0002
Assessment of Complex Flow Patterns in Patients with Carotid Webs, Patients with Carotid Atherosclerosis, and Healthy Subjects Using 4D Flow MRI1Biomedical Engineering, Georgia Institute of Technology, Atlanta, GA, United States, 2Department of Radiology & Imaging Sciences, Emory University, Atlanta, GA, United States, 3Department of Neurology, Emory University, Atlanta, GA, United States
Synopsis
Keywords: Flow, Blood vessels, 4D Flow MRI
Motivation: The motivation of this work is to understand the hemodynamics parameters in subjects with carotid web (CaW), atherosclerosis subjects with similar luminal narrowing, and normal subjects using 4D Flow MRI.
Goal(s): The main goal of this work is to quantify parameters related to vascular dysfunction including wall shear stress (WSS) and oscillatory shear index (OSI).
Approach: 4D Flow MRI was utilized to prospectively scan subjects with CaW and hemodynamic parameters were compared to subjects with mild atherosclerosis and healthy volunteers.
Results: The results show that subjects with CaW have larger regions of complex blood flow represented by low WSS and high OSI.
Impact: This study improves our understanding of disturbed hemodynamics caused by CaWs in comparison to atherosclerosis, which may explain the mechanism of thrombus formation and lay the groundwork for stroke risk assessment in patients with CaW.
Introduction
Carotid webs (CaWs) are fibromuscular pyramid-like or shelf-like projections in the internal carotid artery (ICA). CaWs are not related to atherosclerotic plaques and generally cause <50% stenosis and may account for one-third of cryptogenic strokes [1]. CaWs have been shown to have a prevalence of 1.2%-2.5% of all subjects presenting with acute stroke [2-4].Understanding hemodynamic alterations caused by CaWs is imperative to assessing stroke risk. Time-Average Wall Shear Stress (TAWSS) and Oscillatory Shear Index (OSI) are hemodynamic parameters linked to vascular dysfunction and thrombosis. The purpose of the study was to quantify TAWSS and OSI in carotid bifurcation to improve our understanding of vascular dysfunction and subsequent stroke risk in CaW patients. We hypothesized that CaWs are associated with lower TAWSS and higher OSI than mild atherosclerosis or healthy carotid bifurcation.Methods
The IRB-approved study included a total of 35 subjects (N=14 bifurcations with CaW, 11F, age:49±10, 10 mild atherosclerosis 6F, age: 72±9, 11 healthy 9F, age:42±13). All subjects were imaged in a 3 Tesla MRI scanner (Siemens PrismaFit, Erlangen Germany) using a 4-channel neck coil (Machnet BV, the Netherlands) in combination with a 20-channel head/neck coil. 4D flow MRI scans were acquired in a parasagittal orientation planned in the plane of the bifurcation with the following parameters: FOV=162*200mm2, isotropic spatial resolution=1mm3, TR/TE=47ms/5ms; GRAPPA acceleration factor=2, velocity encoding (VENC)=60-80 cm/s in all directions, scan time=4.8±0.9 min and all images were retrospectively reconstructed with 24 timeframes over the cardiac cycle. 4D Flow MRI images were corrected, combined to generate MRA images, and segmented (Figure 1)[5, 6]. Velocity pathlines were generated using EnSight (Figure 1). 4D Flow velocity data were analyzed in two ways: a 3D surface in the bulbar ICA region (bulb region) and four 2D cross-sectional analyses. The 3D surface in the bulb region is where complex flow patterns are expected and allowed us to quantify the regions where low TAWSS and high OSI were present (Figure 3). The bulb region was determined as the region from the bifurcation to one and a half CCA diameters downstream. The threshold of the low TAWSS and high OSI was determined as a 10% threshold based on all combined subjects' data. Four 2D planes were placed perpendicular to the centerline of the carotid bifurcation for a detailed analysis of TAWSS and OSI (Figure 2). Independent samples Kruskal-Wallis-H test with 0.05 was used for statistical significance.Results
Figure 3 shows an example case of a subject with CaW, a subject with mild atherosclerosis, and a normal subject with velocity pathlines, TAWSS heatmaps, OSI heatmaps, low TAWSS, and high OSI heat maps. Using the 3D volumetric analysis, the percent surface area where low TAWSS was present in the ICA bulb was 12.3 ± 8.0% in CaW subjects, 1.6 ± 1.9% in atherosclerosis, and 8.5 ± 7.7% in healthy subjects, all differences were statistically significant, p-value CaW vs. healthy=0.2) (Figure 4). In the four 2D cross-sectional analyses, the results were statistically significant when comparing CaW subjects to patients with atherosclerosis at all four cross-sections (0.3 ± 0.1 N/m2 versus 0.6 ± 0.3 N/m2) and to normal subjects (0.4 ± 0.1 N/m2). OSI had similar values in the CCA between groups (p-value=0.5), but OSI was significantly higher downstream of the bifurcation in CaW subjects compared to atherosclerosis and normal subjects. OSI returned to be similar values between groups 1.5 diameters distal to the bifurcation (p-value= 0.7) (Figure 5).Discussion
CaWs have been linked to TIA and ischemic stroke in younger patients [1, 3]. This study showed that CaW induced significant complex hemodynamics (higher OSI) compared to atherosclerotic lesions with a similar degree of luminal narrowing mainly represented by the larger region exposed to low TAWSS and high OSI compared to patients with mild atherosclerosis or normal subjects. Additionally, CaW subjects had higher OSI in cross-sections from the web to 1.0 CCA diameters distal to the lesion compared to patients with mild atherosclerosis and normal bifurcations (Figure 5). These factors show vascular dysfunction, which may increase clot formation risk in subjects with CaW.Conclusion
4D flow MRI was utilized to quantify the parameters in patients with CaW to analyze the hemodynamic differences between subjects with CaW, subjects with mild atherosclerosis, and healthy subjects. Lower TAWSS and higher OSI are present in the ICA bulb in patients with CaW when compared to patients with atherosclerotic or healthy subjects.Acknowledgements
This work was funded by National Institutes of Health Grant Numbers: R21NS114603 (Allen and Oshinski) and NIH R01 #R01EB027774 (Oshinski); the American Heart Association Innovative Project Award No. 19IPLOI34760670 (Allen). Additionally, by the National Science Foundation Graduate Research Fellowship Program under Grant No. 1937971 (El Sayed).References
[1] Haussen, D.C., J.A. Grossberg, M. Bouslama, et al., Carotid web (intimal fibromuscular dysplasia) has high stroke recurrence risk and is amenable to stenting. Stroke, 2017. 48(11): p. 3134-3137. DOI: 10.1161/strokeaha.117.019020.
[2] Joux, J., M. Boulanger, S. Jeannin, et al., Association between carotid bulb diaphragm and ischemic stroke in young Afro-caribbean patients: a population-based case-control study. Stroke, 2016. 47(10): p. 2641-4. DOI: 10.1161/strokeaha.116.013918.
[3] Sajed, P.I., J.N. Gonzalez, C.A. Cronin, et al., Carotid bulb webs as a cause of "cryptogenic" ischemic stroke. AJNR Am J Neuroradiol, 2017. 38(7): p. 1399-1404. DOI: 10.3174/ajnr.A5208.
[4] Kim, S.J., R.G. Nogueira, and D.C. Haussen, Current Understanding and Gaps in Research of Carotid Webs in Ischemic Strokes: A Review. JAMA Neurol, 2019. 76(3): p. 355-361. DOI: 10.1001/jamaneurol.2018.3366.
[5] Markl, M., A. Harloff, T.A. Bley, et al., Time-resolved 3D MR velocity mapping at 3T: improved navigator-gated assessment of vascular anatomy and blood flow. J Magn Reson Imaging, 2007. 25(4): p. 824-31. DOI: 10.1002/jmri.20871.
[6] Stalder, A.F., M.F. Russe, A. Frydrychowicz, et al., Quantitative 2D and 3D phase contrast MRI: Optimized analysis of blood flow and vessel wall parameters. Magnetic Resonance in Medicine, 2008. 60(5): p. 1218-1231. DOI: 10.1002/mrm.21778.
Figures
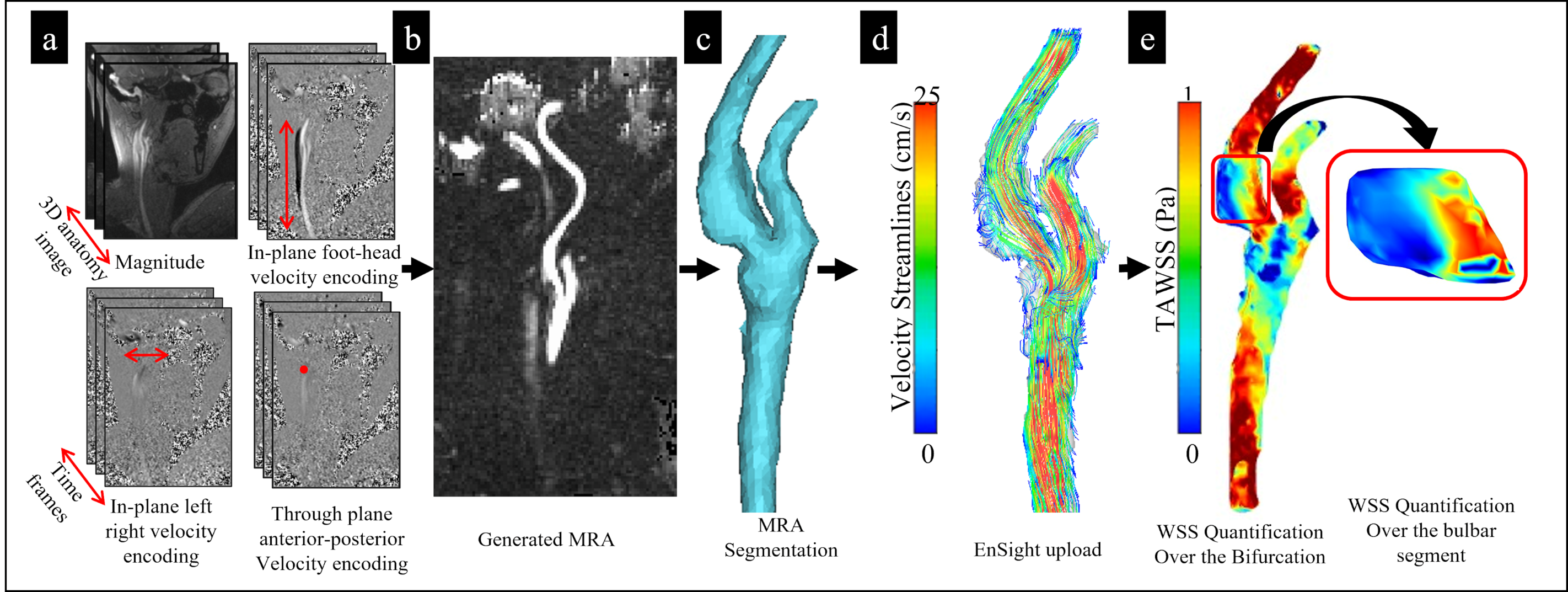
Figure 1. a) 4D flow MRI sequence: 3D magnitude, with 3D velocity encoding directions, acquired across multiple time points in the cardiac cycle. b) the combined velocities directions into an MRA image. c) the segmentation of the MRA image, in CaW cases, where patients undergone a CTA scan. d) Particle pathlines velocity magnitude color-coded in a carotid bifurcation. e) TAWSS heat map of the carotid bifurcation with the bulbar segment region analyzed.
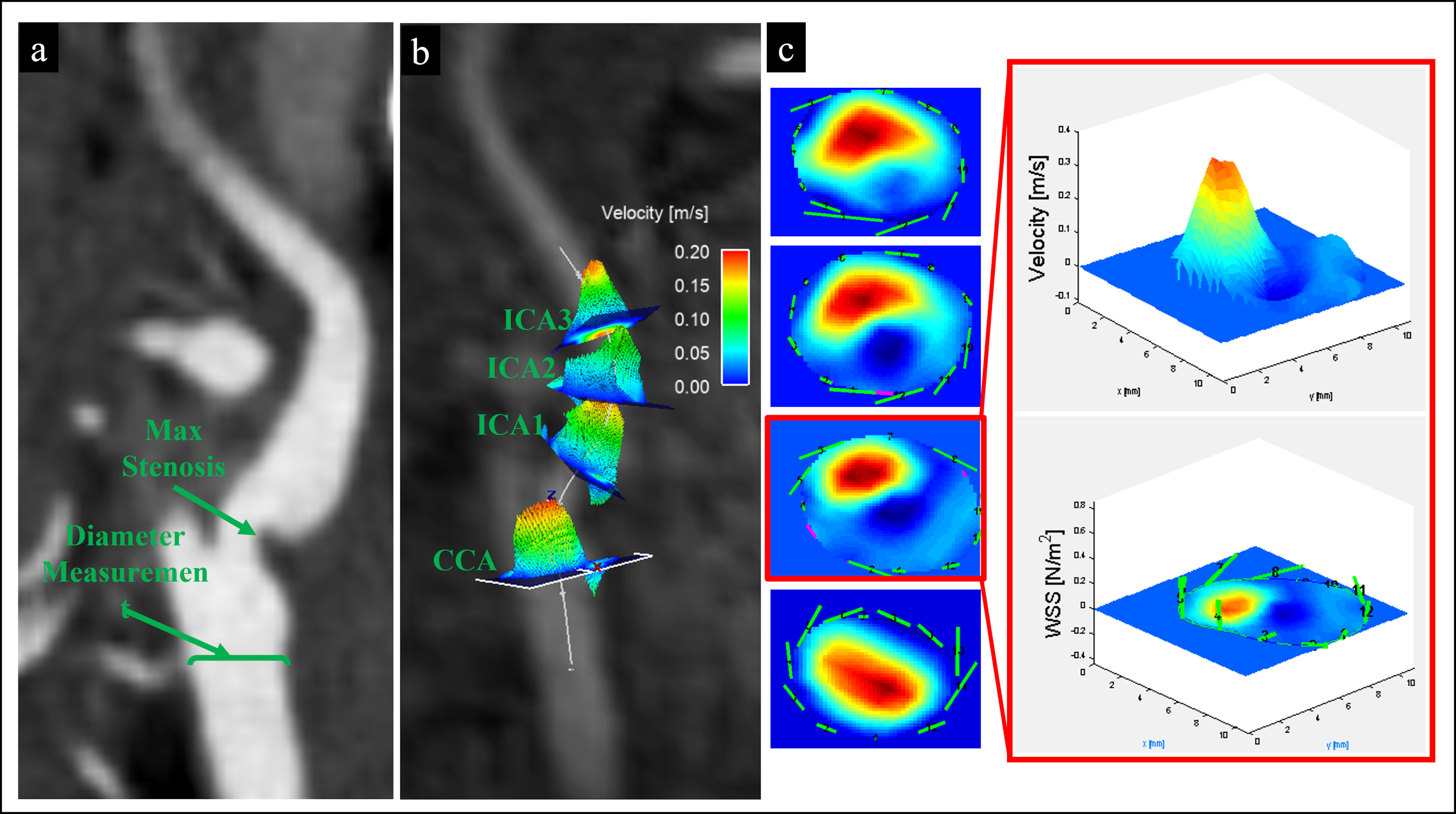
Figure 2. a) shows a CTA image of a patient with CaW. The CCA diameter and maximum stenosis location were measured. b) shows the 2D cross-sectional planes inserted perpendicular to the centerline of the vessel one in CCA and three in the ICA located 0.5D, 1D, and 1.5D above maximum stenosis. c) shows an example of extracted planes with manual ROI segmentation for the calculation of WSS.
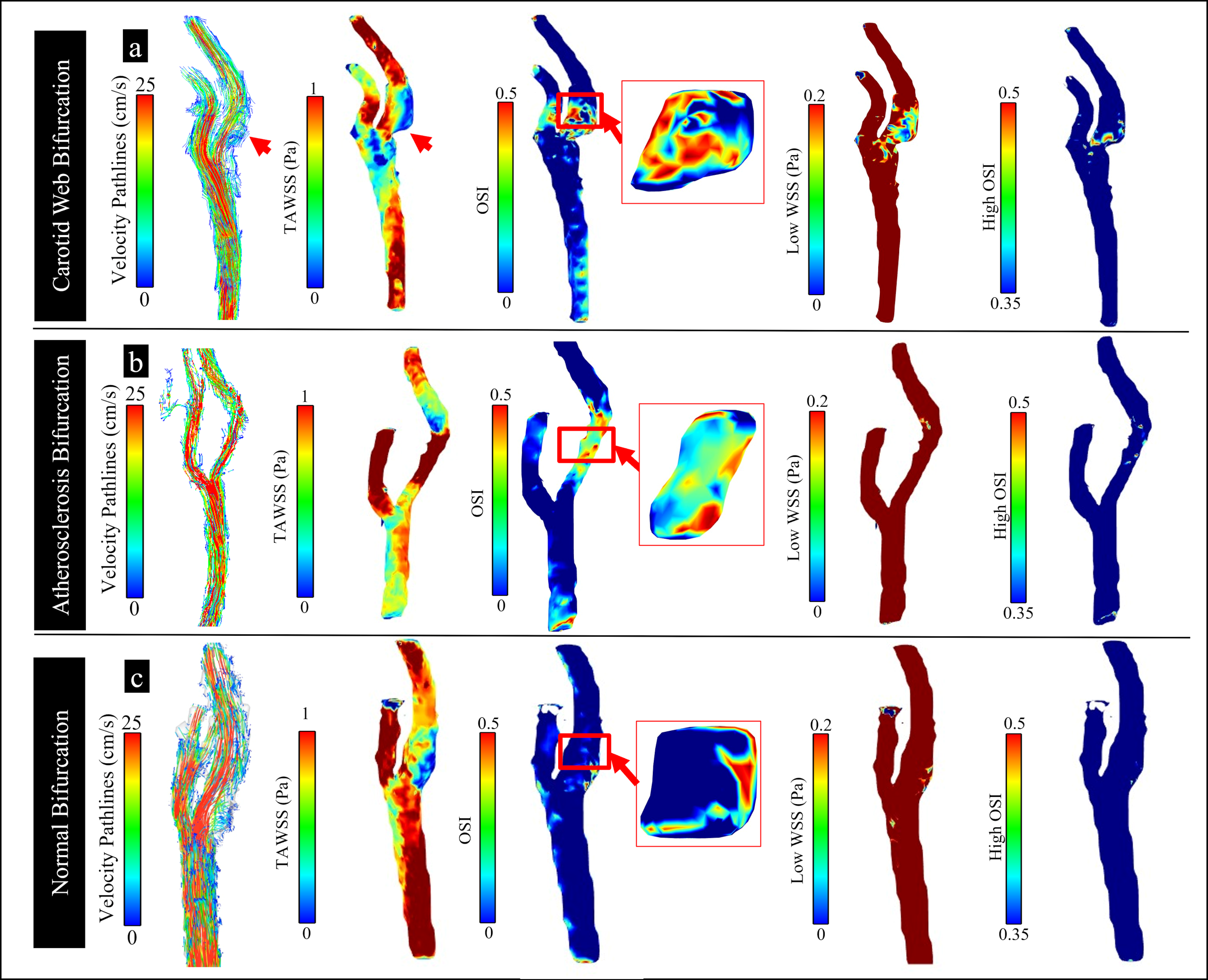
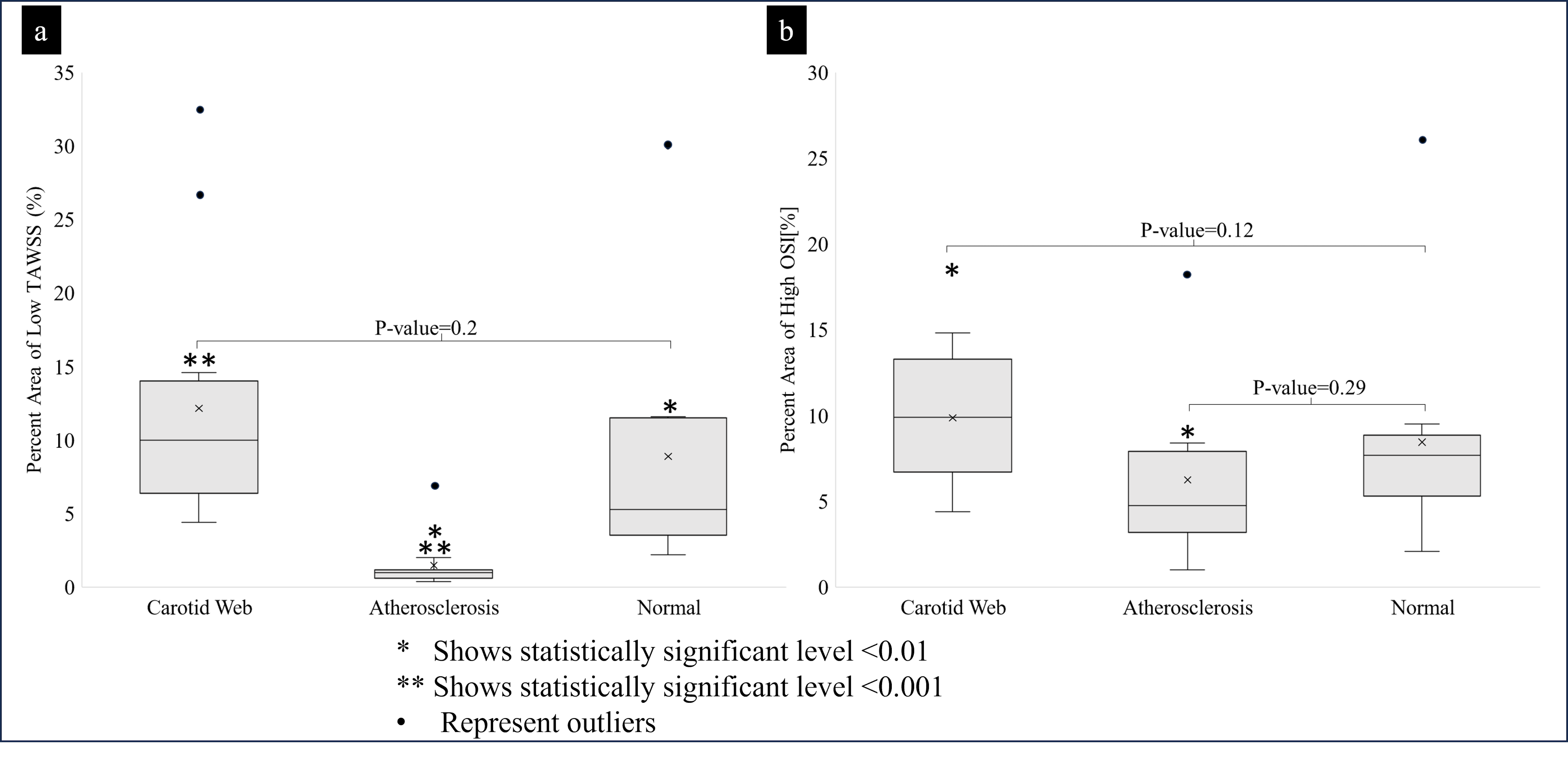
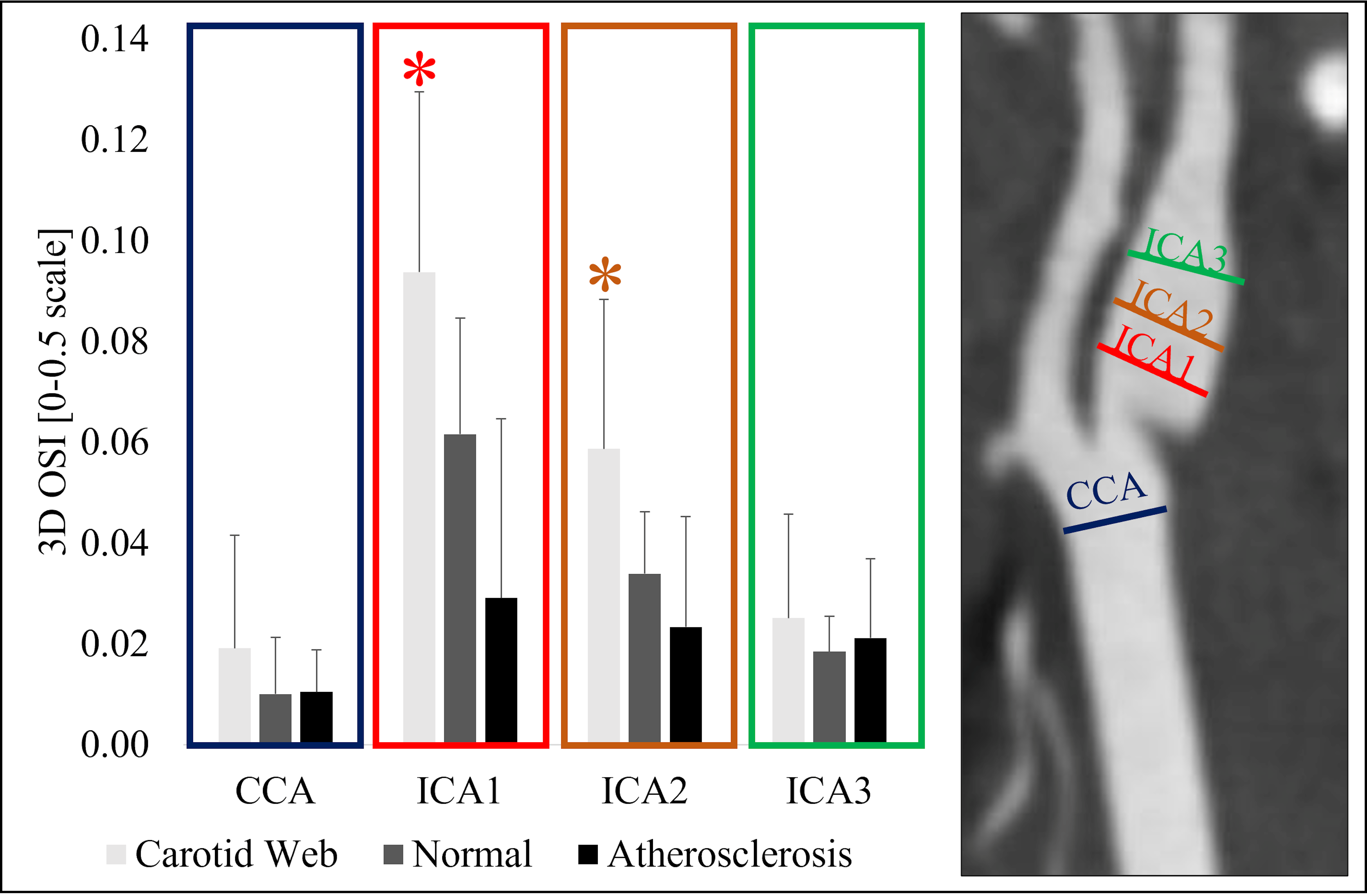
Figure 5. OSI results in patients with CaW, atherosclerosis, and normal carotid bifurcation in CCA, ICA1, ICA2 & ICA3 represented by a bar plot. Note: statistical significance observed in ICA1 and ICA2 is represented by an asterisk*.