FDG PET-MRI: Wins Over PET-CT
1Department of Radiology, Kobe University Hospital, Kobe, Japan, 2Biomedical Imaging Research Center, University of Fukui, Fukui, Japan
Synopsis
Keywords: Physics & Engineering: PET/MR, Cross-organ: Cancer, Body: Body
PET/MRI has advantages over PET/CT as it allows for simultaneous acquisition of two functional images, providing additional insights that are not possible when imaged separately. PET/MRI can detect changes in the two functional imaging over time and obtain superior fusion images regardless of the patient's motion during the examination. PET/MRI can produce accurate fusion images even in the lung by respiratory-gated simultaneous acquisition of ZTE with PET. It also enables quantitatively assessing the uptake and excretion of tracers in the gastrointestinal tract. Time-synchronized PET/MRI enables an accurate assessment of lesion extension and MRI-based PET regions of interest.Introduction
The advantages of PET/MRI over PET/CT that most people may initially think of are the reduced radiation exposure due to the absence of CT imaging and the superior contrast resolution of MRI compared to CT, which is useful in evaluating specific organs and lesions(1-4). However, the actual utility is the ability to simultaneously obtain images from two very different examinations, PET and MRI. This syllabus will explain the utility of PET/MRI through simultaneous PET and MRI acquisition, which cannot be accomplished with PET/CT.Dual functional imaging
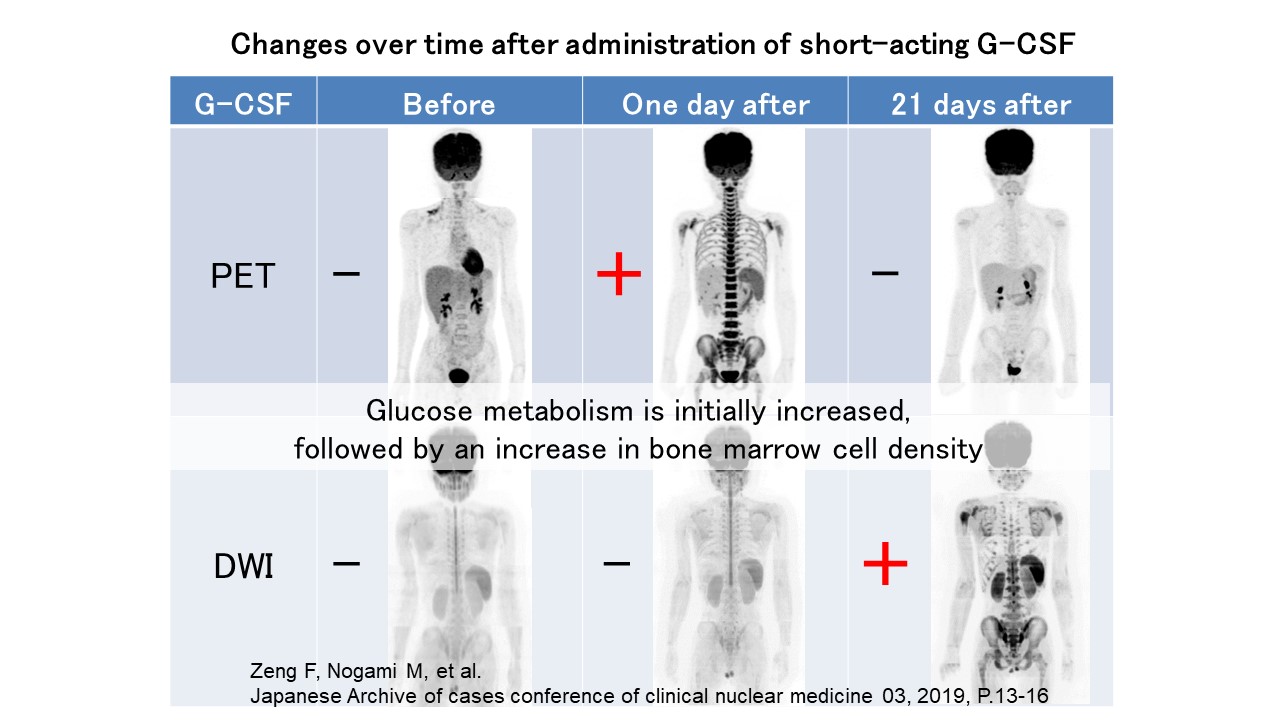
While PET provides quantitative and functional imaging, MRI offers various aspects of functional imaging, including diffusion-weighted images. PET/MRI allows for the simultaneous acquisition of both functional images, enabling spatial or temporal evaluation of organs and lesions throughout the body. Diffusion-weighted Whole-body Imaging with Background Suppression (DWIBS) is a diffusion-weighted image combined with fat suppression and can produce images similar to fluorine-18 fluorodeoxyglucose (FDG) PET. DWIBS can produce images similar to fluorine-18 fluorodeoxyglucose (FDG) PET. Although simultaneous imaging of FDG PET and DWIBS is often considered redundant due to similar findings(1), it can provide additional insights since glucose metabolism and diffusion restriction are different phenomena(5). PET/MRI is capable of detecting changes in normal bone marrow over time due to granulocyte colony-stimulating factor (G-CSF) administration, which is commonly used as an adjuvant to leukopenia after chemotherapy in cancer patients. Early after administration, increased FDG PET accumulation is observed, followed by an increased signal on diffusion-weighted images, suggesting that normal bone marrow glucose metabolism is first enhanced after G-CSF administration, followed by increased cell density (Figure 1). The ability to obtain two functional images simultaneously and observe changes over time is a unique advantage of PET/MRI.Time-synchronized imaging
PET/MRI can obtain superior fusion images regardless of the patient's motion during the examination, thanks to its capability of simultaneous acquisition(6). In contrast, PET/CT cannot perform simultaneous acquisition, making it impossible to avoid misalignment on the fused image due to respiratory motion, cardiac motion, peristalsis of the gastrointestinal tract, and motion associated with urinary tract excretion. The superior fusion imaging accuracy of PET/MRI contributes to improved diagnostic performance in assessing the local extent of lesions and the accuracy of the region of interest in quantitative assessment.Respiratory motion
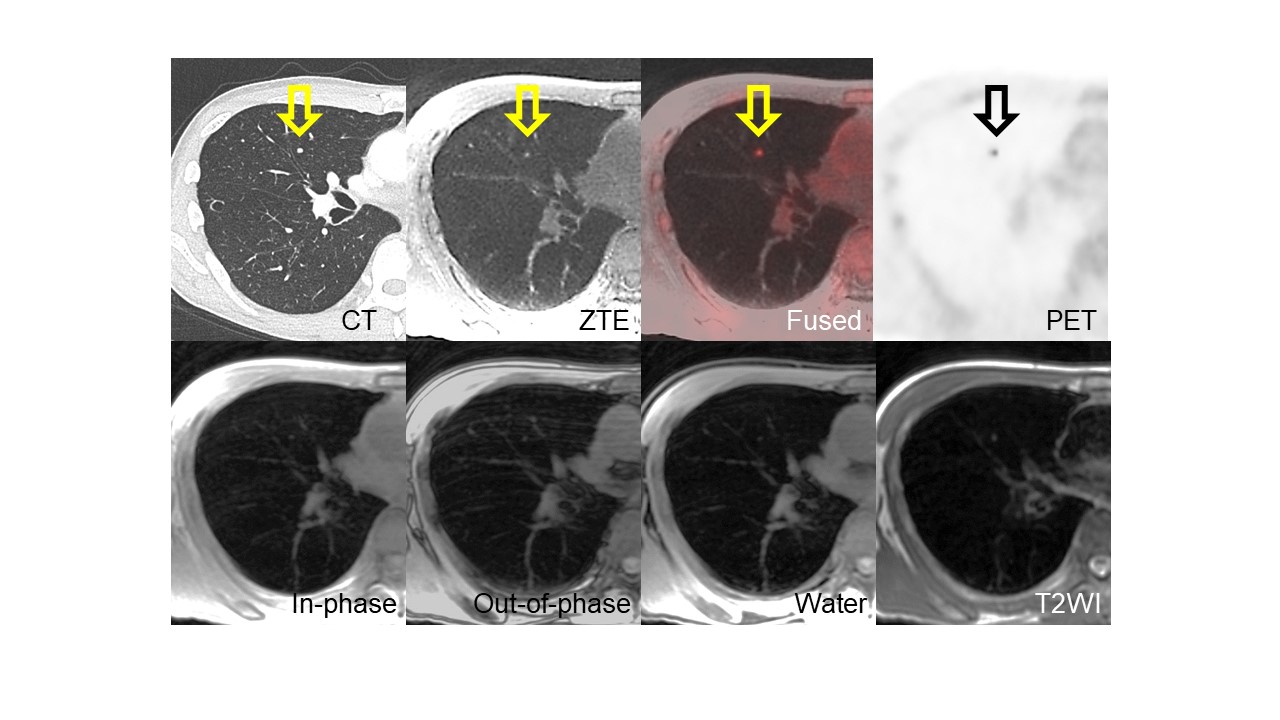
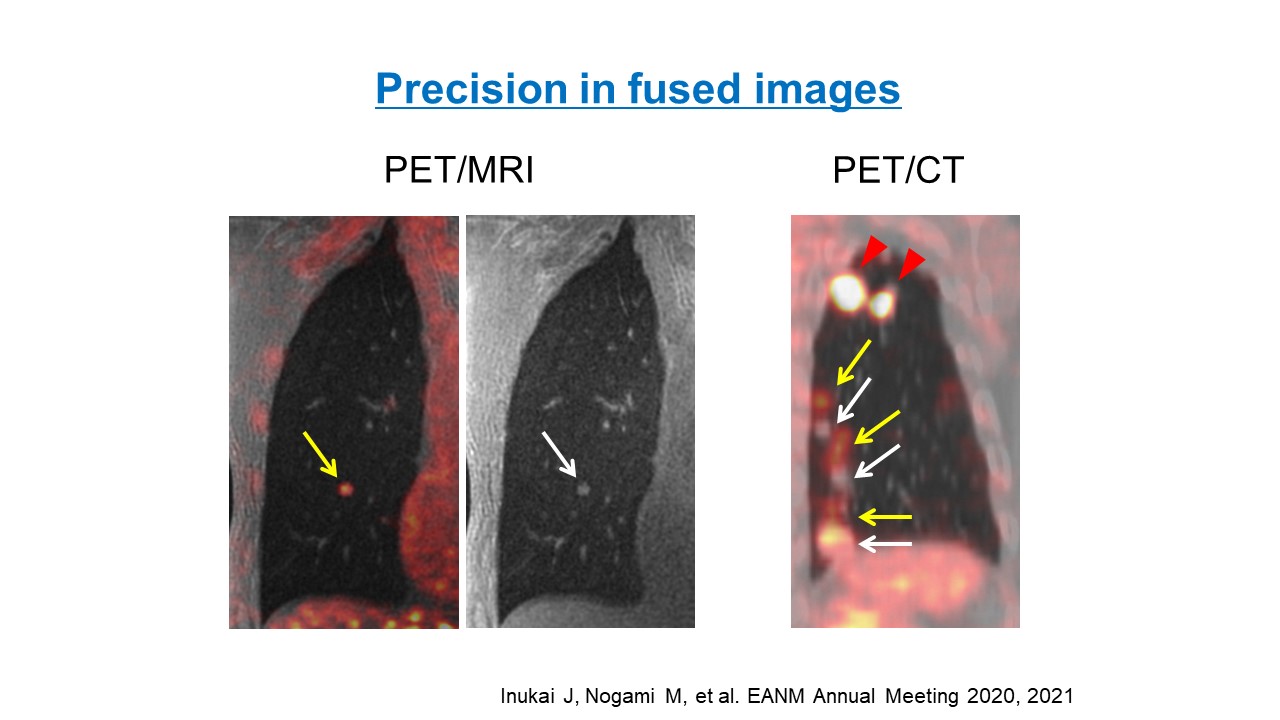
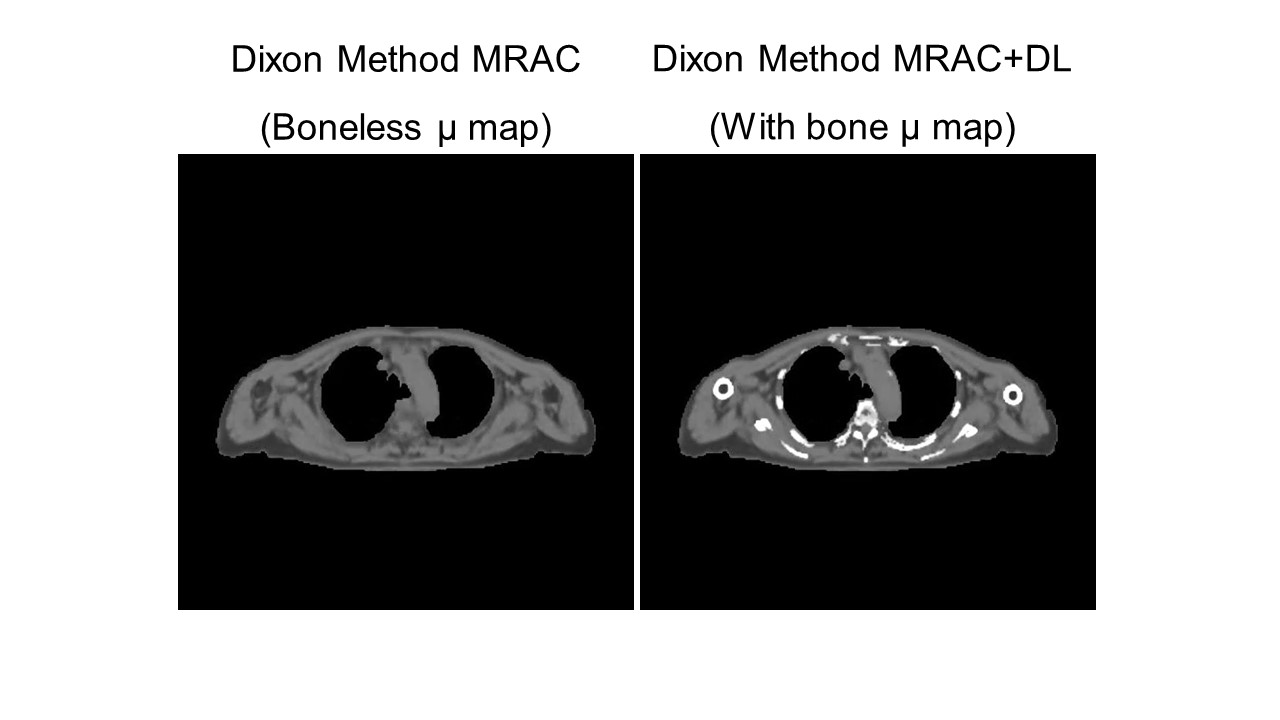
MRI is typically considered inferior to CT for evaluating the lungs due to their low proton density and short T2 relaxation time. However, by using the Ultrashort echo time (UTE) or Zero echo time (ZTE) method, which has a very short or almost zero echo time, organs such as the lungs and bones can be imaged using MRI (Figure 2). PET/MRI offers advantages that PET/CT cannot provide, such as simultaneous acquisition of UTE and ZTE with PET(7). Lung movement during respiratory motion is known to be most significant in the lower lung fields. However, respiratory-gated simultaneous PET/MRI can produce highly accurate fusion images even in the lower lung fields (Figure 3). Another advantage of PET/MRI in the thoracic region is that it can improve attenuation correction errors in PET image reconstruction due to respiratory motion, compared to PET/CT. In PET/CT attenuation correction, an attenuation correction map is generated using CT. However, the attenuation correction in the lower lung field is inaccurate on PET/CT due to respiratory motion(8,9). Since conventional MRI has difficulty delineating bone and lungs, MRI attenuation correction generates maps that ignore bone and lungs, resulting in an underestimation of tracer accumulation. In recent years, pseudo-CT, including bone components generated from ZTE using deep learning(10), has been used for attenuation correction to obtain accurate quantitative values while preventing attenuation correction errors due to respiratory motion (Figure 4).Peristalsis of the digestive tract
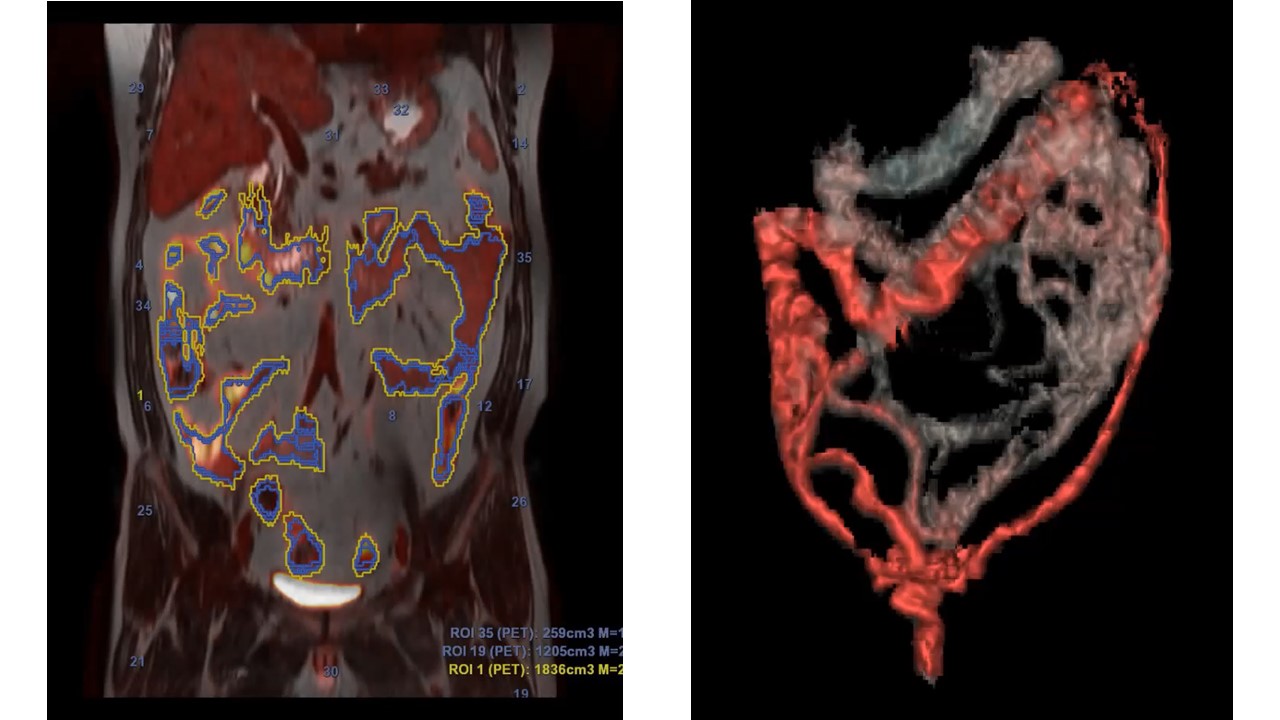
The gastrointestinal tract's peristalsis can also lead to inaccurate fusion images during the examination. Especially when the lumen and wall of the gastrointestinal tract need to be separately evaluated for tracer accumulation, PET/CT is difficult to separate into areas due to its poor fusion image accuracy, and the non-contrast CT used in PET/CT cannot accurately delineate the structure of the gastrointestinal tract due to its poor contrast. Simultaneous PET/MRI acquisition combined with Hyoscine butylbromide makes it possible to quantitatively assess the uptake and excretion of the tracer in the gastrointestinal tract (Figure 5). It was known that patients receiving metformin had a substantial FDG accumulation in the intestinal tract. PET/MRI revealed that this accumulation was not in the wall but in the lumen(11).Even more perfect time-synchronized images: The use of MR active triggers
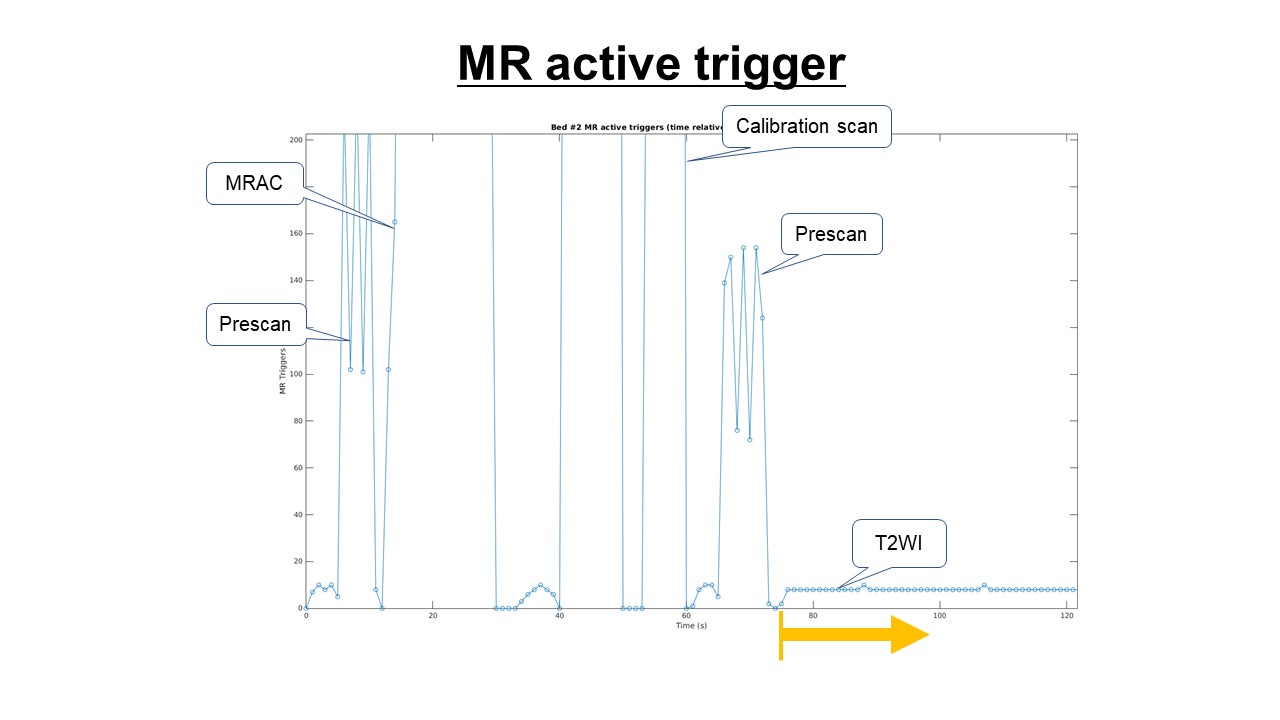
PET consists of a single acquisition method, whereas MRI consists of multiple types of sequences. Therefore, it is necessary to find a solution to obtain PET images that perfectly match the acquisition times of the individual MRIs, even if they are acquired simultaneously. The waveform of the electrical signal sent to the MRI pulse sequence engine is encoded in the PET List-mode data (Figure 6). By retrieving this information, the exact starting and ending time of each MRI sequence can be determined, and accurate fusion images can be obtained by reconstructing PET images that perfectly match the imaging time of each MRI sequence. This time-synchronized PET/MRI allows for a more accurate assessment of local tumor extension and MRI-based PET regions of interest than conventional methods.Conclusions
The advantages of PET/MRI over PET/CT are not only the reduced radiation exposure dose and superior contrast resolution of MRI but also the ability to perform simultaneous acquisitions. Time-synchronized PET/MRI is more valuable than PET/CT for evaluating functional imaging of both PET and MRI over time and for accurately assessing moving organs and lesions in the body.Acknowledgements
No acknowledgement found.References
1. Afaq A, Fraioli F, Sidhu H, et al. Comparison of PET/MRI With PET/CT in the Evaluation of Disease Status in Lymphoma. Clin Nucl Med 2017;42(1):e1-e7.
2. Nakamoto Y, Kitajima K, Toriihara A, Nakajo M, Hirata K. Recent topics of the clinical utility of PET/MRI in oncology and neuroscience. Ann Nucl Med 2022;36(9):798-803.
3. Queiroz MA, Hullner M, Kuhn F, et al. PET/MRI and PET/CT in follow-up of head and neck cancer patients. Eur J Nucl Med Mol Imaging 2014;41(6):1066-1075.
4. Spick C, Herrmann K, Czernin J. 18F-FDG PET/CT and PET/MRI Perform Equally Well in Cancer: Evidence from Studies on More Than 2,300 Patients. J Nucl Med 2016;57(3):420-430.
5. Terao T, Machida Y, Narita K, et al. Total diffusion volume in MRI vs. total lesion glycolysis in PET/CT for tumor volume evaluation of multiple myeloma. Eur Radiol 2021;31(8):6136-6144.
6. Nogami M, Zeng F, Inukai J, et al. Physiological skin FDG uptake: A quantitative and regional distribution assessment using PET/MRI. PLoS One 2021;16(3):e0249304.
7. Zeng F, Nogami M, Ueno YR, et al. Diagnostic performance of zero-TE lung MR imaging in FDG PET/MRI for pulmonary malignancies. Eur Radiol 2020;30(9):4995-5003.
8. Papathanassiou D, Becker S, Amir R, Meneroux B, Liehn JC. Respiratory motion artefact in the liver dome on FDG PET/CT: comparison of attenuation correction with CT and a caesium external source. Eur J Nucl Med Mol Imaging 2005;32(12):1422-1428.
9. Sureshbabu W, Mawlawi O. PET/CT imaging artifacts. J Nucl Med Technol 2005;33(3):156-161; quiz 163-154.
10. Wiesinger F, Bylund M, Yang J, et al. Zero TE-based pseudo-CT image conversion in the head and its application in PET/MR attenuation correction and MR-guided radiation therapy planning. Magn Reson Med 2018;80(4):1440-1451.
11. Morita Y, Nogami M, Sakaguchi K, et al. Enhanced Release of Glucose Into the Intraluminal Space of the Intestine Associated With Metformin Treatment as Revealed by [(18)F]Fluorodeoxyglucose PET-MRI. Diabetes Care 2020;43(8):1796-1802.
Figures