0007
Dynamic lung water magnetic resonance imaging during exercise stress1Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
Keywords: YIA, Data Acquisition, Acquisition & Analysis, Body, Lung, Lung water, Heart failure, Translational Studies
Motivation: Quantification of lung water during exercise is of interest for early diagnosis of heart failure.
Goal(s): To develop a time-resolved 3D MRI method to quantify lung water in transitions between rest and exercise.
Approach: We derive quantitative time-resolved lung water density (LWD) maps using a motion corrected sliding-window image reconstruction. We included 12 healthy controls and 2 patients with heart failure, and a porcine model of mitral regurgitation (n=5).
Results: We measured a peak exercise ΔLWD=16±6.8% in controls, but detected no changes during rest (ΔLWD=-1.4±3.5%, p=0.18). Accumulation rates were slower in patients (2.0±0.1%/min) vs controls (2.6±0.9%/min). Animals developed ΔLWD=3.3±1.5%.
Impact: Exercise-induced changes in lung water can be dynamically quantified using a continuous 3D MRI acquisition with a sliding-window and motion corrected image reconstruction, which may have clinical utility in unmasking latent heart failure at early stages of disease.
Introduction
Shortness of breath during physical activity can be an early sign of heart failure, and is caused by an accumulation of fluid in the lungs. This lung water buildup occurs when abnormal increases in blood pressure during exercise triggers fluid leakage from blood vessels into the extravascular pulmonary interstitium1. Measuring lung water during exercise may therefore detect heart failure early. MRI has shown promise in measuring lung water, but previous methods have only been employed at rest or immediately after exercise2–6, not during exercise itself. Here, we develop a novel method to dynamically measure lung water during exercise. We test this method during supine exercise stress in healthy subjects and patients with heart failure, and validate it with a porcine model of dynamic lung water accumulation through mitral regurgitation.Methods
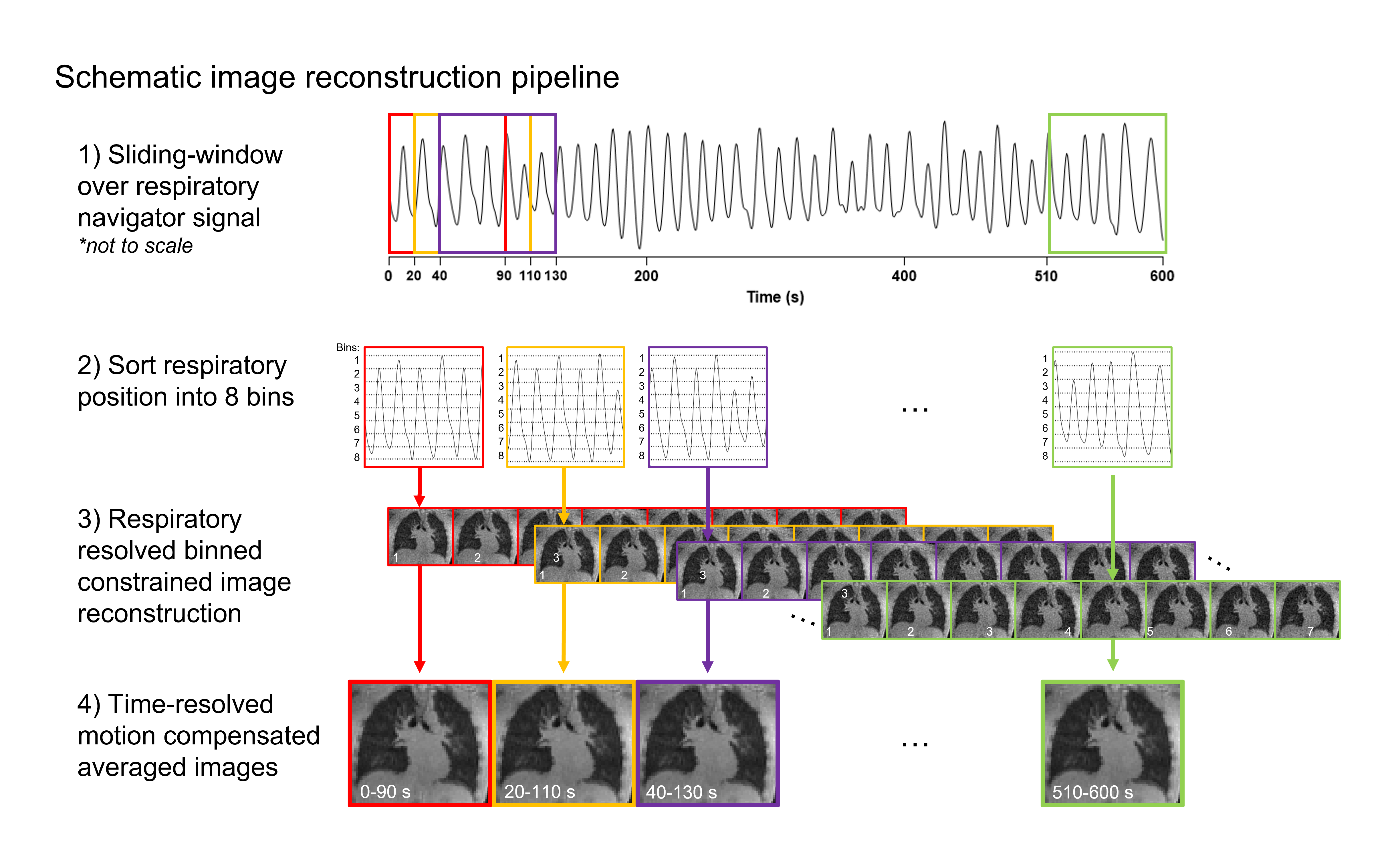
In this IRB- and IACUC-approved study, we utilized a 3D self-gated stack-of-spirals proton density weighted gradient echo sequence to continuously measure lung water at 0.55T (prototype MAGNETOM Area, Siemens)7,8. Typical sequence parameters were TE/TR/θ=0.56ms /9ms/1°, 831 in-plane golden angle spiral interleaves, 5.0ms spiral readout, 3.5x3.5x3.5mm resolution, and 450x450x252mm FOV. To derive time-resolved images for dynamic analysis, we developed a motion-corrected sliding-window compressed sensing image reconstruction with spatial and temporal total variation constraints, sampling 90s of data with a 20s temporal increment (Figure 1)8–11.We generated dynamic pixel-wise LWD maps using automated image analysis, which involved a U-net lung segmentation and signal intensity-based coil shading correction4. LWD maps were derived as the ratio of signal intensities within the lungs to surrounding body tissue, assuming a 70% musculoskeletal water density4. Dynamic ΔLWD was computed as the percentage change in global and regional LWD over time.
To validate the ability of detecting changes in lung water, we utilized a controlled porcine model of severe mitral regurgitation (n=5, 40±2kg). Mitral regurgitation was induced dynamically inside the MRI scanner by applying tension to a suture placed across the anterior mitral leaflet, externally accessed through a femoral vascular sheath. Lung water accumulation was monitored for 10 minutes, along with simultaneous pulmonary arterial wedge pressure (PAWP) measurements. We assessed cardiac output and mitral regurgitation from short-axis-stack cine and aortic flow images.
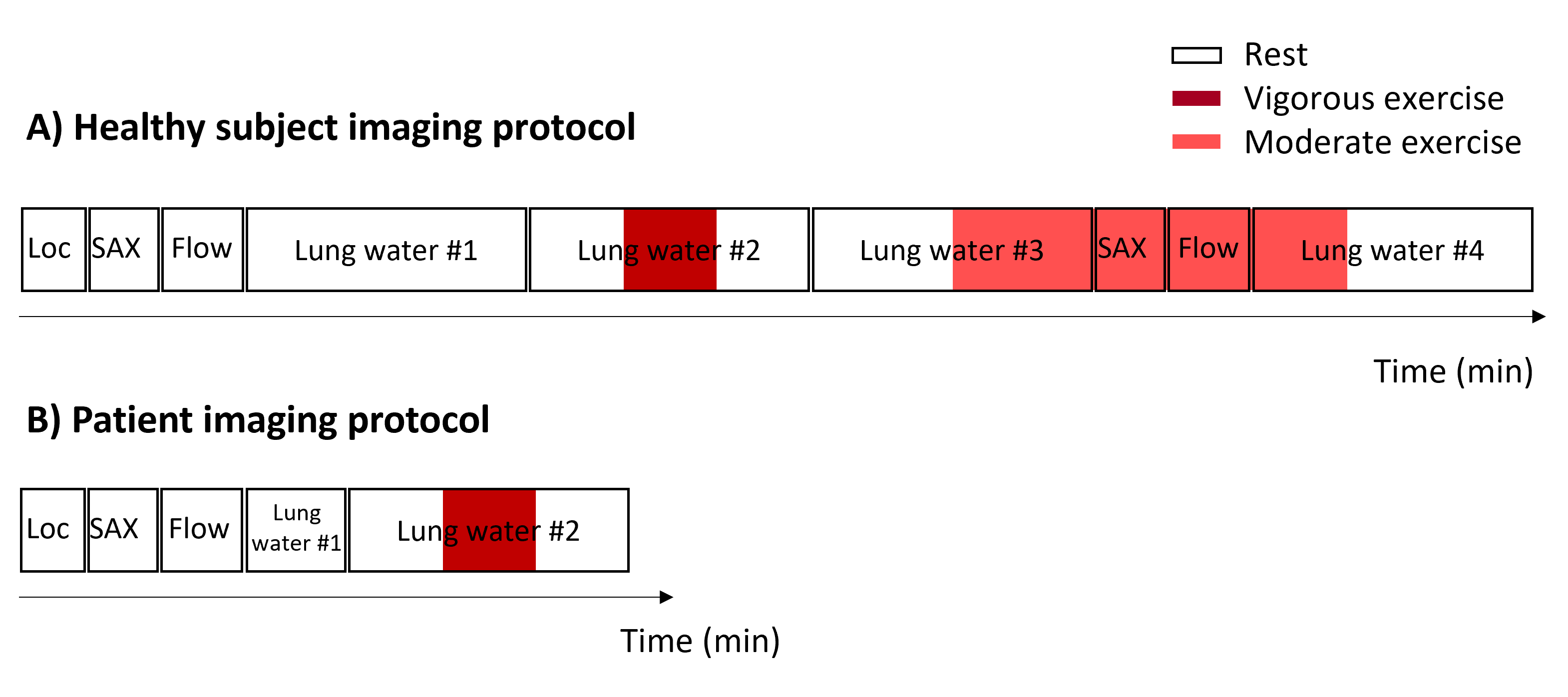
Exercise imaging was performed using an MRI-compatible supine pedal ergometer with 60-90W resistance. We included 12 healthy subjects (27±5yrs, 3 female) and 2 patients (61±4 years, 1 female). The imaging protocols are illustrated in Figure 2.
Results
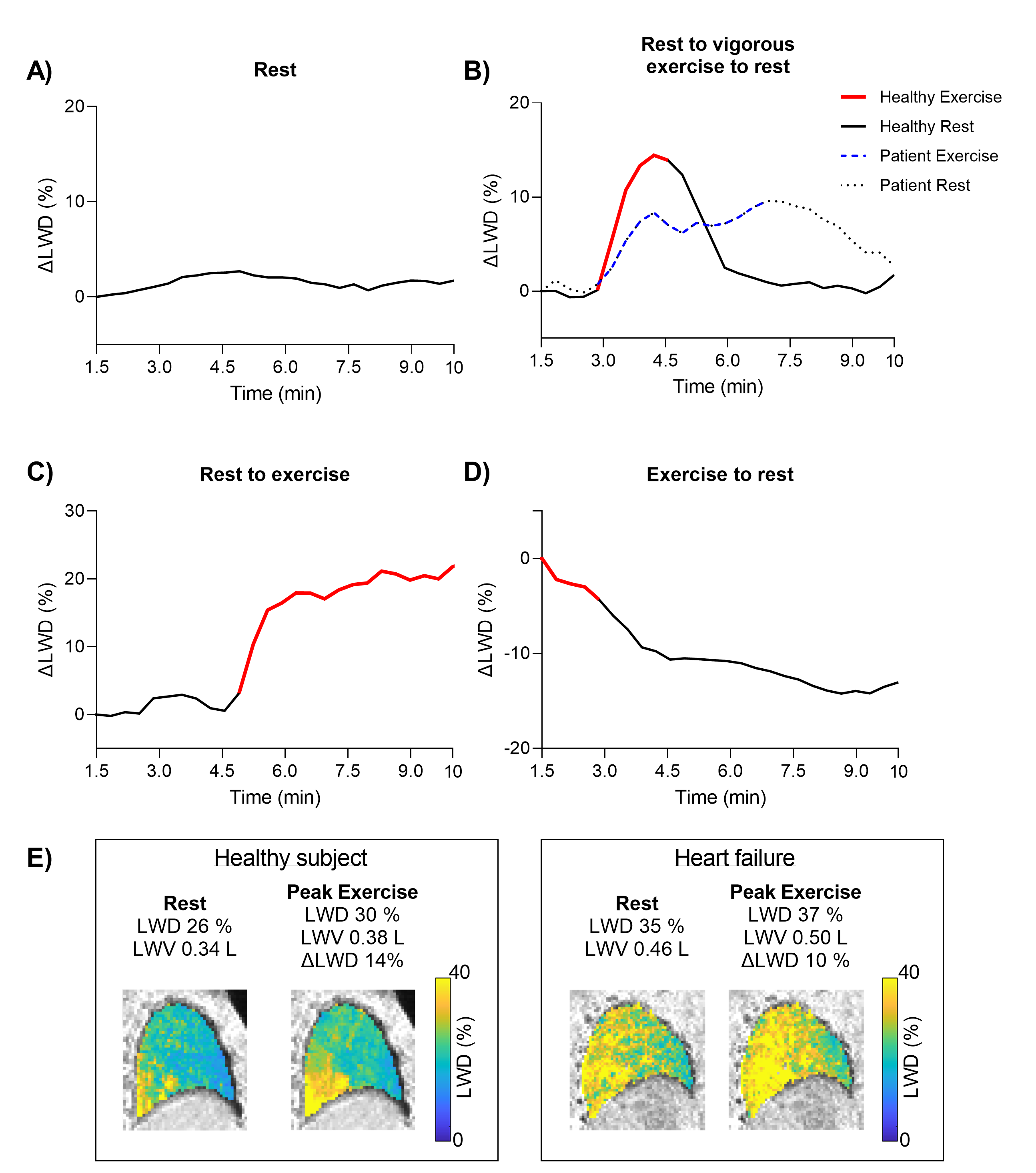
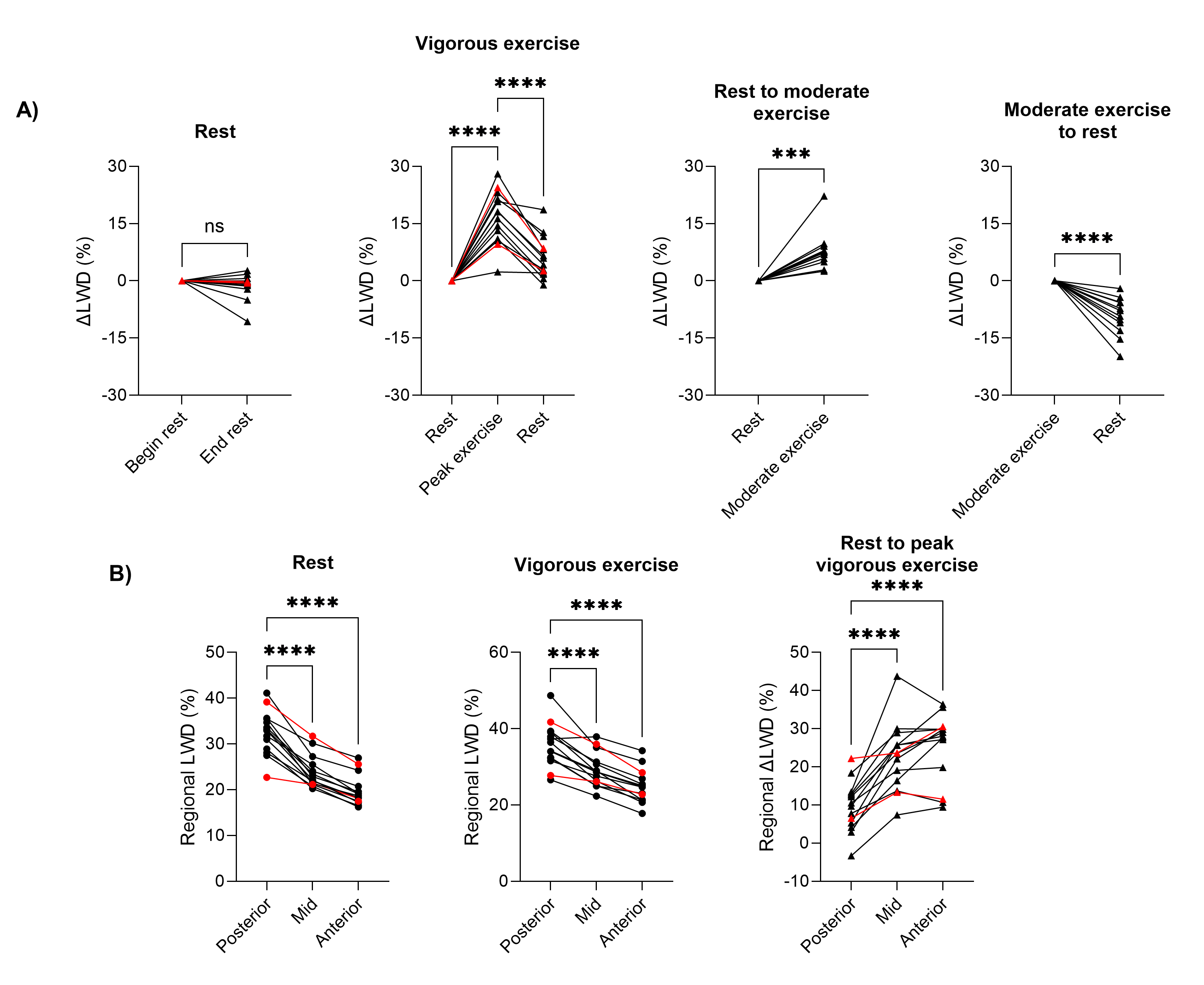
Dynamic LWD imaging during induction of mitral regurgitation and exercise stress was feasible, as illustrated in the Figure 3 animation. Figure 4 shows examples of ΔLWD in a patient and control, and Figure 5 shows regional changes in LWD. Controls developed a ΔLWD of 7.8±5.0% during moderate exercise, peaked at 16±6.8% during vigorous exercise, and remained unchanged over 10 minutes at rest (-1.4±3.5%, p=0.18). We hypothesize the increases in LWD are explained by an augmented intravascular fluid during exercise, as cardiac output increased from 4.5±1.5 L/min at rest to 7.5±2.6 L/min at moderate exercise, p=0.0004. Regional LWD were higher posteriorly compared the anterior lungs (rest: 33±3.7% vs 20±3.1%, p<0.0001; peak exercise: 36±5.5% vs 25±4.6%, p<0.0001), as expected4. A larger ΔLWD was measured anteriorly (33±10%) than posteriorly (16±10%), p<0.0001. Accumulation rates were slower in patients than controls (2.0±0.1%/min vs 2.6±0.9%/min, respectively), whereas LWD were similar at rest (28±10% vs 28±2.9%) and peak exercise (ΔLWD 17±10% vs 16±6.8%).Porcine experiments yielded a 45±24% mitral regurgitant fraction and an ΔLWD increase of 3.3±1.5%. PAWP increased by 6.6±3.1 mmHg (101±112%, p=0.009), and cardiac output decreased from 3.9±0.8 to 2.7±0.6L/min, p=0.007, suggesting the ΔLWD was extravascular.
Discussion
We introduce a technique capable of measuring dynamic changes in LWD and demonstrate its feasibility in a controlled animal model, and in subjects undergoing exercise MRI. The isotropic spatial resolution support images being re-sliced into any orientation, thus enabling regional LWD analysis. The method does, however, not differentiate between fluid inside and outside the vasculature. We noted slower rates of lung water accumulation in patients compared to controls, although not necessarily higher overall lung water content or peak changes, but did not perform statistics due to small patient sample size. The time-derivative dLWD/dt, which requires time-resolved lung water images, may therefore be a valuable clinical parameter for heart failure characterization. Patient studies are needed to assess if this method can detect latent heart failure, where a pathological extravascular lung water accumulation is expected.Conclusion
Dynamic changes in lung water density can be dynamically quantified using a continuous 3D MRI proton density weighted sequence with a sliding-window and respiratory motion-corrected image reconstruction.Acknowledgements
The authors would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T, and the stack-of-spirals UTE sequence, under an existing cooperative research agreement (CRADA) between NHLBI and Siemens Healthcare. We would also like to acknowledge the contributions of Amelia Nargozian, Andrea Jaimes, William H. Schenke, John Kakareka, Victoria Frasier, Katherine Lucas, and Rim Halaby.References
1. Devroey D, Van Casteren V. Signs for early diagnosis of heart failure in primary health care. Vasc Health Risk Manag 2011;7:591–596. doi:10.2147/VHRM.S24476.
2. Thompson RB, Chow K, Pagano JJ, Sekowski V, Michelakis ED, Tymchak W, et al. Quantification of lung water in heart failure using cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson 2019;21:58. doi:10.1186/s12968-019-0567-y.
3. Burrage MK, Hundertmark M, Valkovič L, Watson WD, Rayner J, Sabharwal N, et al. Energetic Basis for Exercise-Induced Pulmonary Congestion in Heart Failure With Preserved Ejection Fraction. Circulation 2021;144:1664–1678. doi:10.1161/CIRCULATIONAHA.121.054858.
4. Seemann F, Javed A, Chae R, Ramasawmy R, O’Brien K, Baute S, et al. Imaging gravity-induced lung water redistribution with automated inline processing at 0.55 T cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2022;24:35. doi:10.1186/s12968-022-00862-4.
5. Meadus WQ, Stobbe RW, Grenier JG, Beaulieu C, Thompson RB. Quantification of lung water density with UTE Yarnball MRI. Magn Reson Med 2021;86:1330–1344. doi:10.1002/mrm.28800.
6. Rocha BML, Cunha GJL, Freitas P, Lopes PMD, Santos AC, Guerreiro S, et al. Measuring lung water adds prognostic value in heart failure patients undergoing cardiac magnetic resonance. Sci Rep 2021;11:20162. doi:10.1038/s41598-021-99816-6.
7. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology 2019;293:384–393. doi:10.1148/radiol.2019190452.
8. Javed A, Ramasawmy R, O’Brien K, Mancini C, Su P, Majeed W, et al. Self-gated 3D stack-of-spirals UTE pulmonary imaging at 0.55T. Magn Reson Med 2022;87:1784–1798. doi:10.1002/mrm.29079.
9. Zhu X, Chan M, Lustig M, Johnson KM, Larson PEZ. Iterative motion-compensation reconstruction ultra-short TE (iMoCo UTE) for high-resolution free-breathing pulmonary MRI. Magn Reson Med 2020;83:1208–1221. doi:10.1002/mrm.27998.
10. Zachiu C, Papadakis N, Ries M, Moonen C, Denis De Senneville B. An improved optical flow tracking technique for real-time MR-guided beam therapies in moving organs. Phys Med Biol 2015;60:9003–9029. doi:10.1088/0031-9155/60/23/9003.
11. Zachiu C, Denis De Senneville B, Moonen C, Ries M. A framework for the correction of slow physiological drifts during MR-guided HIFU therapies: Proof of concept. Med Phys 2015;42:4137–4148. doi:10.1118/1.4922403.
Figures