5402
The Imaging Technique and Clinical Usefulness of Super Rapid Phase Contrast Angiography for Stroke Patients.1Graduate School of Health Sciences, Hokkaido University, Sapporo, Japan, 2Radiology, Otaru General Hospital, Otaru, Japan, 3Neurosurgery, Otaru General Hospital, Otaru, Japan, 4Faculty of Health Sciences, Hokkaido University, Sapporo, Japan
Synopsis
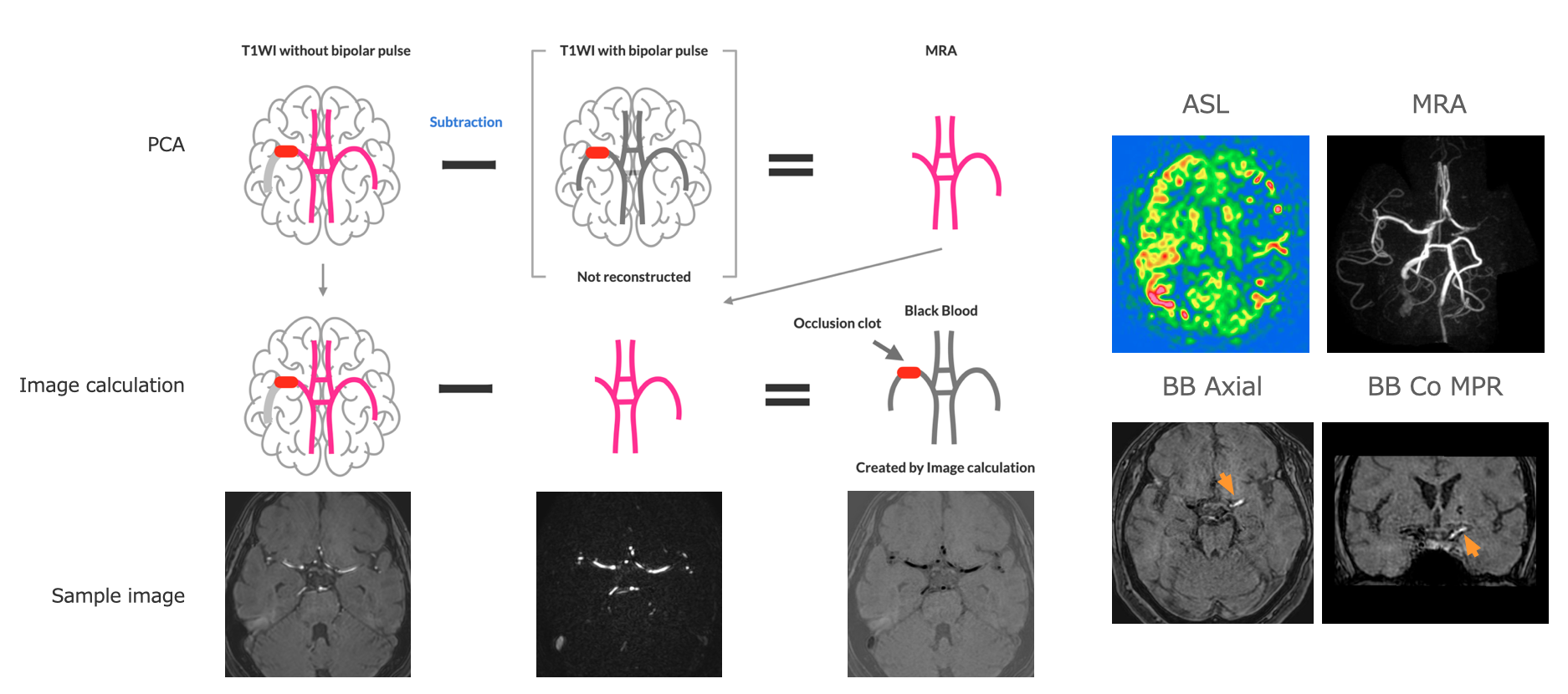
We offer super rapid phase contrast angiography (PCA) with a 60-second scan. This sequence greatly contributes to managing stroke patients compared with a conventional technique such as time-of-flight MRA. Parallel imaging and optimized voxel size reduce scan time as possible. Tilted optimized non-saturating excitation enhanced the depiction of the distal arteries in transverse acquisition PCA. Super rapid PCA overcomes motion artifacts due to short scan time and the shortest repetition time such as under 7 ms. Moreover, we obtain both MRA and black blood images as a subtraction image between the magnitude image and the MRA image.
In the neurosurgical emergency field, we often encounter poor-quality MRA due to motion artifacts or slow flow. Meanwhile, scan time should be shortened as possible in acute ischemic stroke (AIS) to obtain a better clinical outcome.1,2) Hence, we developed a super rapid phase contrast angiography (PCA) which can overcome motion artifacts and a 60-second scan of the cerebral artery. Additionally, we attempted several techniques based on this rapid PCA in clinical practice. 3,4) This sequence has contributed from various aspects for stroke patients.
[Purpose]
This study aimed to introduce the imaging technique and clinical usefulness of super rapid PCA for the neurosurgical emergency field.
[Method]
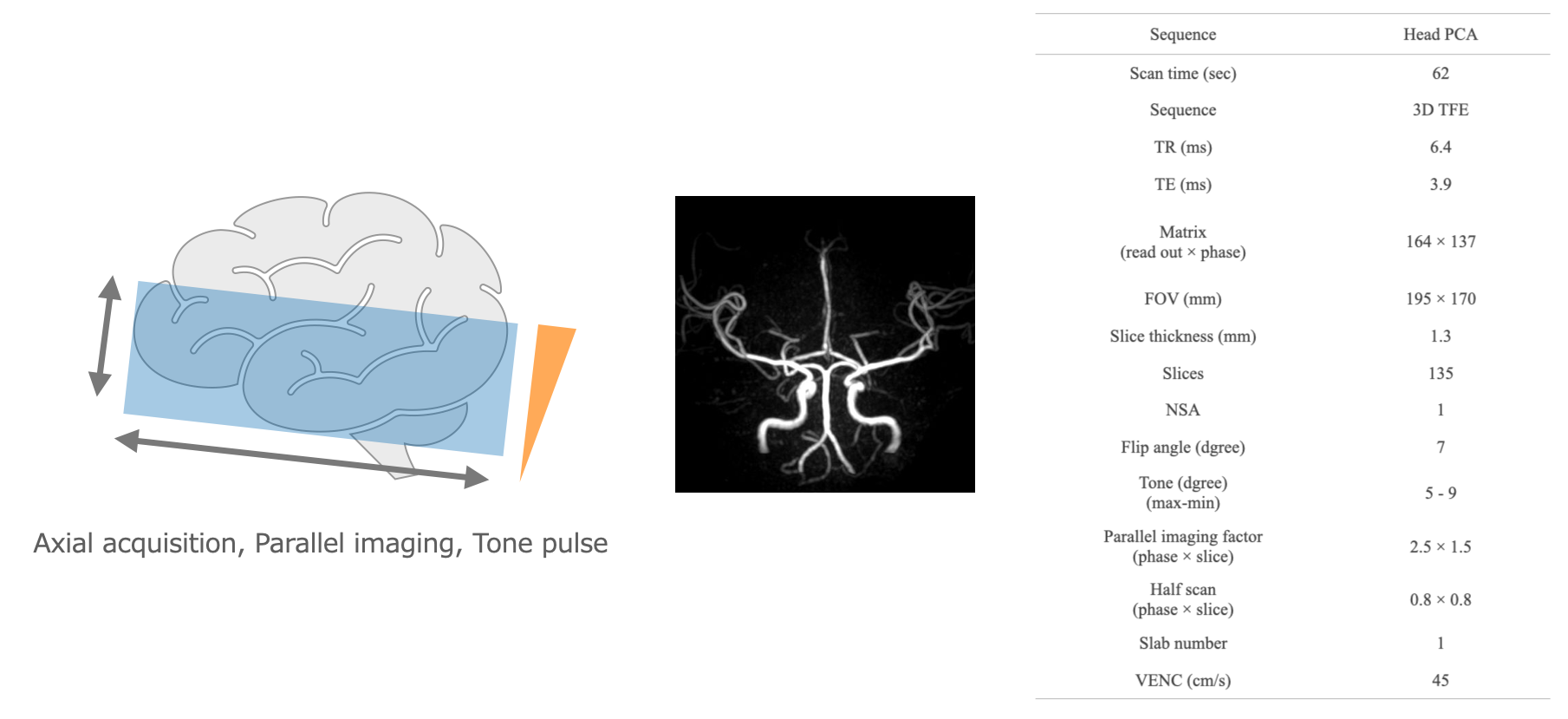
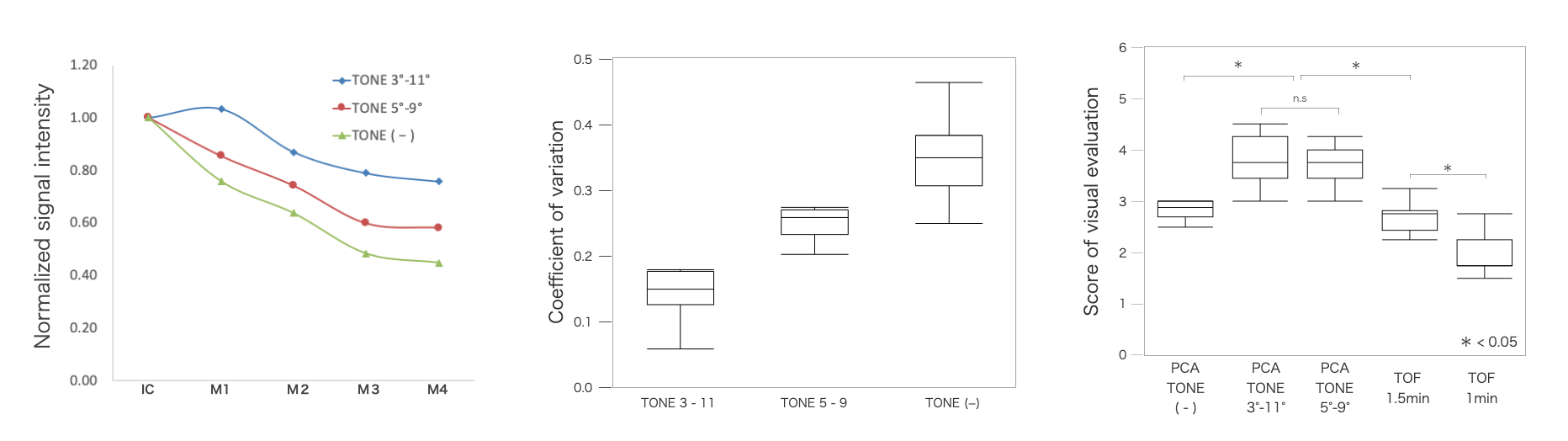
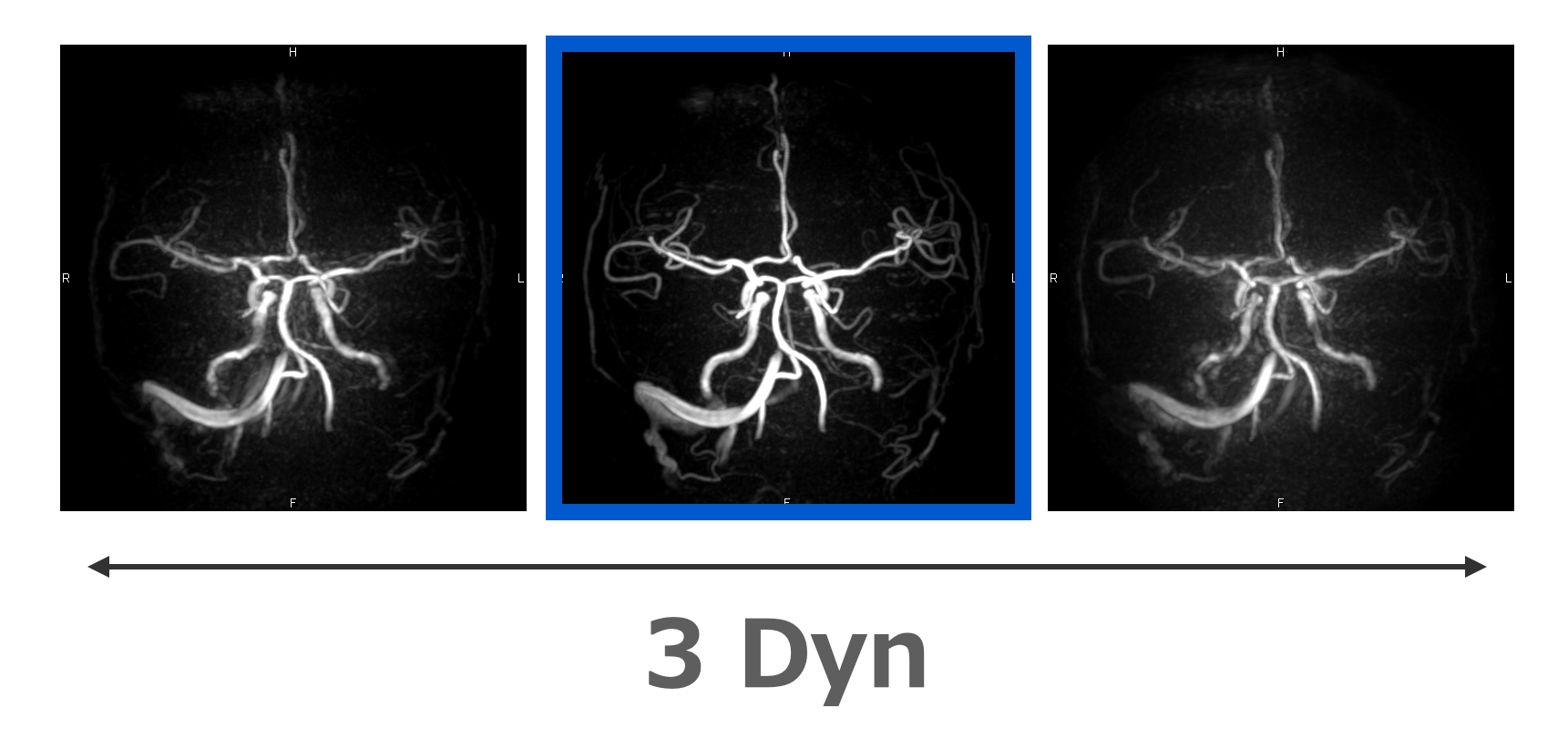
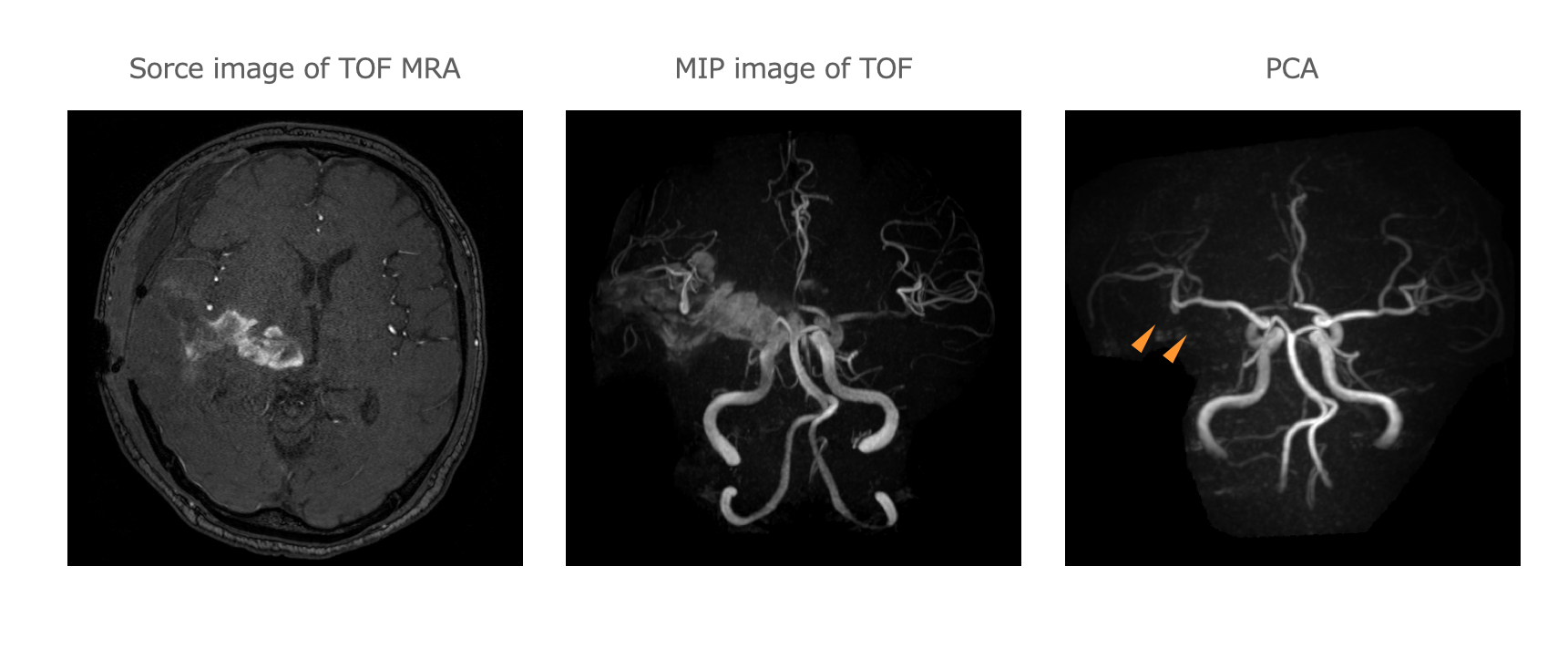
Super rapid PCA was constructed by combing a transverse acquisition, optimization of voxel size, shortest repetition time (TR), and parallel imaging. Tilted optimized non-saturating excitation (TONE) enhanced the depiction of the distal arteries. We investigated the optimal setting of TONE and image quality in the volunteer study. The coefficient of variation of signal intensity and signal behavior of cerebral vessels were evaluated. The visual evaluation also was performed by comparing conventional time-of-flight MRA images. As a clinical study, we obtain both MRA and black blood (BB) images in 36 AIS patients. BB images were demonstrated as a subtraction image between an MRA image and from magnitude image. We named this technique DEPICT (DEpicting blood clot and MRA using Phase contrast angiography with Image Calculation for Thrombectomy) We compared the reliability of the clot location using AC1 in BB image with susceptibility vessel sign (SVS) in T2*WI.5,6) We assessed the robustness of motion artifacts through visual evaluation. Additionally, we attempted a dynamic study consisting of over three times PCA with 45 seconds for strong motion patients with stroke. We used images without motion artifacts to assess cerebral arteries.
[Result]
The optimized TONE pulse of PCA with TR 6.5 ms was from 5 degrees on the proximal side to 9 degrees on the distal side. At extreme tone settings, signal overcorrection was observed. Super rapid PCA offers superior image quality compared with 1.5 min time-of-flight. BB image was obtained in all AIS patients. BB image has higher reliability of the clot location and higher robustness for motion artifact compared with T2*WI. We could obtain MRA images without motion artifacts using dynamic study in almost of patients. Moreover, PCA could provide MRA avoiding hematoma.
[Consideration]
Super rapid PCA provided diagnosable image quality. Especially, main arteries were depicted with superior quality and within a shorter scan time compared to a conventional TOF MRA. This is a large advantage for AIS management. The clot location providing a BB image contributes to the strategy of mechanical thrombectomy. Hence, DEPICT will work as a first-choice technique to assess acute ischemic stroke. Dynamic scan of super rapid PCA showed the potential to overcome strong motion artifacts of patients with stroke.
[Conclusion]
Super rapid PCA contributes to depicting cerebral arteries compared with a conventional technique in stroke patients.
Acknowledgements
NoneReferences
1) Li G, Wu G, Qin Z, Li H, Cheng X, Cai Y. Prognostic Value of Clot Burden Score in Acute Ischemic Stroke after Reperfusion Therapies: A Systematic Review and Meta-Analysis. J Stroke Cerebrovasc Dis 2019;28. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.07.009.
2) Riedel CH, Jensen U, Rohr A, Tietke M, Alfke K, Ulmer S, et al. Assessment of thrombus in acute middle cerebral artery occlusion using thin-slice nonenhanced Computed Tomography reconstructions. Stroke 2010;41:1659–64.
3) Oura D, Ihara R, Myo E, Sato S, Sugimori H. Construction of super-rapid brain MRA using oblique transverse acquisition phase contrast angiography with tilted optimized non-saturated excitation pulse. Magn Reson Imaging 2021;85:193–201.
4) Oura D, Gekka M, Morishima Y, Niiya Y, Ihara R, Ebina T, et al. Simultaneous depiction of clot and MRA using 1 min phase contrast angiography in acute ischemic patients. Magn Reson Imaging 2022. https://doi.org/10.1016/j.mri.2022.08.011.
5) Park M-G, Oh S-J, Baik SK, Jung DS, Park K-P. Susceptibility-Weighted Imaging for Detection of Thrombus in Acute Cardioembolic Stroke. J Stroke Cerebrovasc Dis 2016;18:73–9.
6) Naggara O, Raymond J, Domingo Ayllon M, Al-Shareef F, Touzé E, Chenoufi M, et al. T2* “susceptibility vessel sign” demonstrates clot location and length in acute ischemic stroke. PLoS One 2013;8:e76727.
Figures