5416
Acoustic Noise Reduction in MRI and Utilizing Machine Learning1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
This study assesses the use of acoustic noise reduction (ANR) techniques as well as utilizing machine learning in conjunction with ANR, in order to preserve image quality and limit acquisition time. The standard sequences in a brain without contrast exam were tested to determine decibel (dBA) level, image quality, as well as the scanned volunteers' semiquantitative "loudness" scores.
Background
Magnetic resonance imaging is a critical diagnostic tool used to non-invasively evaluate a plethora of pathology in the outpatient and hospital setting. MRI scanners create an unavoidable acoustic noise that causes discomfort to a significant number of patients, sometimes requiring sedation to tolerate the exam. (1)Acoustic noise reduction techniques have improved patient comfort during MRI exams in previous studies. (2). Patients undergoing repeated MRI exams may even be at risk of hearing impairment, which acoustic noise reduction may mitigate. (3) In the present study, we investigated the acoustic noise produced from five different clinical MRI sequences comprising a standard brain protocol. The evaluation continues with the assessment of and compared to the same sequences with acoustic noise reduction technique. This technique is a GE imaging option provided for many different scanners and sequences. ANR is known to lead to a decrease in image quality, a potentially significant drawback to clinical implementation. (4) We hypothesized a machine learning image reconstruction (GE DL Recon) applied to the ANR sequence could preserve image quality in comparison to the standard MR sequences without ANR or DL Recon. Ultimately, we aimed to weigh the costs and benefits on using ANR after systematically investigating the effects on decibel level (dBA), acquisition time, overall image quality, and a semi quantitative loudness score from the scanned volunteers.
Methods
First, sound measurements were recorded in dBA, using a calibrated microphone, to establish averages for both the standard clinical sequence as well as their ANR counterpart. Sequences sampled include DWI, T2* GRE, T1 FLAIR, T2 FSE, and T2 FLAIR. This testing was done on a GE 3T Premier, and the ambient room was also recorded for reference.Next image quality was assessed. GE offers an acoustic noise reduction imaging option that can be applied to the tested MR sequences with two options, medium or high. For the DWI and GRE there is only an on/off option. Four iterations of each sequence were performed as follows: standard sequence, ANR sequence, DL sequence, and DL ANR sequence. Image quality was assessed on these sequences using a Likert scale. There were four aspects of image quality assessed, overall image quality, signal-to-noise, uniformity, and resolution. The Likert scale had five options to score each aspect of each sequence. “Same as standard (0),”” Marginally worse than the standard exam (-1),” and “Significantly worse than the standard exam (-2).” And the scores applied inversely, “Marginally better than the standard (+1),” and “Significantly better than the standard (+2).”
Four volunteers (N=4) were utilized to gather these images and assess image quality as well as garner a semiquantitative assessment of the “loudness” of each sequence. During the exams, the in vivo volunteers were asked to report a score of 0 to10 to reflect how loud the sequence was to them and their scores were recorded in whole numbers.
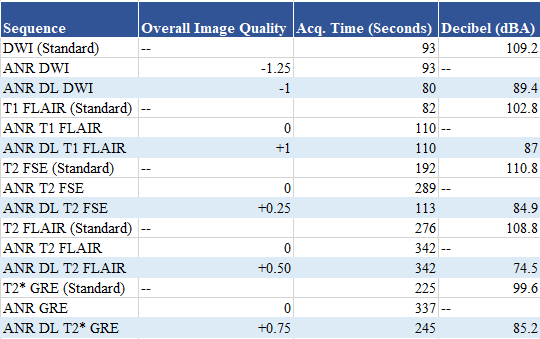
· The standard DWI decreased from 109.2 to 89 dBA,
· T1 FLAIR decreased from 102.8 to 86.9 dBA,
· T2 FSE decreased from 110.8 to 84.9 dBA,
· T2 FLAIR decreased from 108.8 to 74.5 dBA, and the
· T2* GRE decreased from 99.6 to 85.2 dBA.
The application of ANR increased acquisition time for all the sequences other than DWI. Please note that the T2 FSE allowed for acquisition time optimization by adjusting the echo train length from 16 to 18.
The sequences that utilized ANR as well as DL scored positively when compared to the standard, regarding image quality. The exception was the DWI sequence which averaged a score of marginally worse than the standard (-1). The rest of the DL ANR sequences performed, on average, between the same as the standard and marginally better with regards to the overall image quality.
Conclusions
ANR has benefits and disadvantages in the MRI practice. ANR decreases objectively measured decibel levels (dBA) and provides a subjectively quieter experience for the patient in the MR bore; however, it can also decrease image quality and increase acquisition time. Importantly, DL recon with optimized MR sequences can bridge the gap by preserving image quality with ANR and minimizing the difference in acquisition time compared to standard MR sequences.Acknowledgements
No acknowledgement found.References
1. Murphy KJ, Brunberg JA. Adult claustrophobia, anxiety and sedation in MRI. Magn Reason Imaging. 1997;15(1):51-4. doi: 10.1016/s0730-725x(96)00351-7. PMID: 9084025.
2. Alibek S, Vogel M, Sun W, et al. Acoustic noise reduction in MRI using Silent Scan: an initial experience. Diagn Interv Radiol. 2014;20(4):360-363. doi:10.5152/dir.2014.13458
3. Sartoretti E, Sartoretti T, Wyss M, van Smoorenburg L, Eichenberger B, van der Duim S, Cereghetti D, Binkert CA, Sartoretti-Schefer S, Najafi A. Impact of Acoustic Noise Reduction on Patient Experience in Routine Clinical Magnetic Resonance Imaging. Acad Radiol. 2020 Nov 3:S1076-6332(20)30599-7. doi: 10.1016/j.acra.2020.10.012. Epub ahead of print. PMID: 33158702.
4. McJury MJ. Acoustic Noise and Magnetic Resonance Imaging: A Narrative/Descriptive Review. J Magn Reson Imaging. 2022;55(2):337-346. doi:10.1002/jmri.27525
Figures
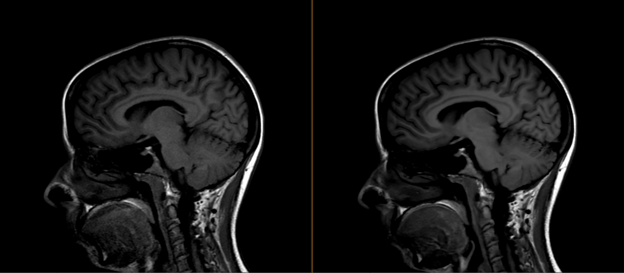
T1 FLAIR Standard (Left) and ANR T1 FLAIR with DL (Right)
The ANR T1 FLAIR with DL (Right), scored as “marginally better than standard” while reducing the decibel level by 15.8 dBA and adding 28 seconds in acquisition time. There was an average of 4 points reduced with the ANR T1 FLAIR with DL (Right) sequence for the volunteer “loudness” assessment survey.
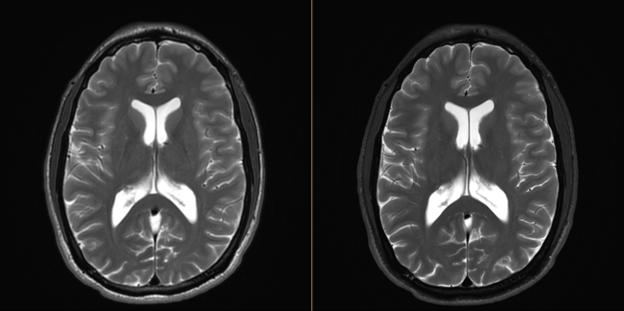
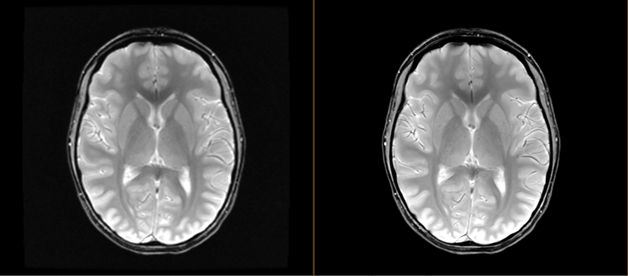
T2 FSE Standard (Left) vs ANR T2 FSE with DL (Right)
The ANR T2 FSE with DL, scored between “same as standard” and “marginally better than standard” while reducing the decibel level by 25.9 dBA and reducing acquisition time by 79 seconds. There was an average of 3 points reduced with the ANR T2 FSE with DL (Right) sequence for the volunteer “loudness” assessment survey.
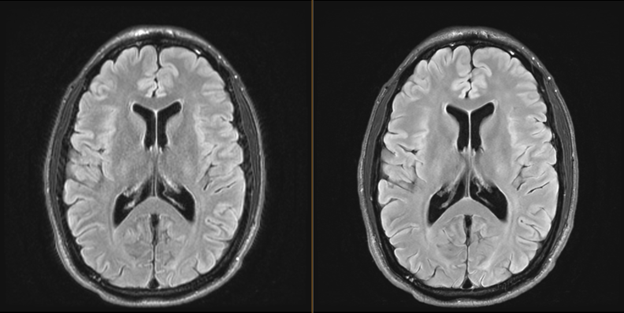
T2 FLAIR Standard (Left) vs ANR T2 FLAIR with DL (Right)
The ANR T2 FLAIR with DL, scored between “same as standard” and “marginally better than standard” while reducing the decibel level by 34.3 dBA and adding 66 seconds to the acquisition time. There was an average of 4 points reduced with the ANR T1 FLAIR with DL (Right) sequence for the volunteer “loudness” assessment survey.
T2* GRE Standard (Left) vs ANR T2* GRE with DL (Right)
The ANR T2* GRE with DL, scored between “same as standard” and “marginally better than standard” while reducing the decibel level by 14.4 dBA and adding 20 seconds in acquisition time. There was an average of 3.5 points reduced with the ANR T2* GRE with DL (Right) sequence for the volunteer “loudness” assessment survey.