5420
DWI of liver using combination of sub-sampling and dual shots without dedicated multi-channel abdomen coil- A CT like patient positioning
Sajith Rajamani1, Ashok Kumar Reddy1, Nitin Jain1, Rajdeep Das1, Rajagopalan Sundaresan1, Jeremy Heinlein2, Harsh Kumar Agarwal1, Arnaud Guidon2, Sudhir Ramanna1, and Ramesh Venkatesan1
1GE Healthcare, Bangalore, India, 2GE Healthcare, Milwauke, WI, United States
1GE Healthcare, Bangalore, India, 2GE Healthcare, Milwauke, WI, United States
Synopsis
DWI is an important sequence for the diagnosis of liver lesions and to monitor the treatment response in patients undergoing therapies for hepatic malignancies [1]. But it is difficult to place the anterior abdomen coil for obese patients in non-wide bore MRI systems because of a potential chance of pinching the coil between patient and the bore. This is a limiting factor for the adoption of liver DWI MRI in clinical practice [2]. As a solution, we are proposing Dual Shots DWI with under-sampling across shots using volume coil located inside the magnet.
Purpose
Acquisition of abdomen mri protocol including DWI in a non-wide bore scanner using volume coil located inside the magnet bore without blurring and distortion in obese patients for whom positioning of dedicated anterior array abdomen coil is not possible because of very less space between the patient’s abdomen region and bore.Introduction
Diffusion weighted imaging is an increasingly used and proven technique in diagnosis and characterization of liver lesions [3]. Current clinical DWI protocol utilizes single shot spin-echo based echo planar imaging with ASSET (GE)/ GRAPPA (Siemens)/ SENSE (Philips) or multi shot DWI with sensitivity-encoding using dedicated multichannel receiver coil positioned over the anterior aspect of the patient to reduce blurring and distortion [4,5].According to WHO, it is estimated that more than 1 billion people worldwide are obese. In a non-wide bore MRI scanner, it is difficult to position an obese patient with a dedicated multichannel anterior array coil. Such patients are referred to centers having a wide bore MRI. In this abstract, we propose the use of single channel volume coil located inside the magnet bore instead of dedicated multi-channel abdomen anterior array coil. Major challenge in using single channel volume coil is the incompatibility of conventional parallel imaging methods because, it needs sensitivity information from individual coil elements of a multi-channel receiver coil to correct the phase information and estimation of missing k-space lines [6]. DWI is susceptible to distortion and blurring if parallel imaging under sampling is not used [7]. whereas other sequences don’t result in these artifacts with full K-Space sampling (Figure1). To mitigate these artifacts, we have proposed Dual Shot DWI with peripheral sub-sampling of k-space across shots to reduce the echo-spacing between the phase encoding lines.
Materials & Methods
A healthy volunteer scan was performed after obtaining informed consent approved by IRB on a 60cm bore 1.5T GE Signa HDXT scanner. An abdomen protocol was scanned using volume coil. Sequences used were, Axial T2 weighted image with fat sat, axial 2D Fiesta, 3D LAVA, single shot DWI and Dual shot DWI with sub-sampling across shots. The Dual Shot DWI Parameters are b values b0, b50 and b-500, field of View: 36cm TR/TE: 2000ms/59ms, No. of shots:2 breath hold duration: 18 seconds. Number of averages 1 for b0 and 2 for b0 and b500. ADC processing was done on an AW workstation using Ready view application.Data sampling and reconstruction of Dual shot DWI: the central portion of k-space is fully sampled which we call as ‘Cal data’. Peripheral part is sub-sampled across both shots to decrease the echo spacing between phase encoding lines to reduce blurring due to T2* decay. The Cal data from each shot is used to correct for the phase difference across the shots which are sub sampled (Figure2). Reconstruction was done using customized MATLAB scripts.
Results
Figure 3 shows single shot DWI and dual shot DWI with b500 sub-sampled across shots and their ADC maps. Single shot DWI image shows reduced signal to noise ratio and blurring because of long read out and T2* decay whereas dual shot Dwi with sub sampling has improved signal to noise ratio and reduced blurring.Conclusion and Discussion
High quality DWI with ADC map is required for the diagnosis and characterization of liver lesions. To generate diffusion weighted images using spin echo EPI without blurring and distortion without the use of dedicated abdomen coil, Dual shot DWI with sub-sampling across shots were used. Initial results show reduction in blurring and improved signal to noise ratio. However, further studies are required to evaluate more. This technique can be used in obese patients where low resolution is suffice for the characterization of abnormality. But in case of smaller pathologies and whenever high-resolution diffusion weighted imaging is required, then should be referred to a wide bore scanner using dedicated multichannel abdomen coil.Acknowledgements
No acknowledgement found.References
- Shenoy-Bhangle, A., Baliyan, V., Kordbacheh, H., Guimaraes, A.R. and Kambadakone, A., 2017.Diffusion weighted magnetic resonance imaging ofliver: Principles, clinical applications, and recent updates. World journal of hepatology, 9(26), p.1081.
- Donato, H., Franca, M., Candelaria, I. and Caseiro-Alves, F., 2017. Liver MRI: from basic protocol to advanced techniques. European journal of radiology, 93, pp.30-39.
- Petra G Kele, Eric J van der Jagt. Diffusion weighted imaging in the liver. World journal of gastroenterology
- Brau, A.C., Beatty, P.J., Skare, S. and Bammer, R., 2008. Comparison of reconstruction accuracy and efficiency among autocalibrating data-drivenparallel imaging methods. Magnetic Resonance in Medicine: 59(2), pp.382-395
- Chen, N.K., Guidon, A., Chang, H.C. and Song, A.W., 2013. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage, 72, pp.41-47
- Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging 2012; 36:55-72.
- Jezzard P, Balaban RS. Correction for geometric distortion in echo planar images from B0 field variations. Magn Reson Med. 1995;34(1):65–73
Figures
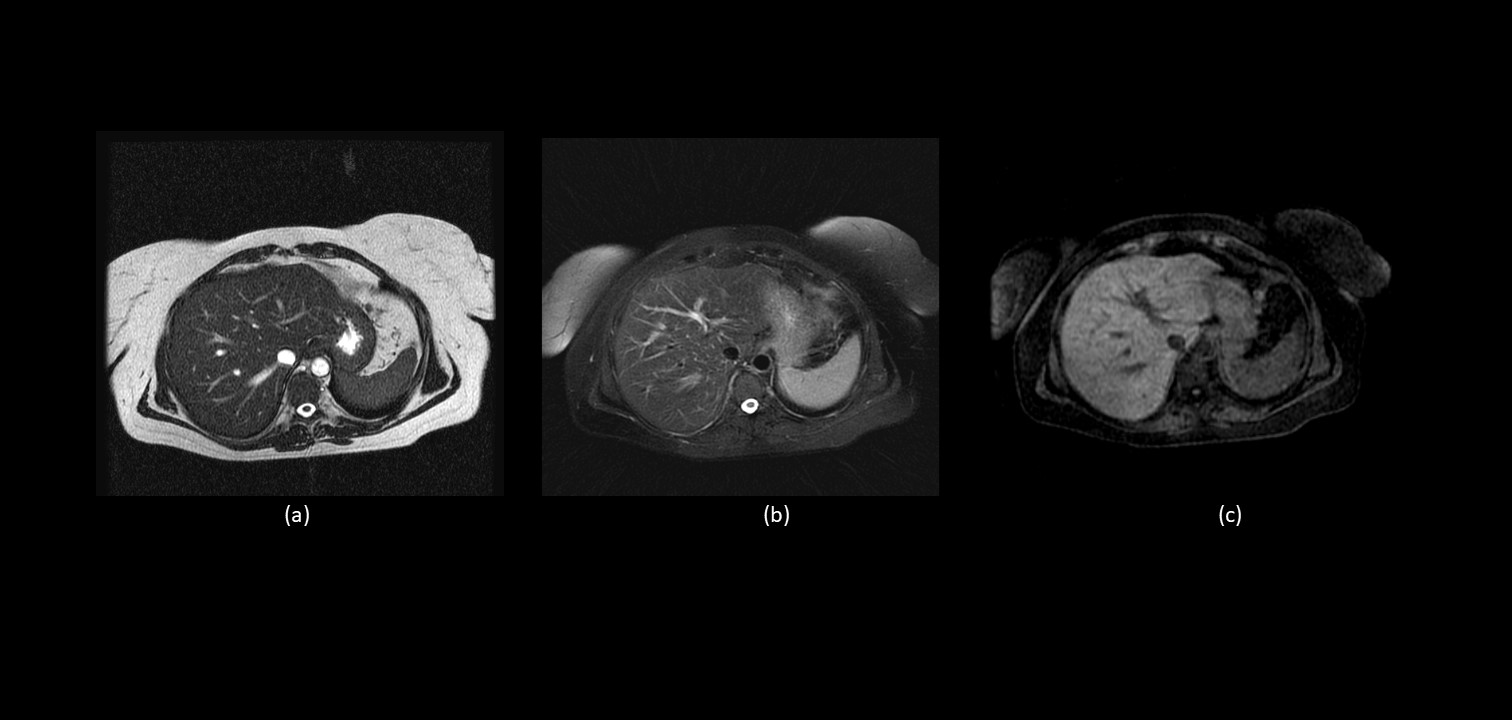
Abdomen
sequences acquired using volume coil without subsampling showing no artifacts.
(a) Axial 2D Fiesta, (b) Axial T2 FSE Fat Sat (c) Axial 3D LAVA
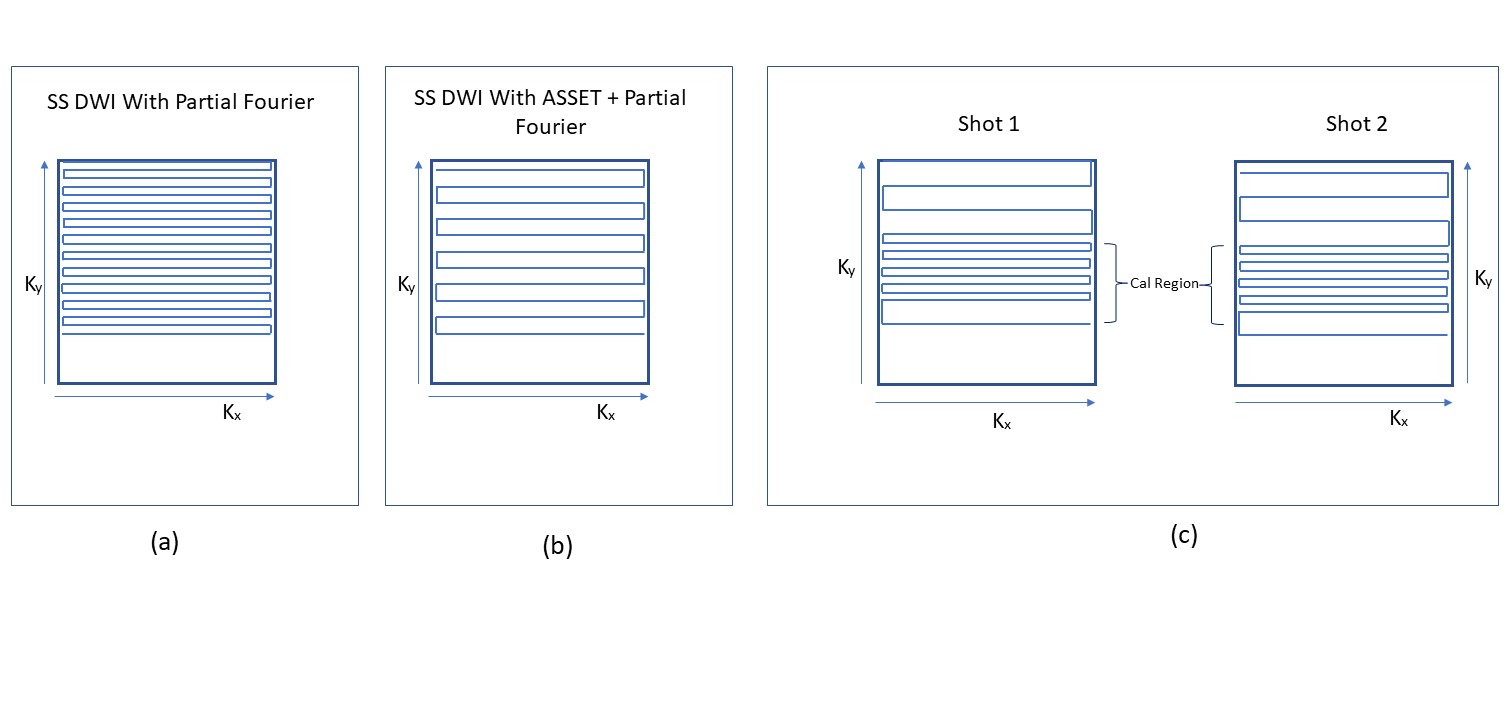
(a) showing the
Partial Fourier k-space filling pattern for single shot DWI using volume coil
with-out under-sampling or parallel imaging. (b) Single shot DWI with Partial
Fourier and ASSET using Multi channel coil. (c) Partial Fourier k-space of
Individual shots with central full sampling which is called Cal region and
peripheral subsampling.
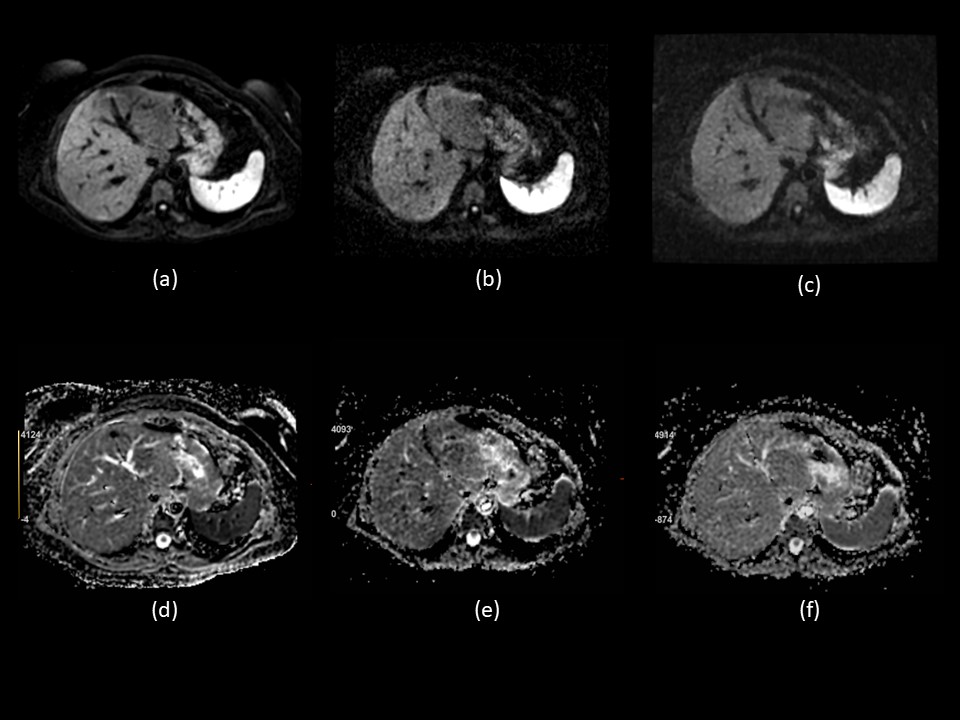
Abdomen Diffusion Weighted
Imaging with Breath Hold. (a) Single Shot DWI acquired using 12channel Anterior
Array Coil with ASSET Parallel Imaging Factor 2, (b) Single Shot DWI with Volume
Coil Partial Fourier image without ASSET showing poor SNR. (c) Dual-Shot DWI
with Partial Fourier and Sub-Sampling peripheral K-Space across shots showing
improved SNR. (d), (e) and (f) showing corresponding ADC Maps.
DOI: https://doi.org/10.58530/2023/5420