0018
Automatic Infiltration Risk Prior Generation with Modified Triplet Loss for Pre-Operative Glioblastoma Infiltration Prediction1Department of Biomedical Engineering, Case Western Reserve University, Cleveland, OH, United States, 2Department of Radiology, University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 3Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, United States, 4Department of Bioengineering, Santa Clara University, Santa Clara, OH, United States, 5Center for Data Driven Discovery in Biomedicine, Children's Hospital of Pennsylvania, Philadelphia, OH, United States, 6Center for Biomedical Image Computing and Analytics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, OH, United States, 7Department of Pathology, University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 8Piedmont Physicians Neurosurgery Atlanta, Piedmont Healthcare, Atlanta, GA, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, Glioblastoma
Motivation: Pre-operative glioblastoma (GBM) infiltration prediction models rely on manual infiltration risk (IR) prior segmentation which is tedious, requires expert input, and is highly variable.
Goal(s): Automation is needed for fast segmentation. A data-driven method would account for GBM heterogeneity and be independent of specific MRI input for applicability to clinical protocols.
Approach: IR priors are grown using modified triplet loss with inter-prior and intra-prior terms to ensure priors are distinct from each other and maintain similarity within individual priors.
Results: TripleSeq generated more consistent IR priors compared to manual segmentation. TripleSeq-trained models showed good classification (> 85% mean accuracy) of ground truth infiltration.
Impact: Glioblastoma (GBM) infiltration inevitably leads to tumor recurrence and progression. We introduce an automatic method to generate infiltration risk priors for improved GBM infiltration machine learning prediction, which applied pre-operatively can identify at-risk peritumoral regions for targeted neurosurgery and radiotherapy.
Introduction
To supplement limited pathological ground truth data, MRI-based machine learning (ML) models for pre-operative glioblastoma (GBM) infiltration prediction often train on domain knowledge metrics like distance1–4. However, such approaches often involve manual segmentation which is tedious, requires expert input, and is highly variable. To address these drawbacks, we introduce a triplet loss5-based segmentation method termed TripleSeq to automatically derive infiltration risk (IR) priors as surrogate for ground truth. TripleSeq iteratively searches the peritumoral region to identify candidate ROIs with high and low similarity to enhancing tumor (ET) image data: it is fully data-driven and does not require specific MRI contrasts or image sequences as input. This makes TripleSeq suitable for automatic generation of IR priors from multiparametric MRI (mpMRI) data. Here, we introduce the conceptual basis for TripleSeq and evaluate its application in mpMRI with MR fingerprinting6 (MRF) radiomics for GBM infiltration prediction.Theory
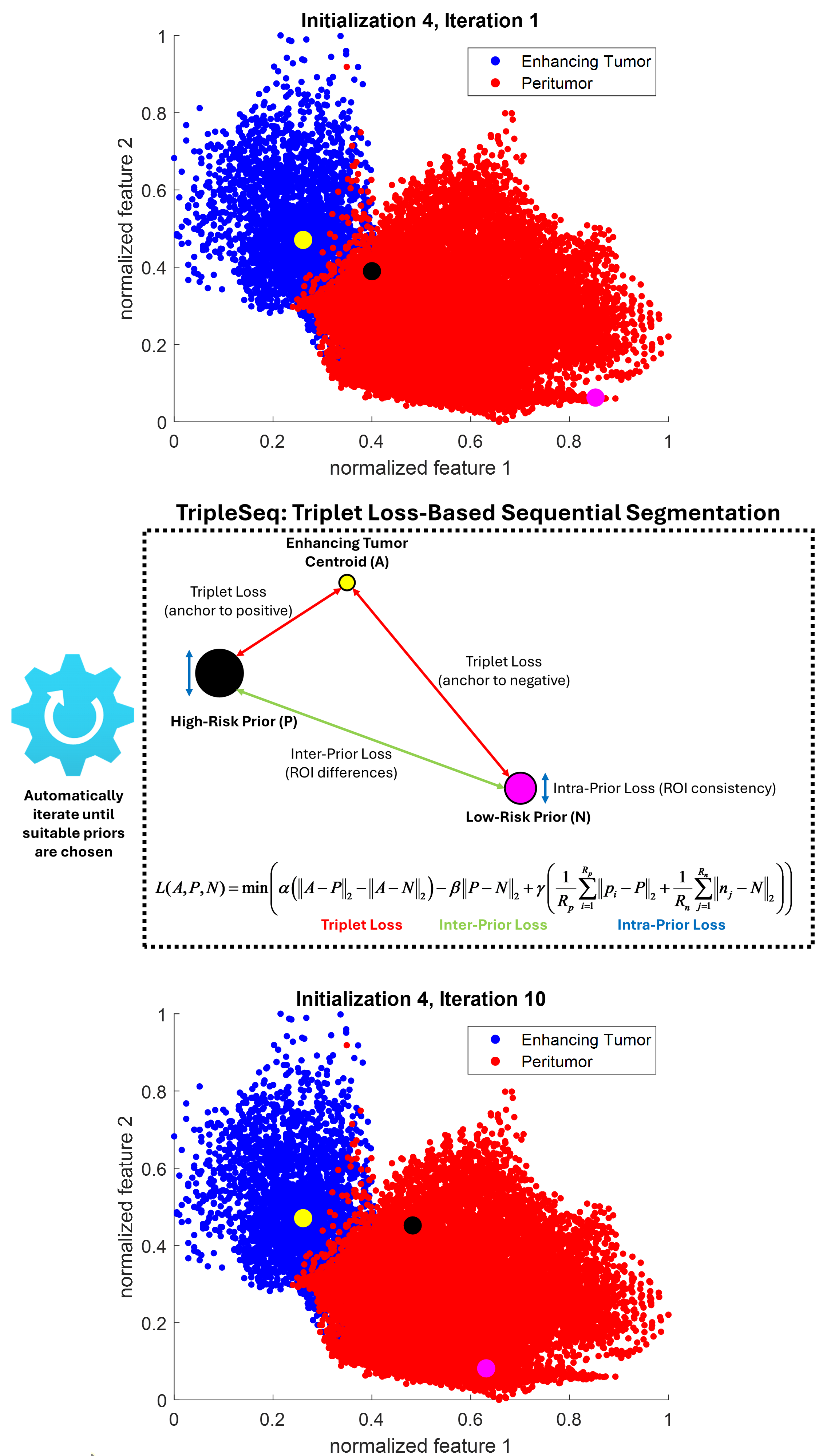
An ideal imaging biomarker7 for GBM infiltration should be consistently different between enhancing tumor (ET) and peritumor8 without infiltration. Furthermore, a monotonic trend should exist for peritumor with intermediate infiltrative potential, with high-risk regions having similar image features to ET and low-risk areas being dissimilar to ET.Triplet loss-based sequential segmentation (TripleSeq) employs this assumption to automatically identify IR priors (Figure 1). Following whole tumor segmentation, mpMRI data is projected voxel-wise into a high-dimensional image feature space (each dimension is a voxel-wise feature like T1w intensity) to identify the characteristic ET feature vector centroid $$$A$$$. The peritumor1,8,9 ROI (marginal area surrounding tumor core) is iteratively searched using a triplet loss, using characteristic ET feature vector $$$A$$$ as anchor and candidate high-risk $$$P$$$ and low-risk $$$N$$$ feature vectors as positive and negative inputs respectively. Following selection of high- and low-risk seeds, region growing is performed with a modified triplet loss:
$$L(A,P,N)=min(\alpha(\left\|A-P\right\|_{2}-\left\|A-N\right\|_{2})-\beta\left\|P-N\right\|_{2}+\gamma(\frac{1}{R_{p}}\sum_{i=1}^{R_{p}}\left\|p_{i}-P\right\|_{2}+\frac{1}{R_{n}}\sum_{j=1}^{R_{n}}\left\|n_{j}-N\right\|_{2}))$$
In addition to standard minimization between anchor (ET) and positive input (high-risk prior) and maximization between anchor and negative input (low-risk prior), the triplet loss is modified with k-means10 inspired metrics to include inter-prior ($$$\left\|P-N\right\|_{2}$$$; distance between cluster centroids10) and intra-prior ($$$\frac{1}{R_{p}}\sum_{i=1}^{R_{p}}\left\|p_{i}-P\right\|_{2}+\frac{1}{R_{n}}\sum_{j=1}^{R_{n}}\left\|n_{j}-N\right\|_{2}$$$; average point-wise distance from cluster centroids10) similarity terms: $$$α$$$, $$$β$$$ , and $$$γ$$$ are weighting hyperparameters for triplet, inter-prior, and intra-prior losses respectively. The triplet loss is calculated during region growing which terminates when either inter-prior loss falls below a threshold ε1 (priors are similar) or intra-prior loss surpasses a threshold ε2 (ROI voxels have high variance). These metrics generate differences between IR priors while ensuring each prior is internally consistent.
Materials and Methods
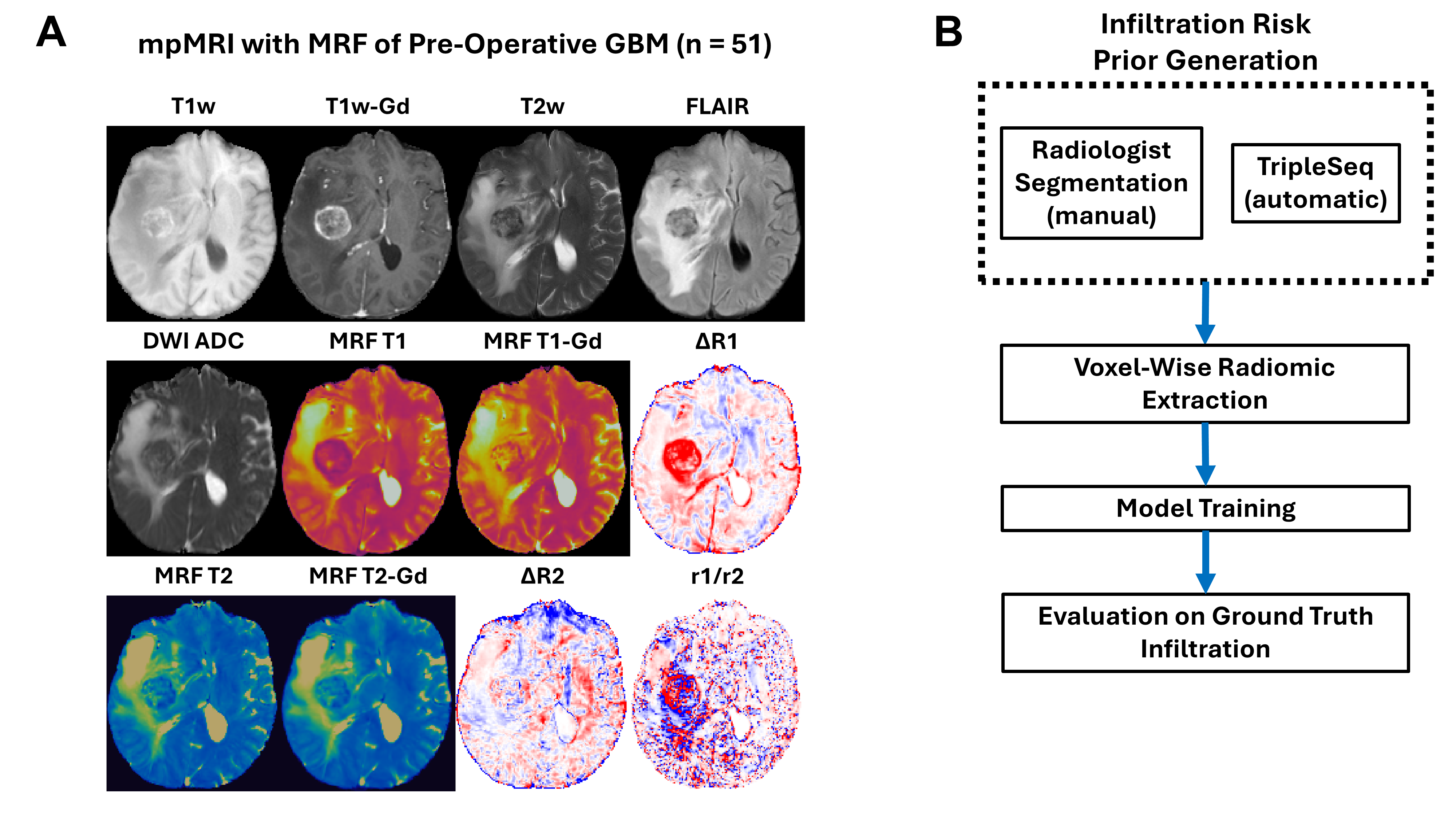
Pre-operative 3D MRF (T1 and T2; w/wo contrast) and mpMRI (T1w, T1w-Gd, T2w, FLAIR, and DWI ADC) from GBM patients (n = 51) was analyzed (Figure 2). MRI data was obtained from independent cohorts acquired between February 2017 and February 2020 (cohort 1) and between July 2022 and October 2023 (cohort 2) following IRB approval.Following tumor segmentation9 into ET and peritumor, IR prior generation with TripleSeq using mpMRI, MRF, and MRF-derived delta relaxometry maps11, voxel-wise mpMRI radiomic features (98 per MRI sequence (n = 12); 1176 total) were extracted12 from IR priors using a 5x5x5 sliding kernel (Figure 2). Features were used to train a multilayer perceptron (five FC layers) for voxel-wise classification of infiltration risk, using data from cohort 1, cohort 2, and combined cohorts. A subset (n = 14) of patients had pathologically confirmed non-enhancing peritumoral infiltration identified through targeted biopsy or intra-operative 5-ALA fluorescence13: these cases were withheld from training and had ground truth infiltration ROIs (n = 58) annotated by a board-certified neuroradiologist in collaboration with the operating neurosurgeon (Figure 2). Infiltration ROIs were used to test voxel-wise classification accuracy (Figure 4).
Results
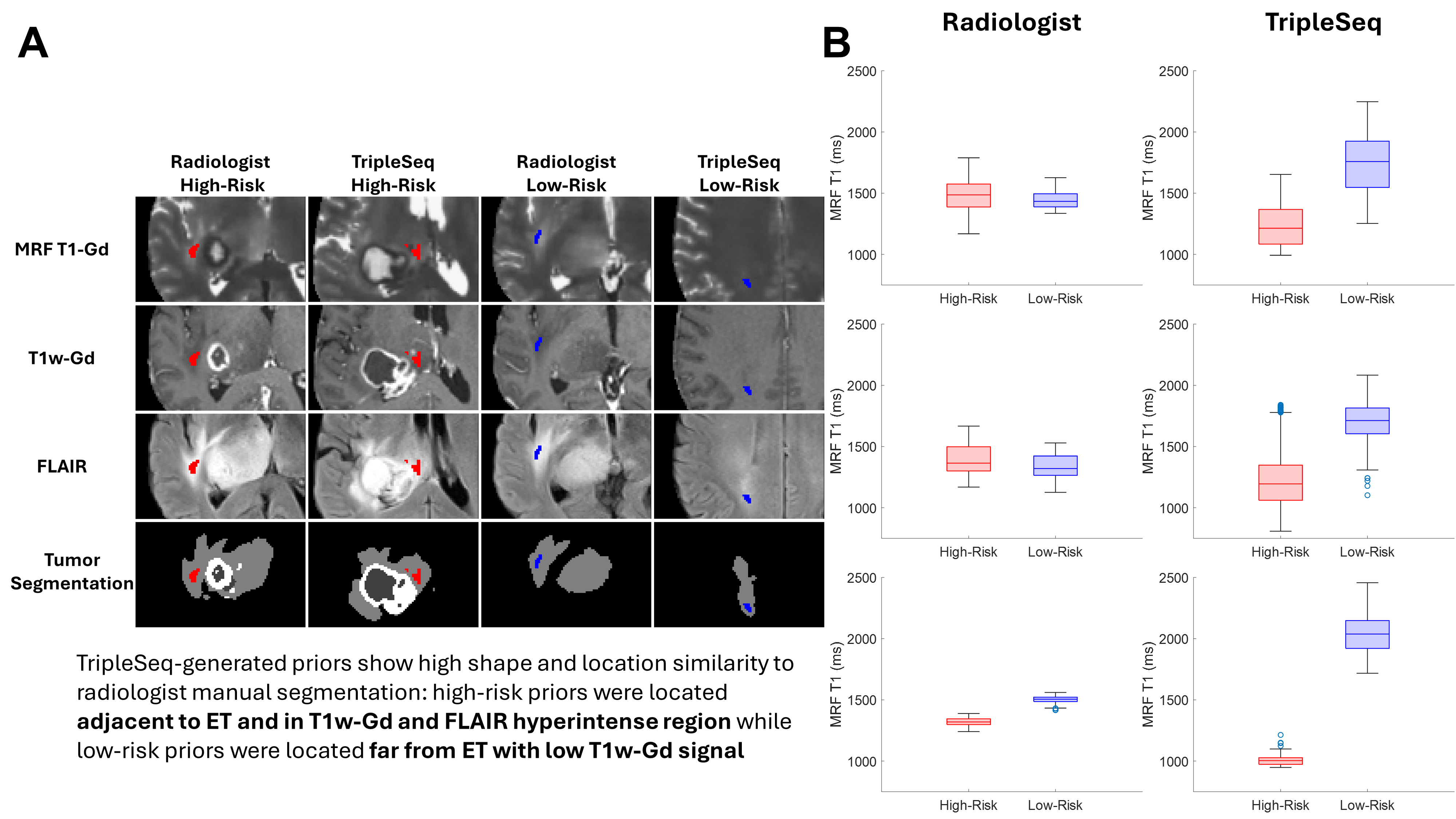
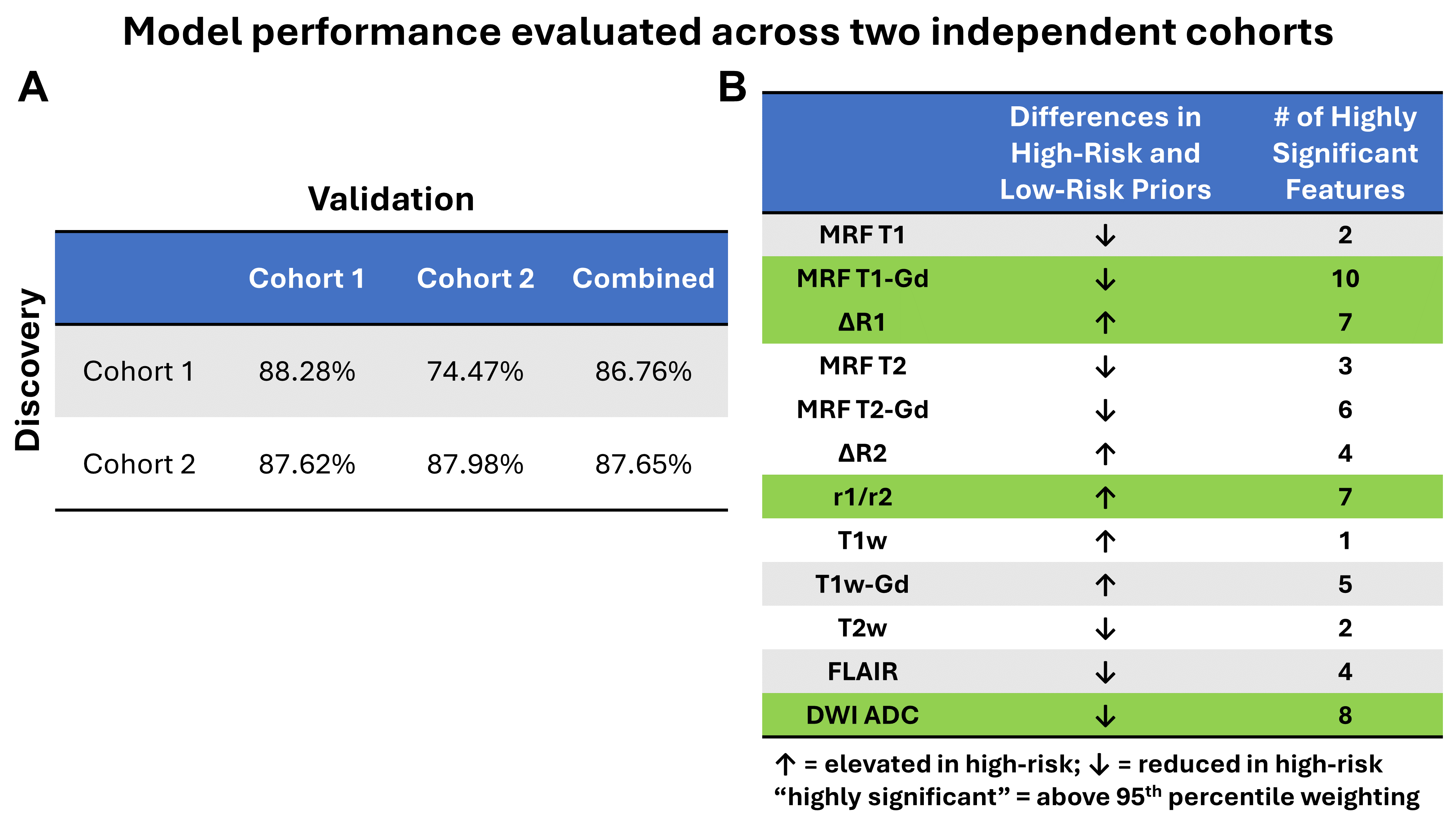
TripleSeq-generated priors showed consistent image feature trends compared to manual segmentation (Figure 3B), with high-risk priors being similar to ET and low-risk priors being dissimilar. Mean processing time per IR prior was < 1 min with TripleSeq and > 5 min manually. Across discovery-validation schemes, training with TripleSeq priors led to good test prediction (> 85% mean accuracy) of ground truth infiltration status (Figure 4A). Characteristic mpMRI feature value differences between high- and low-risk peritumor (Figure 4B) align with previously reported infiltration signatures1,2. MRF T1-Gd, ADC, r1/r2, and ΔR1 had the greatest number of highly significant features. Finally, the model can be applied to generate whole tumor infiltration prediction maps for prospective neurosurgical or radiotherapy guidance (Figure 5).Conclusion
We develop an automatic, data-driven method to generate infiltration risk priors for pre-operative GBM infiltration prediction from mpMRI. The trained model demonstrates high prediction accuracy of ground truth infiltration and can be applied prospectively to guide neurosurgery and radiotherapy.Acknowledgements
This work was supported by Siemens Healthineers, NIH grants R01 CA269604, R01 CA282516, R01 NS109439, T32 EB007509, T32 GM007250, and TL1 TR000441, the Imaging Devices and AI Technologies Track Funding Agency (Jobs Ohio), an American Cancer Society Institutional Research Grant, and the Radiation Oncology Institute.References
1. Rathore S, Akbari H, Doshi J, et al. Radiomic signature of infiltration in peritumoral edema predicts subsequent recurrence in glioblastoma: implications for personalized radiotherapy planning. J Med Imaging Bellingham Wash. 2018;5(2):021219. doi:10.1117/1.JMI.5.2.021219
2. Akbari H, Macyszyn L, Da X, et al. Imaging Surrogates of Infiltration Obtained Via Multiparametric Imaging Pattern Analysis Predict Subsequent Location of Recurrence of Glioblastoma. Neurosurgery. 2016;78(4):572-580. doi:10.1227/NEU.0000000000001202
3. Angeli S, Emblem KE, Due-Tonnessen P, Stylianopoulos T. Towards patient-specific modeling of brain tumor growth and formation of secondary nodes guided by DTI-MRI. NeuroImage Clin. 2018;20:664-673. doi:10.1016/j.nicl.2018.08.032
4. Yamahara T, Numa Y, Oishi T, et al. Morphological and flow cytometric analysis of cell infiltration in glioblastoma: a comparison of autopsy brain and neuroimaging. Brain Tumor Pathol. 2010;27(2):81-87. doi:10.1007/s10014-010-0275-7
5. Boutros F, Damer N, Kirchbuchner F, Kuijper A. Self-restrained triplet loss for accurate masked face recognition. Pattern Recognit. 2022;124:108473. doi:10.1016/j.patcog.2021.108473
6. Ma D, Gulani V, Seiberlich N, et al. Magnetic Resonance Fingerprinting. Nature. 2013;495(7440):187-192. doi:10.1038/nature11971
7. Smits M. MRI biomarkers in neuro-oncology. Nat Rev Neurol. 2021;17(8):486-500. doi:10.1038/s41582-021-00510-y
8. Giambra M, Di Cristofori A, Valtorta S, et al. The peritumoral brain zone in glioblastoma: where we are and where we are going. J Neurosci Res. 2023;101(2):199-216. doi:10.1002/jnr.25134
9. Kamnitsas K, Ledig C, Newcombe VFJ, et al. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Med Image Anal. 2017;36:61-78. doi:10.1016/j.media.2016.10.004
10. Steinley Douglas. K-means clustering: A half-century synthesis. Br J Math Stat Psychol. 2006;59(1):1-34. doi:10.1348/000711005X48266
11. Deng S, Zhao W, Jordan DW, Badve C, Ma D. Delta-relaxometry with contrast-enhanced MR Fingerprinting: phantom validation and application to tumor imaging. In: Proceedings of the 31st Annual Meeting of the ISMRM. Toronto, Canada; 2023.
12. Zhao W, Hu Z, Kazerooni AF, et al. Physics-Informed Discretization for Reproducible and Robust Radiomic Feature Extraction Using Quantitative MRI. Invest Radiol. September 2023:10.1097/RLI.0000000000001026. doi:10.1097/RLI.0000000000001026
13. Chohan MO, Berger MS. 5-Aminolevulinic acid fluorescence guided surgery for recurrent high-grade gliomas. J Neurooncol. 2019;141(3):517-522. doi:10.1007/s11060-018-2956-8
Figures