro Oncol 2023;25:799-807
2. Revilla-Pacheco F, Rodríguez-Salgado P, Barrera-Ramírez M, et al. Extent of resection and survival in patients with glioblastoma multiforme: Systematic review and meta-analysis. Medicine (Baltimore) 2021;100:e26432
3. Bobholz SA, Lowman AK, Brehler M, et al. Radio-Pathomic Maps of Cell Density Identify Brain Tumor Invasion beyond Traditional MRI-Defined Margins. AJNR Am J Neuroradiol 2022;43:682-688
4. Bobholz SA, Lowman AK, Connelly JM, et al. Non-invasive tumor probability maps developed using autopsy tissue identify novel areas of tumor beyond the imaging-defined margin. medRxiv 2022
Figures