5391
Clinical Impact of Single Breath Hold Contrast Enhanced 4D-MRA with High Temporal and Spatial Resolution without k-space Data Sharing Techniques1Dept. of Radiological technology, Kokura memorial hospital, Kitakyushu, Japan
Synopsis
For evaluation of arteriovenous malformations, contrast-enhanced 4D-MRA is useful to detect feeding arteries and draining veins. However, with the Keyhole technique, contamination of different phases is a major problem. We solved this problem by applying parallel imaging with compressed sensing to contrast-enhanced 4D-MRA(CS-4D-MRA). CS-4D-MRA was able to acquire images without contamination of the arterial phase with echo signals from the venous phase. It also had high temporal and spatial resolution, and was able to clearly visualize the feeder and the drainer.
Background
Arteriovenous malformations are evaluated by contrast-enhanced CTA, contrast-enhanced MRA, and transcatheter angiography. Remarkably, contrast-enhanced 4D-MRA can evaluate the 3D structure of blood vessels and flow over time1). For contrast-enhanced 4D-MRA imaging, it is common to image using Keyhole and/or view-sharing techniques2). The keyhole technique collects only the central portion of the k-space, which determines the contrast in each phase. In addition, high-frequency components are collected at different time phases, and the echo signals are shared to achieve high temporal resolution. However, this technique has the problem of contamination of venous phase data into the reconstructed early arterial phase image, because it uses k-space data from different phases3). This may affect the evaluation of the assessment of vascular geometry when imaging arteriovenous malformations, such as the appearance of veins in the early arterial phase. Our method solves this problem by using parallel imaging with compressed sensing to provide contrast-enhanced 4D-MRA with high temporal and spatial resolution. We evaluated its benefit from clinical images.Materials and methods
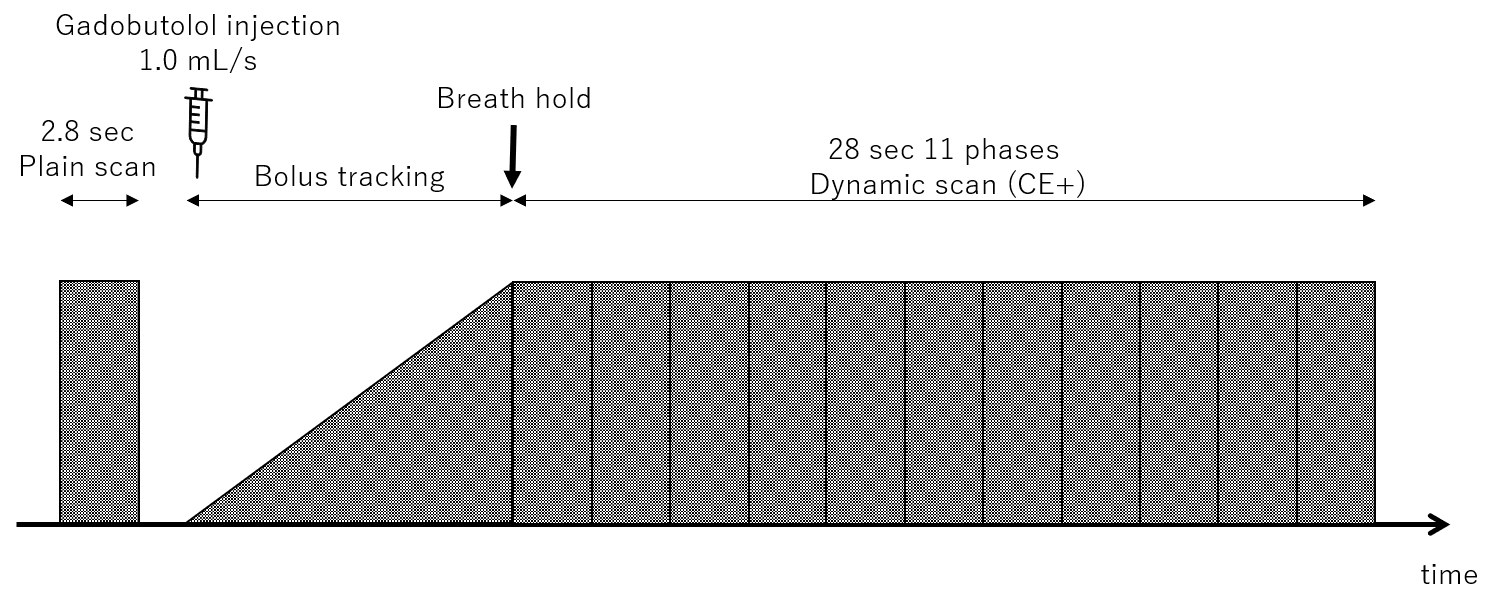
PHILIPS Ingenia 1.5T was used as MR scanner. Gadobutolol 1.0 mol/L was used for the studies, and 0.1 mmol/kg was injected at the recommended injection rate of 1.0 mL/s by an injector. Our MR imaging sequence has a temporal resolution of 2.8 sec (acquisition time of 1 phase) and a spatial resolution of 0.7*0.7*2.0 mm. The MR imaging sequence acquired of a plain phase imaging before contrast enhancement, followed by 11 phases (31 sec) with breath hold after contrast enhancement and monitoring the arrival of the contrast agent (Fig. 1). The imaging sequence used a gradient echo method to collect 3DT1-weighted images with a Compress SENSE factor of 7. The resulting image was presented as plain images subtracted from the contrast-enhanced images. Instead of using keyhole technique and view sharing, which are generally used in MR-DSA, parallel imaging technique with compressed sensing was used to provide high temporal and high spatial resolution imaging.Teaching point
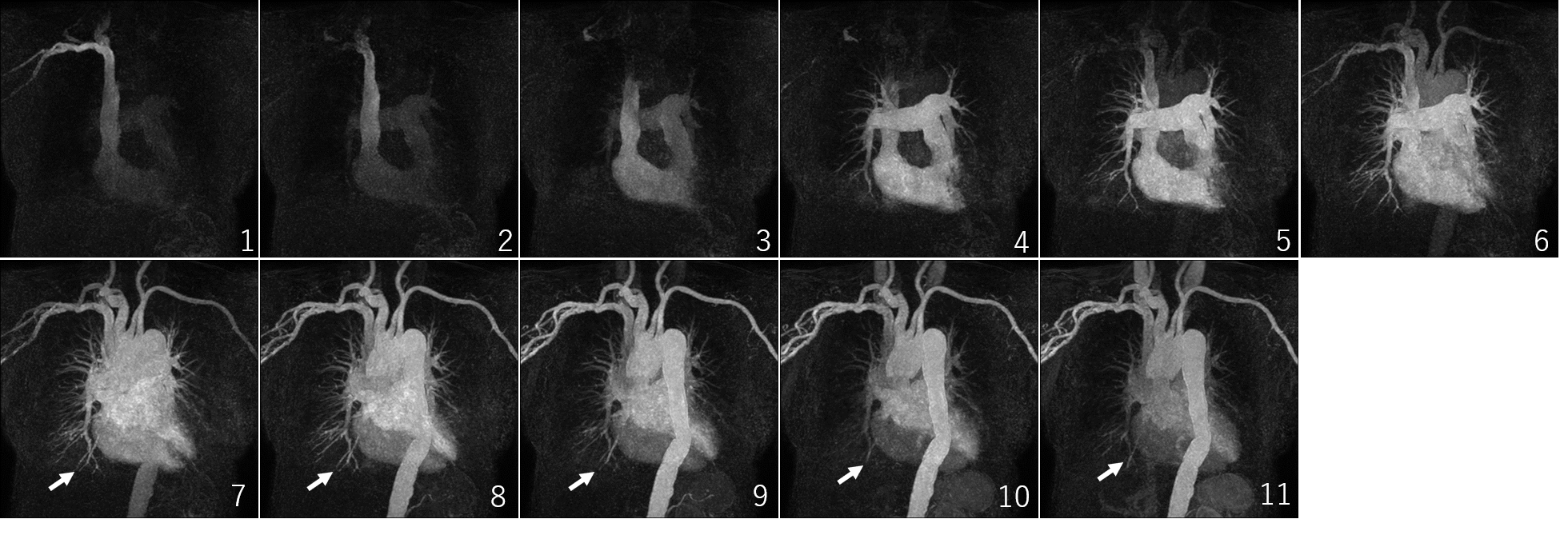
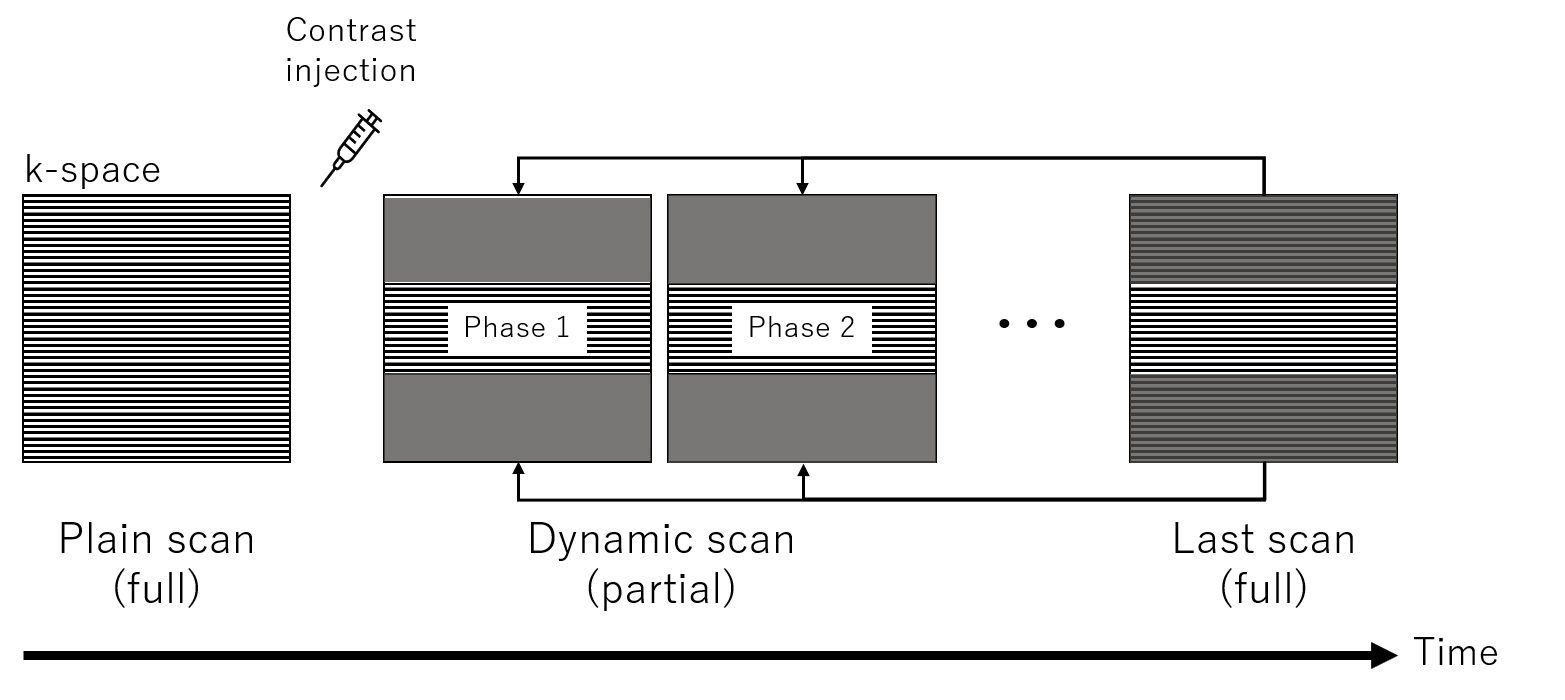
Contrast-enhanced 4D-MRA with high temporal and spatial resolution by using parallel imaging with compressed sensing was able to acquire images of the appropriate timing phase of contrast without venous phase contamination in the evaluation of shunt diseases such as pulmonary arteriovenous fistulas. An example of an image acquired is shown in Figure 2. The acquired images clearly visualized even the details of the blood vessels by using subtraction processing. The results enabled the detection of feeder and drainer blood vessels. In addition, keyhole and view sharing were not used in our study. The Keyhole technique, as shown in Figure 3, fully samples data only in the first or last phase. For any other phases, only the low-frequency component of the k-space is acquired, and the high-frequency component is used instead of the full-sampled phase. Therefore, using the post contrast phase with high SNR leads to contamination of vein information. In addition, motion artifacts in the reference scan affect the overall phase. In this study, 4D-MRA could be collected without any loss of temporal or spatial resolution. This is a benefit of the parallel imaging with compressed sensing for higher speed and noise reduction process.Conclusion
Our 4D-MRA with high temporal and spatial resolution has improved the evaluation of clinical conditions in shunt disease, fistula and arteriovenous malformations. Therefore, no contamination of other phases in the early arterial phase was detected. In addition, keyhole and view sharing were not used in our study. Therefore, the inclusion of in the early arterial phase, i.e., vein images, was not detected.Acknowledgements
No acknowledgement found.References
1. Illies T, Forkert ND, Ries T, et al. Classification of cerebral arteriovenous malformations and intranidal flow patterns by color-encoded 4D-hybrid-MRA. Am J of Neuroradiol, 2013, 34(1): 46-53.
2. Hadizadeh DR, Kukuk GM, Steck DT, et al. Noninvasive evaluation of cerebral arteriovenous malformations by 4D-MRA for preoperative planning and postoperative follow-up in 56 patients: comparison with DSA and intraoperative findings. Am J of neuroradiol, 2012, 33(6): 1095-1101.
3. Van Vaals JJ, Brummer ME, Thomas DW, et al. “Keyhole” method for accelerating imaging of contrast agent uptake. J of Magnetic Resonance Imaging, 1993, 3(4): 671-675.
Figures