History & Current Status of Non-Contrast-Enhanced MRA Techniques
Martin John Graves1
1Radiology, University of Cambridge, Cambridge, United Kingdom
1Radiology, University of Cambridge, Cambridge, United Kingdom
Synopsis
Keywords: Cardiovascular: Angiography
Non-contrast-enhanced magnetic resonance angiography (NCE-MRA) has evolved considerably since its inception in the mid-1980s. The technique uses flow-related signal changes to visualize the vasculature, without contrast agents. Initially, time-of-flight (TOF) and phase-contrast (PC) were the most common methods. However, limitations such as flow-related artifacts and slow acquisition times, have led to the development of techniques like flow-sensitive dephasing (FSD), balanced steady-state free precession (bSSFP) and quiescent-interval slice-selective (QISS). These methods have shown promise in improving image quality and reducing scan times. NCE-MRA is currently used in clinical practice, particularly for patients with renal insufficiency or contraindications to contrast-enhanced imaging.Introduction
Non-contrast-enhanced magnetic resonance angiography (NCE-MRA) encompasses a wide range of methods for producing images of the human vasculature without the administration of an exogenous contrast agent. The term NCE-MRA did not really come into existence until the technique of contrast-enhanced MRA (CE-MRA) was introduced by Martin Prince in 1994 (1), where the desired vascular territory was imaged during the first pass of a gadolinium-based MR contrast agent (GBCA).Prior to this development the main methods of performing MR angiography either exploited differences in the phase of transverse magnetisation, or differences in the longitudinal magnetization, of blood and stationary tissue. The first MR angiographic image was acquired in 1985 by Van Weeden et al (2) using a spin echo sequence. Using non-selective RF excitation, two projective MR images were obtained, one gated to systole and the other gated to diastole. The amplitude of the readout gradient was calibrated to yield a known velocity-phase relationship. The choice of phase shift resulted in significant phase dispersion, and therefore signal loss, for fast systolic flow velocities but relative preservation of signal for the slower diastolic velocities, whilst the static tissue signal remained the same. Subtraction of the two magnitude images eliminated the static signal and produced a bright blood image of the vasculature. Whilst the technique was only suitable for pulsatile flow in the direction of the readout gradient and was subject to artifacts from patient and vessel movement, it did lead to the rapid development of the first generation of MR angiography methods based on either phase or longitudinal magnetisation effects.
Whilst these NCE-MRA techniques served the imaging community well for a long period they were primarily used for visualisation of the cranial and extracranial circulation. The requirements for imaging the thoracic, abdominal, and peripheral circulation meant these techniques were not particularly successful. The development of CE- MRA allowed high quality imaging of all these regions due to the ability of these techniques to acquire high resolution, high vessel/background contrast, and large field-of-view studies in a relatively short acquisition time. However, in 2006 initial reports emerged of patients with end-stage renal disease (ESRD) developing nephrogenic system fibrosis (NSF) after receiving GBCAs for MRI scans. NSF is a rare and serious systemic condition that affects the skin, joints, and internal organs. It is characterized by excessive deposition of collagen, leading to fibrosis and thickening of tissues. NSF primarily occurs in individuals with pre-existing kidney dysfunction, particularly those with ESRD or acute kidney injury.This spurred the MRI vendors to develop a new generation of NCE-MRA techniques to address the challenges of acquiring high quality angiograms in the body, particularly in those patients with renal insufficiency or contraindications to contrast-enhanced imaging.
Phase Contrast
In 1987 Dumoulin and Hart (3) produced projection angiograms using bipolar flow encoding gradients incorporated into an ECG-triggered gradient refocused echo (GRE) pulse sequence. The amplitude and duration of the flow encoding gradients was controlled by a user supplied velocity encoding (VENC) parameter which determined the phase shift accrued for a given flow velocity. Angiograms were obtained by acquiring two images, each with opposite polarity flow encoding gradients, i.e., positive, and negative phase shifts, and then performing a complex subtraction, i.e., subtracting the raw data before reconstruction and therefore retaining the phase information. Sensitivity to in-plane flow direction was eliminated by performing the experiment twice, firstly with the flow encoding gradients applied along the frequency encoding direction and then secondly with them applied along the phase encoding direction. Images of the two orthogonal components of flow were then combined, using the theorem of Pythagoras, into a single speed, i.e., independent of direction, image. This approach requires twice the acquisition time and is sensitive to misregistration between the two acquisitions.An alternative technique based on a multi-echo sequence was subsequently proposed that permitted the simultaneous acquisition of orthogonal flow directions as separate echoes (4). These projection methods also incorporated an additional dephasing gradient applied along the projection direction to reduce the large signal from stationary spins, thereby maximising the dynamic range for vessels.
Further improvements in acquisition speed and image quality were presented by Dumoulin et al (5) in 1987. Projection angiograms were acquired not by using cardiac synchronisation, with the repetition time (TR) equal to the R-R interval, but by averaging many echoes per phase encoding step, typically 30-64, with a short TR (33ms). Sensitivity to patient motion was reduced by inverting the flow encoding gradients on alternate acquisitions, i.e., every TR. Since this method produced angiograms reflecting only average blood flow the basic cardiac synchronised method was combined with the short TR concept to produce dynamic projection angiograms at different times, or phases, within the cardiac cycle (6). Cine display of the angiograms demonstrated the temporal variations in blood flow throughout the cardiac cycle. Techniques to compensate for the phase shift acquired by spins moving with constant velocity along a magnetic field gradient (7), were also employed to produce MR angiograms.
Axel (8) proposed a method for projection angiography involving the subtraction of a velocity-compensated SE image, in which vascular signal is high, from a non-velocity-compensated SE image in which the vascular signal is reduced through dephasing. Similar techniques were also employed by Laub et al (9) who used an ECG-triggered SE sequence with different trigger delays to selectively image arteries and veins. They extended their work further by using velocity compensated and uncompensated three-dimensional (3D) GRE sequences. Following slice-by-slice subtraction, projective angiograms were produced by casting parallel rays through the tomographic volume and displaying only the maximum intensity along each ray (10). Retrospective calculation of projections using this "maximum intensity projection" (MIP) algorithm at small angular increments, followed by display in a cine loop format, gave a very strong 3D illusion of the vasculature.
These velocity compensated/uncompensated techniques were, however, limited to looking at unidirectional flow along the axis of the velocity compensated gradient. A major advance in phase contrast angiography came in 1989 when Dumoulin et al (11) described the method of 3D phase contrast angiography. A volumetric GRE sequence was used with bipolar velocity encoding gradients applied along each gradient direction in turn resulting in a six-measurement acquisition, i.e., positive, and negative phase shifts along each orthogonal axis. The raw data from the two velocity encodings were subtracted to eliminate the static tissue signal and image volumes for each velocity direction reconstructed by 3D Fourier transformation. The three volumes were then combined on a pixel-by-pixel basis into a single speed volume using the theorem of Pythagoras. The angiogram was finally produced by MIP through the speed volume. This 3D technique provides small, almost isotropic, voxels which minimise the phase dispersion across the voxel, thereby reducing many of the artifacts encountered in thick section projection angiograms, e.g., signal cancellation from overlapping vessels.
The major disadvantage of the technique however is the long scan time, requiring six excitations to produce an angiogram. In principle only four measurements are required, one reference i.e., no velocity sensitivity, and three sensitive to velocity along each orthogonal direction (12, 13). Subtraction of each velocity sensitive image from the reference yields the velocity-only image for that direction. The use of one image as the reference is sub-optimal from an SNR point of view and a more efficient subtraction scheme based on a Hadamard multiplexing scheme is usually employed (14). This method also has the advantage of providing a stationary tissue image in addition to the three velocity component images. The 3D phase contrast MRA technique as described by Dumoulin et al employed complex subtraction of the two velocity encodings along each direction before combination into a final speed image. An alternative processing method is to reconstruct the phase images for each encoding and then perform the subtraction. This has the advantage of providing quantitative information on the magnitude and direction of blood flow. Providing the gradients are correctly calibrated there is a linear relationship between the blood velocity and the measured phase shift, controlled by the VENC parameter. The value of the phase shift can be used to calculate the component of the velocity vector parallel to the encoding gradient axis whilst its sign represents the direction along that axis. Providing the VENC is chosen such that the maximum velocity does not exceed a phase shift of 180° then the velocity and its direction will be unambiguous. Should the phase shift exceed 180° then the velocity will alias, leading to incorrect measurements unless the aliasing is noted and corrected.
Angiograms can still be produced from phase difference data by simply combining the orthogonal phase images using the theorem of Pythagoras. The velocity magnitude and direction information will be lost but a conventional MR angiographic display, i.e., bright vessels on a dark background will result. It should be noted that phase difference processing is only suitable for thin slice data acquisition, i.e., 3D techniques, thick slab 2D techniques require complex difference processing to avoid image artifacts (15).
Time-of-flight
The time-of-flight (TOF) phenomena has been the basis of a rich variety of angiographic techniques. The initial methods relied on stationary signal suppression via subtraction of two acquisitions differing only in the selective labelling of moving spins outside the imaged region. Dixon et al (16) used an inversion labelling approach to produce projection angiograms of the carotid and vertebral arteries. A small surface coil placed on the neck is used to invert the magnetisation of flowing spins moving along a magnetic field gradient parallel to the vessel. The change in Larmor frequency as the spins move along the gradient satisfies the condition for an adiabatic free passage (AFP) inversion. Adiabatic inversion pulses have the advantage of inducing uniform 180° rotation of the magnetisation from the z to the -z axis even in the presence of large variations in RF field homogeneity. By subtracting two acquisitions one with and one without the inversion the stationary signal can be cancelled leaving only the blood signal. The detectable range of the spins motion however is limited by its velocity and the T1 lifetime of the inversion.An alternative spin labelling approach was taken by Nishimura et al (17). A selective 180° pulse was used to invert the magnetisation in the slab of interest. An inversion time (TI) was then allowed for uninverted blood to flow into the slab before a SE readout. The sequence was then repeated with a non-selective 180° pulse to invert all the spins followed by complex subtraction of the data. This method was used to produce projection angiograms of the carotid arteries.
Presaturation pulses have also been used as a method of spin labelling. Dumoulin et al (18), using a 3D velocity compensated GRE sequence in the neck, acquired volumetric images with and without presaturation slabs positioned proximally or distally to the imaging volume. The velocity compensation ensured that the vascular signal was bright whilst the presaturation pulses could be used to selectively destroy the longitudinal magnetisation of spins flowing into the volume from either above or below. Subtraction of the two volumes cancelled the stationary signal and yielded selective images of arteries or veins depending on the position of the presaturation slab. Angiographic projections were produced using MIP and shaded surface displays. The obvious disadvantage is in the necessity to acquire two volumetric acquisitions.
The current, most widely employed, method of producing TOF angiograms suppresses the stationary tissue by saturation of its longitudinal magnetisation. This was first proposed in 1989 using both a 3D volumetric acquisition technique (19) and a sequential slice 2D acquisition technique (20). Both methods employed short echo time (TE), velocity compensated, partial flip angle, GRE sequences to maximise the vascular signal whilst simultaneously minimising the stationary tissue signal by judicious choice of TR and flip angle. The capability of the 3D technique to produce thin slices and therefore small voxels offers several advantages for producing angiograms. Firstly, the use of small voxels reduces the intravoxel phase dispersion and thereby reduces signal loss. Secondly the use of a volumetric acquisition provides high resolution with good signal-to-noise ratio (SNR) ideal for looking at small tortuous vessels, e.g., the intracerebral arterial circulation (19). Finally, because the sequence excites a thick slab of tissue short duration RF pulses can be used, reducing the TE.However, volumetric acquisitions suffer from progressive signal saturation further into the volume as the flowing spins experience multiple excitations.
In comparison with the 3D technique, the 2D sequential slice technique employs slices that are thin compared with the 3D slab thickness but are relatively thick in comparison with the effective 3D slice thickness. The use of thin, sequential, 2D slices means that despite the poor SNR the flow/stationary tissue contrast in each slice is always maximal, even for quite slow flow. The 2D method is therefore suited to looking at slow flow, e.g., the venous circulation and for acquiring data over a long segment of vessel without saturation effects (21). However, the larger voxel size, combined with the longer TE required to excite a thin 2D slice rather than a thick 3D volume, means that the 2D method will always suffer more from intravoxel phase dispersion (22). To reduce the high background signal from stationary tissue in 3D acquisitions, the technique of magnetization transfer (MT) is often used (23, 24).
MT refers to the process whereby protons associated with unbound, or free, water molecules can exchange their spin energy with other protons bound to macromolecules. Protons that are bound to macromolecules have very short T2 relaxation times and hence very broad resonances. These protons are therefore essentially 'invisible' to conventional MR imaging. To perform MT background suppression, a high-power, off-resonance (typically 1–2 kHz), RF pulse is used to saturate the magnetization of protons in the bound pool. When these protons exchange their magnetization with the free protons, there is a significant reduction in the signal from tissues. In the brain, the signal from grey and white matter can be reduced whilst the signal from moving blood, which does not exhibit a significant MT effect, is relatively unaffected. The result is an overall improvement in vessel contrast. The use of MT also has a few disadvantages. First there is increase in RF power deposition because of the high- power MT pulse. Second it is necessary to increase TR and thus the total scan time to play out the pulse, although this improves in-flow effects. Finally, fat tends to be more conspicuous since lipids do not exhibit significant MT effects either.
A further limitation of 3D TOF techniques is known as progressive saturation. Repeatedly exciting a thick slab of tissue means that the signal from flowing spins gradually saturates as the spins penetrate more distally into the volume, i.e., spins progressively experience more RF pulses the longer they remain within the volume. Although the signal loss can be reduced using small imaging flip angles, e.g., 25°, this is at the expense of an overall reduction in vascular contrast. There are two sequence improvements that help to reduce this effect. The first is the use of a 2D/3D hybrid technique, often termed MOTSA (Multiple Overlapping Thin Slab Acquisition) (25). This method aims to reduce the saturation effect by reducing the thickness of the 3D slab but maintaining the volume coverage by using multiple slabs. The 3D slab profile effect is ameliorated by slightly overlapping the slabs and discarding the overlapping slices when doing the final MIP, however this can sometimes cause an artifact commonly known as the 'venetian blind’ effect, where there is a noticeable signal intensity transition between each slab.
The second improvement is the use of ramped RF excitation pulses, e.g., TONE, (Tilted Optimised Non-saturating Excitation), which are specially designed pulses that increase the flip angle across the 3D acquisition volume (26, 27). Instead of exciting a flat-topped rectangular slab profile, the profile is a trapezoid with a linear variation of flip angle with position through the slab. The ramp direction is set so that the higher flip angles further into the scan are downstream of the blood flow to help compensate for the saturation, whilst the lower flip angles are at the start of the scan to ensure that the spins are not saturated too early. The combination of MT, MOTSA and ramped RF (TONE) allows us to acquire high-resolution TOF angiograms of the intra- and extra-cerebral circulation.
Next Generation NCE-MRA Methods
The initial leaders in the field of whole-body NCE-MRA methods development was the Toshiba, now Canon, MRI research group led by Dr Mitsue Miyazki. The most successful technique being that of ECG-triggered, inversion-recovery prepared, 3D fast spin echo (28, 29), often referred to as “fresh-blood imaging” (FBI). Two segmented 3D acquisitions are performed; the first is acquired in systole and the second in diastole. In the systolic images fast arterial flow results in signal dephasing and a reduction in intravascular signal. In the diastolic image the arterial flow is relatively slow and therefore appears as a high signal. Venous flow is relatively slow throughout the cardiac cycle and therefore appears bright in both acquisitions. Bright blood images are therefore obtained by magnitude subtraction of the matching systolic images from the diastolic images. Limitations of the technique include spatial misregistration between the two acquisitions, each often taking several minutes, and T2 blurring caused by fast spin echo readout during the intrinsic T2 decay. The use of parallel imaging techniques to reduce the length of the echo train can be used to reduce these effects. There is also a requirement to perform an “ECG-Prep” scan to identify the optimal systolic and diastolic trigger delays for each body area.Balanced steady-state-free-precession (bSSFP) sequences have also been used as NCE-MRA techniques due to their high T2/T1 contrast weighting which is well matched to the intrinsic relaxation times of blood resulting in a high signal from blood, relatively independent of flow. This method is particularly effective given that bSSFP sequences operate best with very short TEs and TRs. ECG and respiratory-triggered 3D bSSFP techniques have been used in many body areas including the coronaries (30) and thoracic aorta (31). However, a disadvantage of standard 3D bSSFP sequences is that both arteries and veins appear bright as well as background tissues.
This led to the development of arterial spin labelling or tagging preparations of various combinations (32). One example is a method for renal artery MRA in which a spatially selective inversion pulse is applied prior to a smaller spatially selective 3D bSSFP readout The inversion time between tag and the readout is chosen such that the background signal, including the inferior vena cava, is suppressed and there is time for inflow of arterial spins into the imaging volume. Respiratory triggering is used to reduce misregistration artefacts.
In a similar fashion to the FBI technique presented above bSSFP techniques have also been used for peripheral vascular angiography. The most popular implementation being that of quiescent-interval single-shot (QISS) MRA (33). In QISS, an in-plane RF saturation pulse is applied to suppress the background signal, and a tracking RF saturation pulse is used to suppress venous signal. These pulses help improve image quality by selectively saturating unwanted signals. Immediately after the RF saturation pulses, a quiescent interval is introduced. This interval coincides with the period of rapid systolic flow and ensures that the saturated in-plane spins are replaced by unsaturated ones before the balanced steady-state free precession (bSSFP) readout. QISS also uses fat saturation for better visualization of the blood vessels of interest. QISS acquires groups of 40-50 axial slices per station, with each station imaged near the magnet isocenter. This approach helps minimize off-resonance effects that can distort the images. To further improve vessel visualisation a reference "mask image", without applying the saturation pulses, can be acquired and subtracted from the QISS data.
bSSFP techniques have also been used to produce angiographic images using flow sensitive dephasing (FSD) a subtraction technique but with the blood suppression being created using a motion-sensitised driven equilibrium (MSDE) preparation, rather than the inherent flow-spoiling of FSE in the readout direction used in FBI. This is essentially a weak diffusion preparation scheme that dephases rapidly flowing arterial blood. Subtraction of two acquisitions with and without MSDE results in an angiographic image (34).
Recently Edelman and Koktzoglou recently introduced a modification of bSSFP method known as Balanced T1 Relaxation-Enhanced Steady-State (bT1RESS) which provides the basis for a simplified approach to NCE-MRA (35). bT1RESS uses an ungated continuous data acquisition where background suppression is achieved by imparting a flexible amount of T1 weighting to a bSSFP acquisition using periodically applied contrast-modifying (CMα) RF pulses. T1-weighting increases with larger CMα flip angles and shorter CMα TR. A fast interrupted steady-state (FISS) readout (36) is used with RF spoiling performed across FISS modules. With FISS, the steady-state magnetization is intermittently stored along the z-axis by a α/2 excitation RF pulse, with gradient and quadratic RF spoiling, followed by a restore α/2 excitation RF pulse to resume the steady-state. Data are collected using a radial k-space trajectory and optimized azimuthal view angles (37).
Finally, there is the NCE-MRA method of Velocity-Selective Magnetic Resonance Angiography (VS-MRA) a Fourier-based velocity-selective magnetization preparation, which produces image contrast by altering the amplitude and phase of each magnetic spin based solely on its velocity, regardless of its spatial location (38). Since the VS preparation is spatially non-selective it can be used with a 3D bSSFP or GRE readout, depending on field strength, enabling a high spatial resolution and a large field of view in all three dimensions. By assigning velocity pass and stop bands properly, the VS preparation can suppress background tissues without affecting arterial blood, thus forming an angiogram. Additionally, VS preparation generates positive angiographic contrast from a single acquisition, unlike subtractive 3D approaches. With cardiac gating and an appropriate trigger delay, a VS preparation pulse is played close to the time of peak systolic flow, followed by a fat saturation pulse and a 3D segmented data acquisition as used in other magnetization prepared imaging. VS-MRA has been found to be feasible for a variety of vascular territories, including renal, abdominal, pedal, and cerebral arteries however the VS preparation scheme is vulnerable to B0 and B1 field errors, which have been addressed in various versions to minimize their effects (39, 40). Other potential issues include inadequate depiction of very slow arterial flow and difficult suppression of fast venous flow.
Summary
There is a plethora of NCE-MRA techniques described in the literature and several excellent review articles (41-47). The techniques primarily based around one or more aspects of- Longitudinal magnetisation recovery
- Transverse phase modulation
- Stationary tissue suppression
- Sensitivity of bSSFP to the high T2/T1 of blood
Acknowledgements
Thanks to colleagues in the University of Cambridge Department of Radiology and Cambridge University Hospitals Department of Imaging.References
- Prince MR. Gadolinium-enhanced MR aortography. Radiology. 1994;191(1):155-64.
- Wedeen VJ, Meuli RA, Edelman RR, Geller SC, Frank LR, Brady TJ, et al. Projective imaging of pulsatile flow with magnetic resonance. Science. 1985;230(4728):946-8.
- Dumoulin CL, Hart HR, Jr. Magnetic resonance angiography. Radiology. 1986;161(3):717-20.
- Dumoulin CL, Souza SP, Feng H. Multiecho magnetic resonance angiography. Magn Reson Med. 1987;5(1):47-57.
- Dumoulin CL, Souza SP, Hart HR. Rapid scan magnetic resonance angiography. Magn Reson Med. 1987;5(3):238-45.
- Dumoulin CL, Souza SP, Walker MF, Yoshitome E. Time-resolved magnetic resonance angiography. Magn Reson Med. 1988;6(3):275-86.
- Haacke EM, Lenz GW. Improving MR image quality in the presence of motion by using rephasing gradients. AJR Am J Roentgenol. 1987;148(6):1251-8.
- Axel L, Morton D. MR flow imaging by velocity-compensated/uncompensated difference images. J Comput Assist Tomogr. 1987;11(1):31-4.
- Laub GA, Kaiser WA. MR angiography with gradient motion refocusing. J Comput Assist Tomogr. 1988;12(3):377-82.
- Rossnick S, Laub G, Braeckle R, al. e, editors. Three dimensional display of blood vessels in MRI. Proceedings of the IEEE Computers in Cardiology Conference; 1987.
- Dumoulin CL, Souza SP, Walker MF, Wagle W. Three-dimensional phase contrast angiography. Magn Reson Med. 1989;9(1):139-49.
- Pelc NJ, Bernstein MA, Shimakawa A, Glover GH. Encoding strategies for three-direction phase-contrast MR imaging of flow. J Magn Reson Imaging. 1991;1(4):405-13.
- Hausmann R, Lewin JS, Laub G. Phase-contrast MR angiography with reduced acquisition time: new concepts in sequence design. J Magn Reson Imaging. 1991;1(4):415-22.
- Dumoulin CL, Souza SP, Darrow RD, Pelc NJ, Adams WJ, Ash SA. Simultaneous acquisition of phase-contrast angiograms and stationary-tissue images with Hadamard encoding of flow-induced phase shifts. J Magn Reson Imaging. 1991;1(4):399-404.
- Bernstein MA, Ikezaki Y. Comparison of phase-difference and complex-difference processing in phase-contrast MR angiography. J Magn Reson Imaging. 1991;1(6):725-9.
- Dixon WT, Du LN, Faul DD, Gado M, Rossnick S. Projection angiograms of blood labeled by adiabatic fast passage. Magn Reson Med. 1986;3(3):454-62.
- Nishimura DG, Macovski A, Pauly JM, Conolly SM. MR angiography by selective inversion recovery. Magn Reson Med. 1987;4(2):193-202.
- Dumoulin CL, Cline HE, Souza SP, Wagle WA, Walker MF. Three-dimensional time-of-flight magnetic resonance angiography using spin saturation. Magn Reson Med. 1989;11(1):35-46.
- Ruggieri PM, Laub GA, Masaryk TJ, Modic MT. Intracranial circulation: pulse-sequence considerations in three-dimensional (volume) MR angiography. Radiology. 1989;171(3):785-91.
- Keller PJ, Drayer BP, Fram EK, Williams KD, Dumoulin CL, Souza SP. MR angiography with two-dimensional acquisition and three-dimensional display. Work in progress. Radiology. 1989;173(2):527-32.
- Mattle HP, Wentz KU, Edelman RR, Wallner B, Finn JP, Barnes P, et al. Cerebral venography with MR. Radiology. 1991;178(2):453-8.
- Litt AW, Eidelman EM, Pinto RS, Riles TS, McLachlan SJ, Schwartzenberg S, et al. Diagnosis of carotid artery stenosis: comparison of 2DFT time-of-flight MR angiography with contrast angiography in 50 patients. AJNR Am J Neuroradiol. 1991;12(1):149-54.
- Pike GB, Hu BS, Glover GH, Enzmann DR. Magnetization transfer time-of-flight magnetic resonance angiography. Magn Reson Med. 1992;25(2):372-9.
- Edelman RR, Ahn SS, Chien D, Li W, Goldmann A, Mantello M, et al. Improved time-of-flight MR angiography of the brain with magnetization transfer contrast. Radiology. 1992;184(2):395-9.
- Parker DL, Yuan C, Blatter DD. MR angiography by multiple thin slab 3D acquisition. Magn Reson Med. 1991;17(2):434-51.
- Ikushima I, Korogi Y, Hirai T, Takahashi M. Variable tip angle slab selection pulses for carotid and cerebral time-of-flight MR angiography. Theory and experimental analysis. Acta Radiol. 1997;38(2):275-80.
- Nagele T, Klose U, Grodd W, Nusslin F, Voigt K. Nonlinear excitation profiles for three-dimensional inflow MR angiography. J Magn Reson Imaging. 1995;5(4):416-20.
- Miyazaki M, Sugiura S, Tateishi F, Wada H, Kassai Y, Abe H. Non-contrast-enhanced MR angiography using 3D ECG-synchronized half-Fourier fast spin echo. J Magn Reson Imaging. 2000;12(5):776-83.
- Miyazaki M, Takai H, Sugiura S, Wada H, Kuwahara R, Urata J. Peripheral MR angiography: separation of arteries from veins with flow-spoiled gradient pulses in electrocardiography-triggered three-dimensional half-Fourier fast spin-echo imaging. Radiology. 2003;227(3):890-6.
- Deshpande VS, Shea SM, Laub G, Simonetti OP, Finn JP, Li D. 3D magnetization-prepared true-FISP: a new technique for imaging coronary arteries. Magn Reson Med. 2001;46(3):494-502.
- Pereles FS, McCarthy RM, Baskaran V, Carr JC, Kapoor V, Krupinski EA, et al. Thoracic aortic dissection and aneurysm: evaluation with nonenhanced true FISP MR angiography in less than 4 minutes. Radiology. 2002;223(1):270-4.
- Ito K, Koike S, Jo C, Shimizu A, Kanazawa H, Miyazaki M, et al. Intraportal venous flow distribution: evaluation with single breath-hold ECG-triggered three-dimensional half-Fourier fast spin-echo MR imaging and a selective inversion-recovery tagging pulse. AJR Am J Roentgenol. 2002;178(2):343-8.
- Edelman RR, Sheehan JJ, Dunkle E, Schindler N, Carr J, Koktzoglou I. Quiescent-interval single-shot unenhanced magnetic resonance angiography of peripheral vascular disease: Technical considerations and clinical feasibility. Magn Reson Med. 2010;63(4):951-8.
- Priest AN, Graves MJ, Lomas DJ. Non-contrast-enhanced vascular magnetic resonance imaging using flow-dependent preparation with subtraction. Magn Reson Med. 2012;67(3):628-37.
- Edelman RR, Koktzoglou I. "Push-button" noncontrast MR angiography using balanced T(1) relaxation-enhanced steady-state (bT1RESS). Magn Reson Med. 2021;85(3):1248-57.
- Koktzoglou I, Edelman RR. Radial fast interrupted steady-state (FISS) magnetic resonance imaging. Magn Reson Med. 2018;79(4):2077-86.
- Edelman RR, Giri S, Murphy IG, Flanagan O, Speier P, Koktzoglou I. Ungated radial quiescent-inflow single-shot (UnQISS) magnetic resonance angiography using optimized azimuthal equidistant projections. Magn Reson Med. 2014;72(6):1522-9.
- Shin T, Worters PW, Hu BS, Nishimura DG. Non-contrast-enhanced renal and abdominal MR angiography using velocity-selective inversion preparation. Magn Reson Med. 2013;69(5):1268-75.
- Shin T, Qin Q, Park JY, Crawford RS, Rajagopalan S. Identification and reduction of image artifacts in non-contrast-enhanced velocity-selective peripheral angiography at 3T. Magn Reson Med. 2016;76(2):466-77.
- Shin T, Qin Q. Characterization and suppression of stripe artifact in velocity-selective magnetization-prepared unenhanced MR angiography. Magn Reson Med. 2018;80(5):1997-2005.
- Graves MJ. Magnetic resonance angiography. Br J Radiol. 1997;70:6-28.
- Miyazaki M, Lee VS. Nonenhanced MR angiography. Radiology. 2008;248(1):20-43.
- Miyazaki M, Akahane M. Non-contrast enhanced MR angiography: Established techniques. J Magn Reson Imaging. 2011;35(1):1-19.
- Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging. 2012;36(2):286-304.
- Edelman RR, Koktzoglou I. Noncontrast MR angiography: An update. J Magn Reson Imaging. 2019;49(2):355-73.
- Navot B, Hecht EM, Lim RP, Edelman RR, Koktzoglou I. MR Angiography Series: Fundamentals of Non-Contrast-enhanced MR Angiography. Radiographics. 2021;41(5):E157-E8.
- Shin T. Principles of Magnetic Resonance Angiography Techniques. Investig Magn Reson Imaging. 2021;25(4):209-17.
Figures
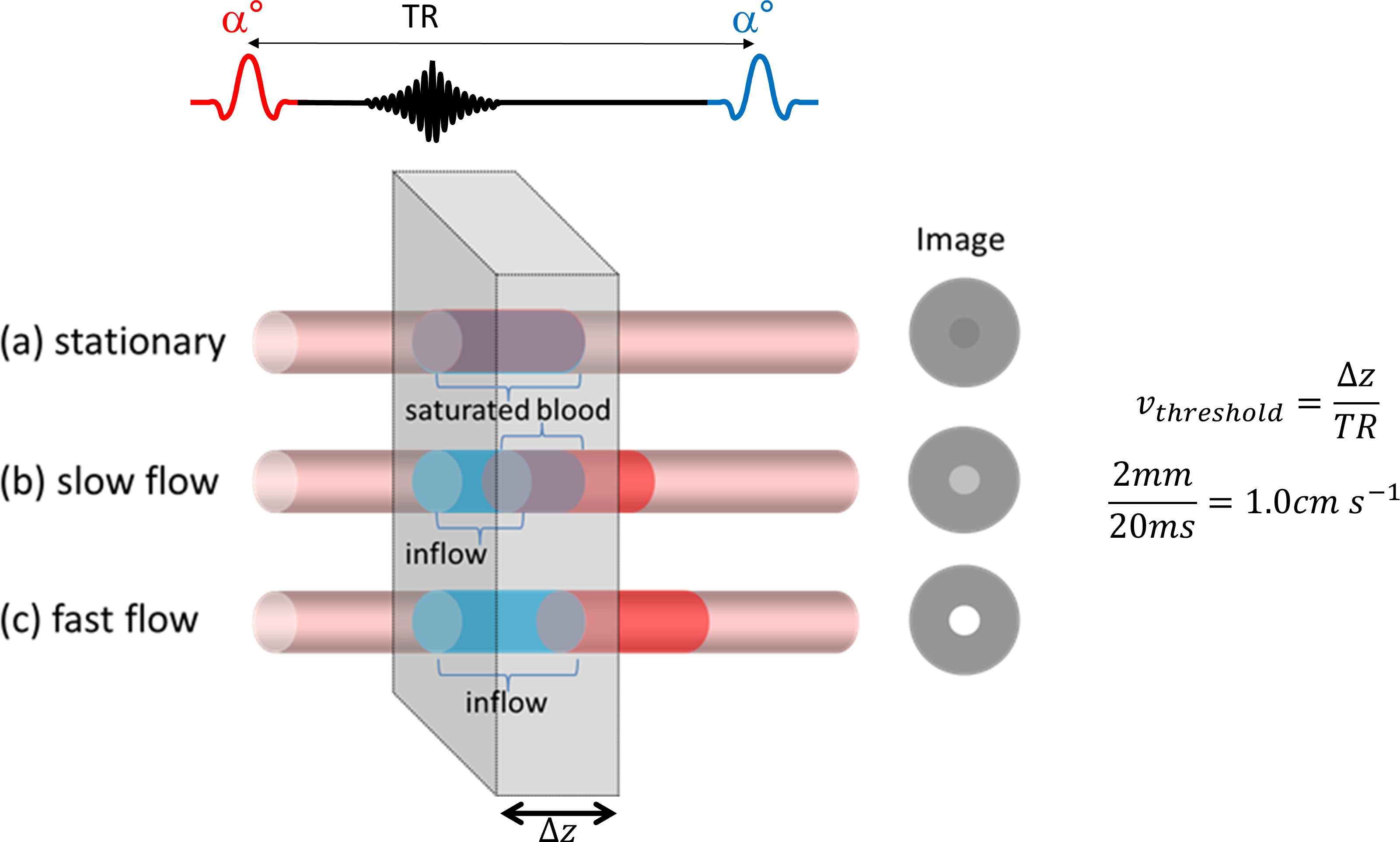
Figure 1.Time-of-flight
effect in gradient echo imaging. When blood is stationary it becomes saturated
like other tissues with long T1 and has reduced signal. When v ≥ Δz/TR maximal in-flow is observed. At intermediate blood velocities there is
increased signal due to the partial inflow of fresh blood, i.e. blood that has not experienced any prior RF excitation and has maximum magnetisation.
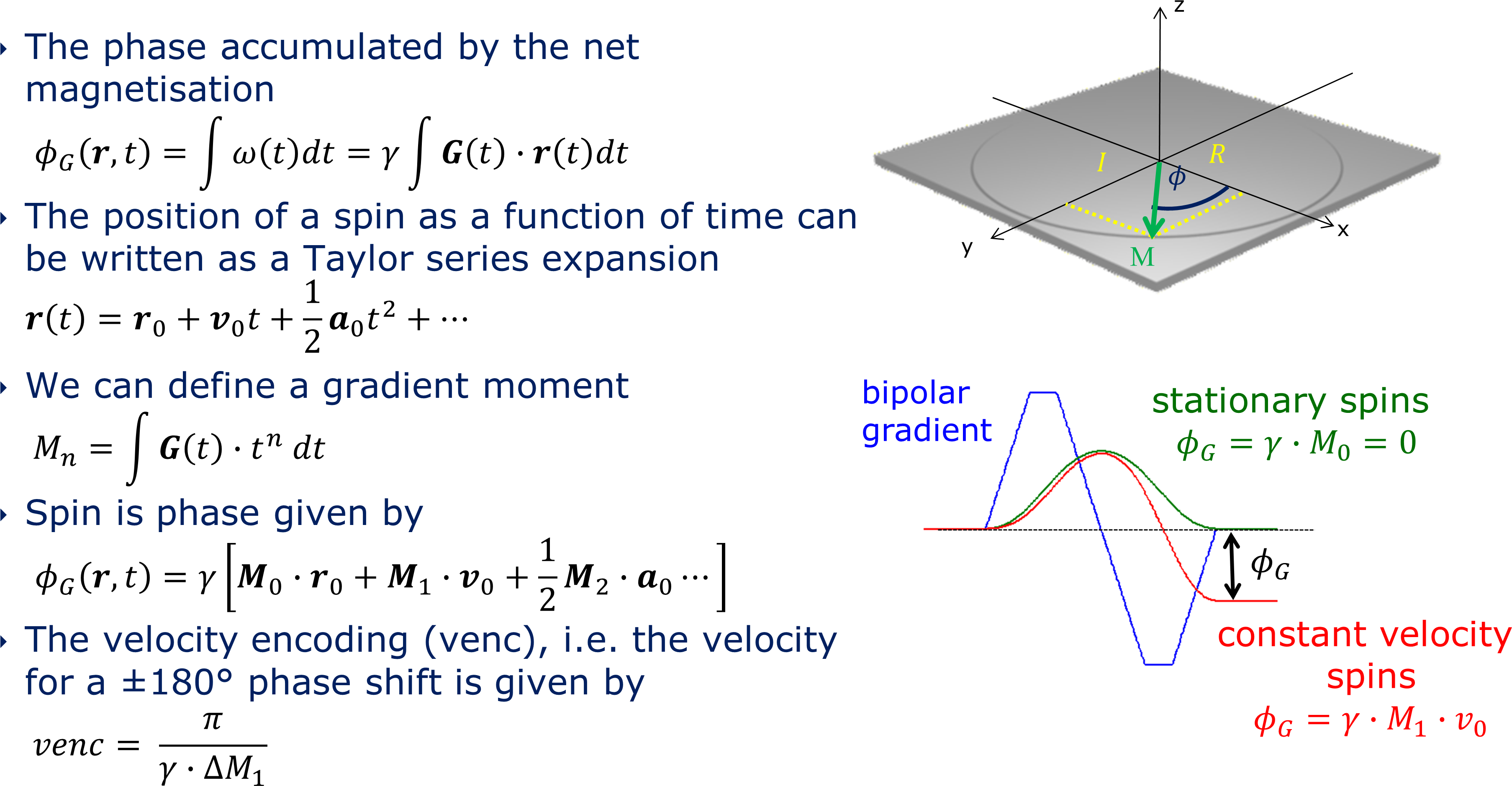
Figure 2. Principles of phase contrast imaging. MRI data is acquired in quadrature, allowing the determination of both the signal magnitude and phase. A bipolar gradient with equal areas has a zeroth order gradient moment M0 = 0, i.e., zero phase shift for stationary spins. However, it has a non-zero first order moment M1 = φG / γ v0 for spins moving with a constant velocity The gradient amplitudes and duration can be adjusted to give a known phase shift, typically 180°, for a given velocity. This is known as the velocity encoding or venc.
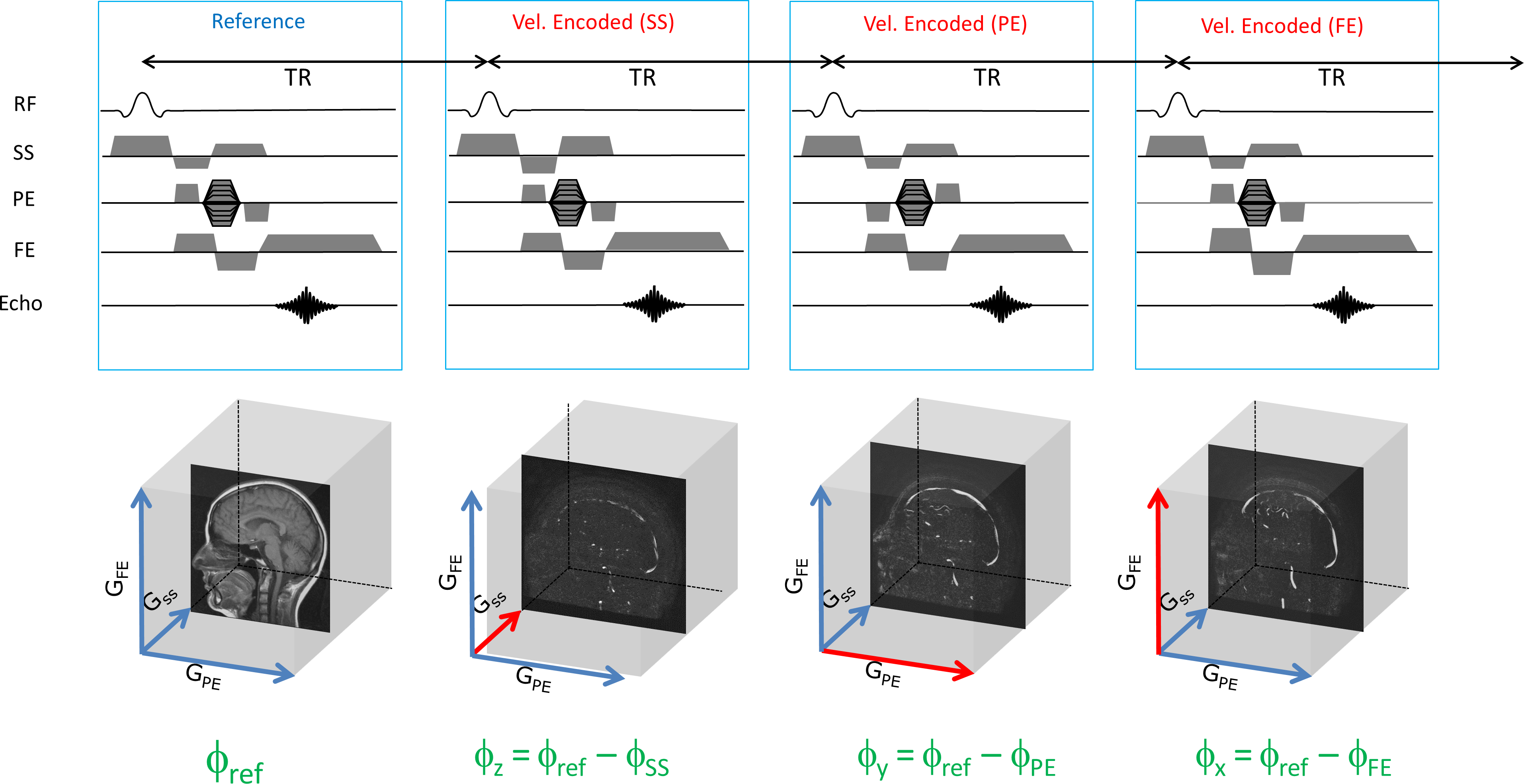
Figure 3. 3D PC MRA acquisition. A reference
acquisition is performed with M1 = 0 followed by further acquisitions which are sensitised
to velocity induced phase shifts along the three orthogonal directions. Each directional phase image is then subtracted from the reference phase. The individual phase subtraction images for each flow
direction are then combined into a directionally independent speed image.
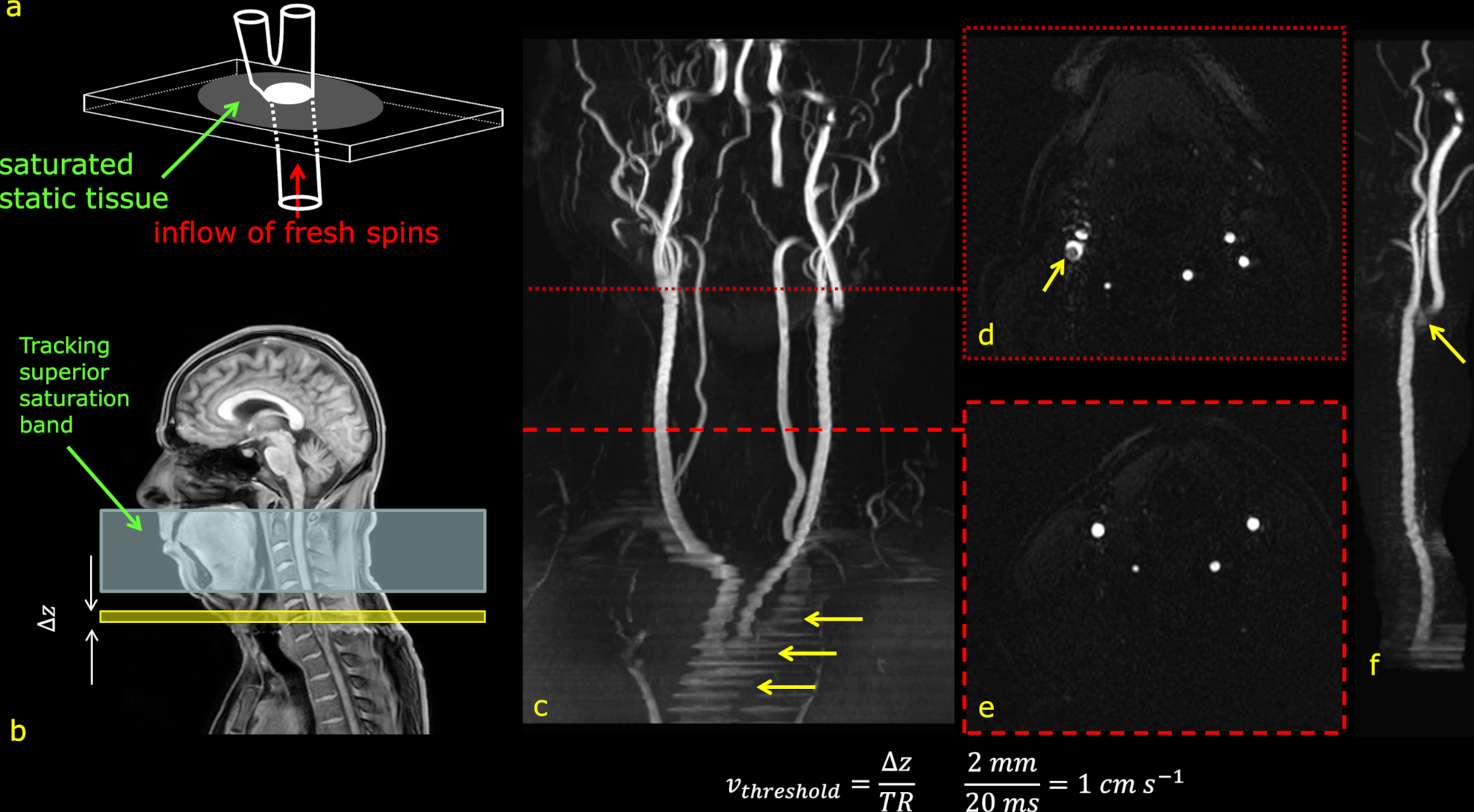
Figure 4. Principles of 2D time-of-flight (TOF) MRA. a) the static tissue is saturated by a large excitation flip angle and short TR. Inflowing, previously unexcited spins, yield a high signal. b) a superior saturation band suppresses the flow in the opposite direction. c) and f) large FOV MIPs of the carotid arteries from the aortic arch (arrowed). d) signal loss around the carotid bifurcation due to recirculant flow (arrow). e) normal appearance of the common carotid arteries. f) signal loss due to transverse flow (arrowed). The threshold for maximal signal is low due to the thin slice.
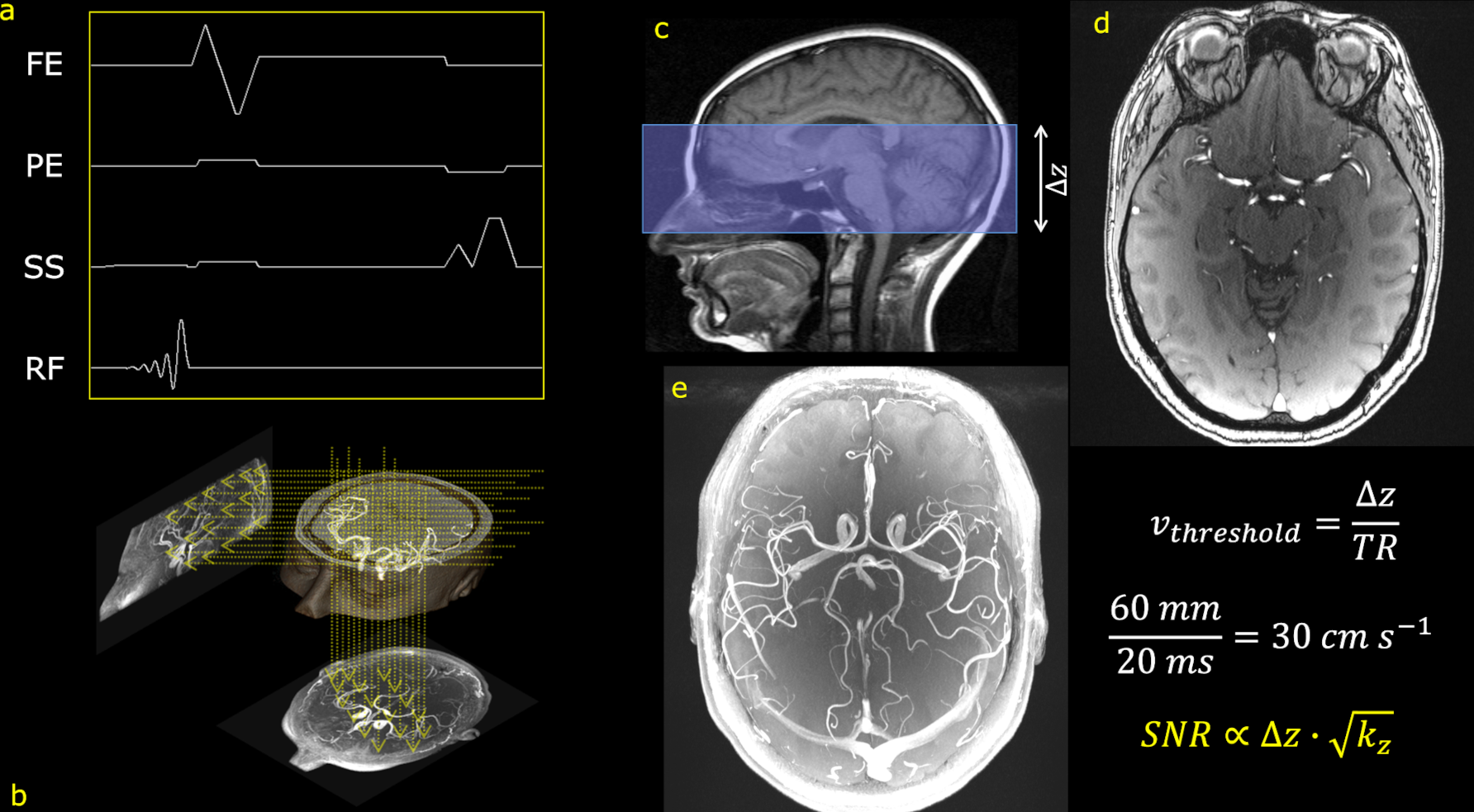
Figure 5. Principles of 3D time-of-flight (TOF) MRA. a) a typical 3D TOF pulse sequence with a minimum phase excitation pulse. b) the principle of the maximum intensity projection (MIP) algorithm. c) a thick slab is excited and phase encoded in the slice slect direction resulting in thin slices with good SNR d) single axial slice from a 3D TOF acquisition. e) a top-down MIP of all the slices in the 3D volume.The threshold for maximal signal is high due to the thick slab excitation.
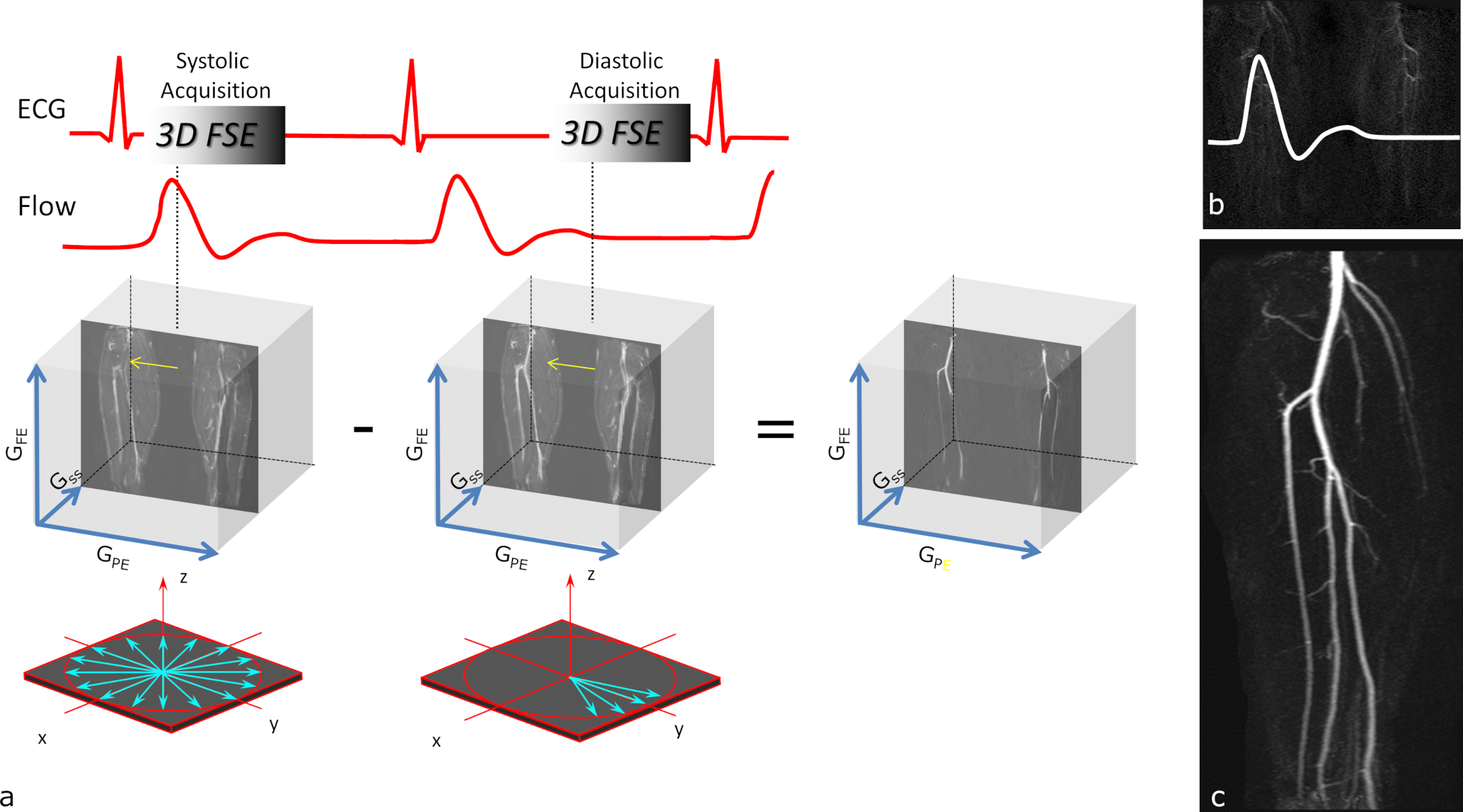
Figure 6. Principle of turbo/fast spin echo subtraction MRA. a) two segmented 3D acquisitions are performed; the first in systole and the second in diastole. In systole fast arterial flow results in signal dephasing and a reduction in signal. In diastole the arterial flow is relatively slow and therefore appears as a high signal. Since venous blood and stationary tissue are identical in both acquisitions magnitude subtraction of the images results in only signal from the arteries. b) the timing need to be optimised for each vessel territory. c) example MIP of the popliteal trifurcation.
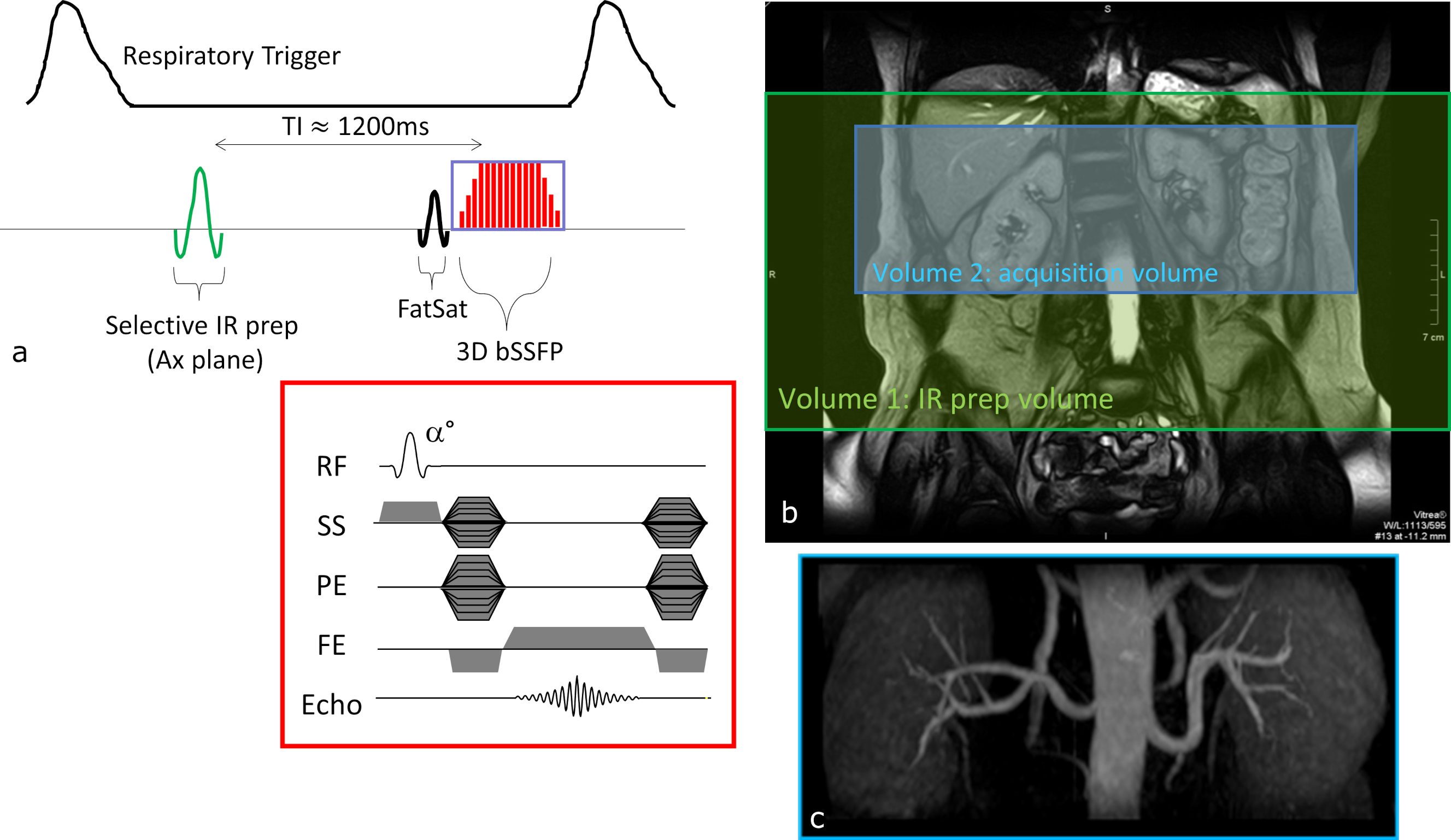
Figure 7. Principles of arterial spin labelling (ASL) MRA. a) a method for renal artery MRA in which a large FOV spatially selective
inversion preparation pulse is applied prior to a smaller FOV spatially selective 3D bSSFP
readout. The inversion time between tag and the readout is chosen such that the
background signal, including the inferior vena cava, is suppressed and there is
time for inflow of arterial spins into the imaging volume b) the 3D acquisition volume is offset from the larger inversion volume. c) example renal artery angiogram.