5356
Comprehensive evaluation of carotid body tumor complicated with carotid plaque by high resolution vascular wall imaging in plateau area1Affiliated Hospital of Qinghai University, Xining, China
Synopsis
Keywords: Vessels, Tumor
This study investigated risk factors for Carotid body tumor(CBT) in plateau areas, compared the incidence of CBT at high altitude group and low altitude group, and investigated the relationship between CBT and ipsilateral carotid plaque.The results showed that the incidence of CBT was higher at high altitude group than at low altitude group, and CBT will increase the incidence of ipsilateral carotid plaque.high resolution magnetic resonance vascular wall imaging(HR-VWI) has more advantages in the diagnosis of carotid body tumor than conventional MR Imaging.Introduction/Purpose
Carotid body tumor (CBT) is more common in plateau area than in plain area in long-term chronic hypoxia environment [1,2,3].Surgical treatment of CBT with carotid plaque is risky.In recent years, MR Imaging has played an increasingly important role in preoperative examination of CBT [4,5], but it cannot accurately identify plaques and evaluate their properties.This study is based on high resolution magnetic resonance vascular wall imaging(HR-VWI) comprehensive evaluation of CBT and carotid plaques. The purpose of this study was to: (1) To explore the diagnostic advantages of HR-VWI over conventional MR Imaging for CBT;(2) The incidence of carotid body tumor in high and low altitude groups was compared and the risk factors of CBT in plateau areas were analyzed;(3) To investigate the effect of CBT on ipsilateral carotid plaque.Method
The patients who underwent 3T MR-scanner (MAGNETOM PRISMA,Siemens Healthcare,Erlangen,Germany)high resolution magnetic resonance vascular wall imaging(HR-VWI) examination in the Affiliated Hospital of Qinghai University from April 2015 to February 2022 and lived in Qinghai region for more than 10 years were retrospectively analyze.The sequence and parameters of scan are:(1)T1-spcae:TR/TE=750ms/13ms;FOV=230mm×230mm;scan matrix=328×328;voxel size=0.4mm×0.4mm×0.6mm;slice thickness=0.6mm;acquisition time=7 min 43 sec;(2)T2-spcae:TR/TE=2500ms/353ms;FOV=230×230mm;scan matrix=328×328;voxel size=0.4mm×0.4mm×0.7mm;slice thickness=0.7mm;acquisition time=6 min 2 sec;(3)3D-TOF:TR/TE=21ms/3.43ms;FOV=140mm×140mm;scan matrix=256×256;voxel size=0.3mm×0.3mm×0.7mm;slice thickness=0.65mm;acquisition time=4min 8 sec.The patients were divided into Carotid body tumor(CBT) group and no CBT group. The general data of the two groups were compared,including age, gender, altitude of residence, hemoglobin(HGB), hematocrit(HCT),red blood cell(RBC),meancorpuscular volume(MCV),mean corpuscular hemoglobin(MCH),mean corpuscular hemoglobin concentration(MCHC),red blood cell distribution width-coefficient of variation (RDW-CV),red blood cell volume distribution width- Standard deviation (RDW-SD). Univariate analysis and multivariate LOGISTIC regression were used to analyze the independent risk factors of CBT.A total of 251 patients were divided into high altitude group (≥2500m) and low altitude group (< 2500m) according to the altitude of their residence. The incidence of CBT was compared between high altitude group and low altitude group.Classification was made according to the degree of wrapping of the surrounding blood vessels by CBT, and the relationship between different types of CBT and altitude was analyzed.If carotid body tumor is combined with ipsilateral carotid plaque, the relationship between CBT and ipsilateral carotid plaque was studied.
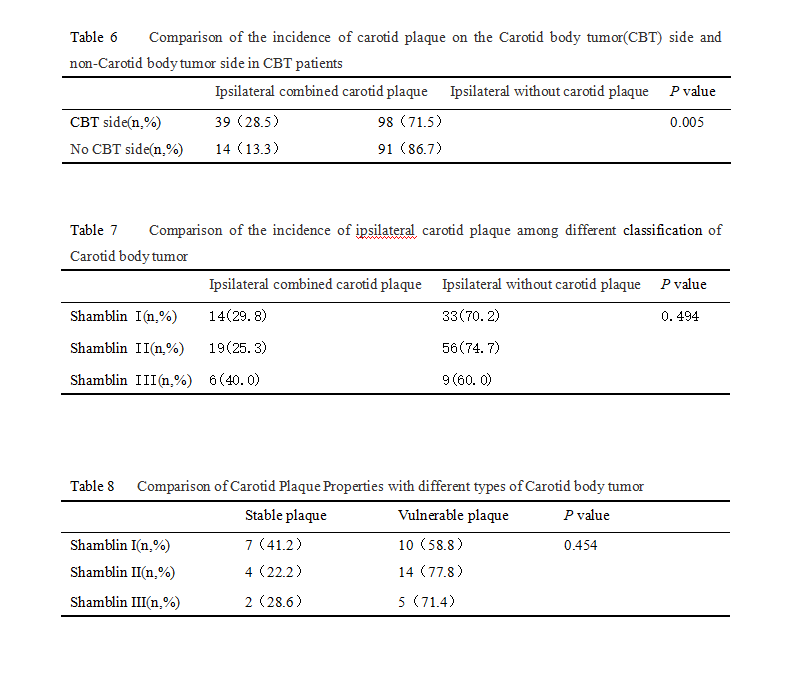
Independent samples T-test was used for normal distribution data between CBT group and no CBT group.The factors with significant difference (P<0.05) were selected as independent variables by univariate analysis, and the independent risk factors of CBT were analyzed by multivariate LOGISTIC regression.Pearson Chi-square test was used to compare the incidence of CBT between the high and low altitude groups.The altitude of different CBT classification was compared by one-way ANOVA.Pearson Chi-square test was used to Compare the incidence of carotid plaque on the CBT side and no CBT side in CBT patients .Pearson Chi-square test was used to compare the incidence of ipsilateral carotid plaque among different classification of Carotid body tumor.Comparison of Carotid Plaque Properties with different types of Carotid body tumor using Fisher's exact probability method.
Result
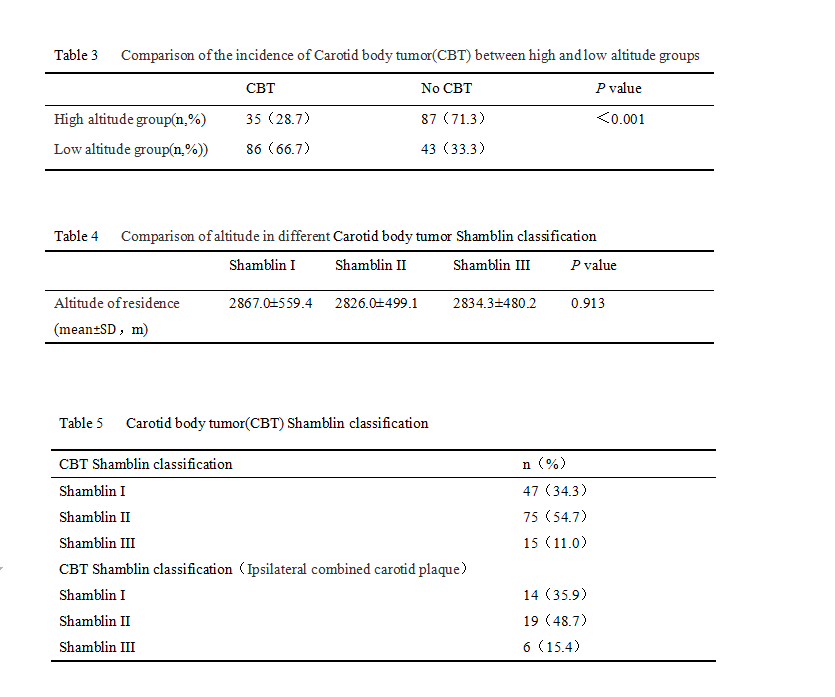
A total of 251 patients were included, ranging in age from 23 to 93 years old, with an average age of 56.8±12.0 years old, with an altitude of 1770 to 4700m, and an average altitude of 2661.8±537.6m. There were 121 patients in the Carotid body tumor(CBT)group and 130 patients in no CBT group.There were 105 cases of unilateral CBT and 16 cases of bilateral CBT,A total of 137 cases were detected.There were 47 cases of Shamblin I, 75 cases of Shamblin II, and 15 cases of Shamblin III.A total of 39 cases of CBT ipsilateral combined with carotid plaque, 42 cases of carotid plaque were detected, of which 29 cases (69.0%) were vulnerable and 13 cases (31.0%) were stable.Univariate analysis and multivariate LOGISTIC regression analysis showed that Age(OR=0.952;95% CI = 0.925 0.979;P=0.001), Gender(OR=7.149;95% CI = 3.547 14.408;P < 0.001), Altitude of residence (OR=1.001;95% CI = 1.000 1.001;P=0.013),mean corpuscular hemoglobin concentration(MCHC)(OR=0.946; 95% CI = 0.914 0.979;P=0.002) was an independent risk factor for CBT.CBT increased the incidence of ipsilateral carotid plaque (P=0.005).There were 122 patients in the high altitude group and 129 in the low altitude group. The incidence of CBT in the high altitude group was higher than that in the low altitude group (P < 0.01).Discussion/Conclusion
The incidence of Carotid body tumor(CBT) in the high altitude group was higher than that in the low altitude group. CBT will increase the incidence of ipsilateral carotid plaque;High-resolution magnetic resonance vascular wall imaging can accurately display CBT and carotid plaque.Acknowledgements
No acknowledgement found.References
[1] Shahi S, Upadhyay AR, Devkota A, Pantha T, Gautam D, Paudel DR. Excision of rare carotid body tumour without preembolisation: Case report and literature review. Int J Surg Case Rep. 2018;53:99-101. DOI: 10.1016/j.ijscr.2018.10.029. Epub 2018 Oct 25.
[2] Hinojosa CA, Anaya-Ayala JE, Laparra-Escareno H, Torres-Machorro A, Lizola R, Gamboa-Domínguez A. Concomitant Surgical Treatment of Symptomatic Carotid Artery Disease With a Coexisting Shamblin I Carotid Body Tumor. Vasc Endovascular Surg. 2017 Feb;51(2):103-107. DOI: 10.1177/1538574416689430. Epub 2017 Jan 24.
[3] Rodríguez-Cuevas S, López-Garza J, Labastida-Almendaro S. Carotid body tumors in inhabitants of altitudes higher than 2000 meters above sea level. Head Neck. 1998 Aug;20(5):374-8. DOI: 10.1002/(sici)1097-0347(199808)20:5<374::aid-hed3>3.0.co;2-v.
[4] Arya S, Rao V, Juvekar S, Dcruz AK. Carotid body tumors: objective criteria to predict the Shamblin group on MR imaging. AJNR Am J Neuroradiol. 2008 Aug;29(7):1349-54. DOI: 10.3174/ajnr.A1092. Epub 2008 Apr 16.
[5] Berger G, Łukasiewicz A, Grinevych V, Tarasów E. Carotid Body Tumor - radiological imaging and genetic assessment. Pol Przegl Chir. 2020 Nov 6;92(6):39-44. DOI: 10.5604/01.3001.0014.4872.
Figures
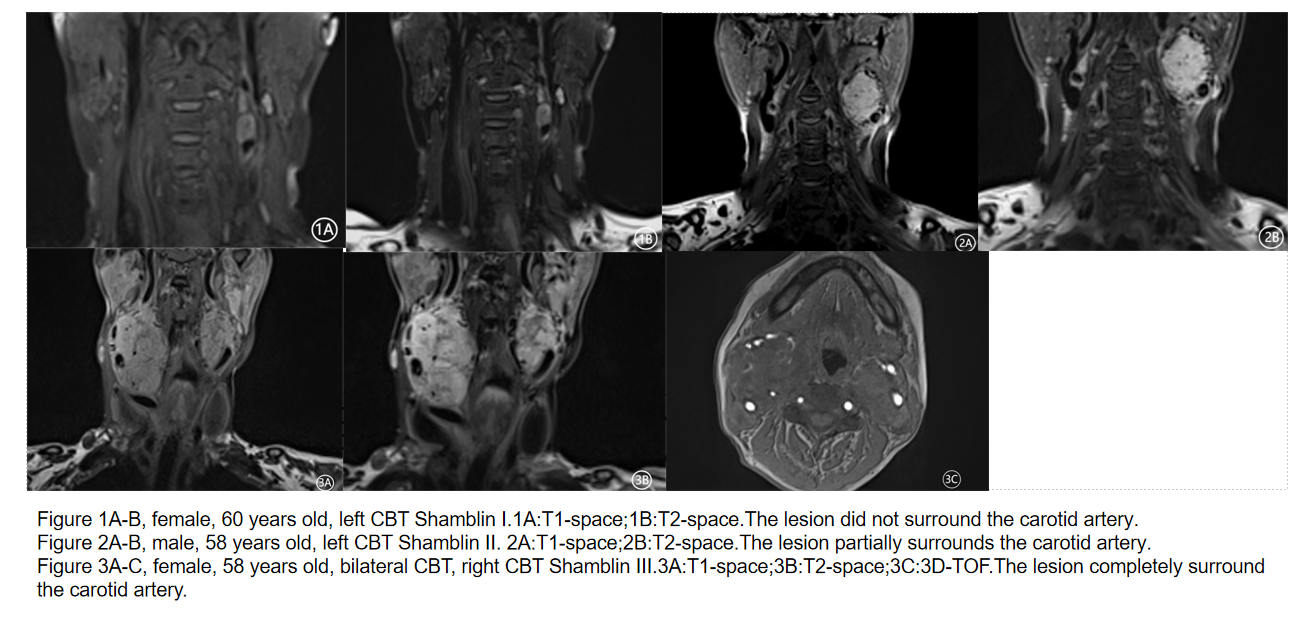
Figure 1A-B, female, 60 years old, left CBT Shamblin I.1A:T1-space;1B:T2-space.The lesion did not surround the carotid artery.
Figure 2A-B, male, 58 years old, left CBT Shamblin II. 2A:T1-space;2B:T2-space.The lesion partially surrounds the carotid artery.
Figure 3A-C, female, 58 years old, bilateral CBT, right CBT Shamblin III.3A:T1-space;3B:T2-space;3C:3D-TOF.The lesion completely surround the carotid artery.
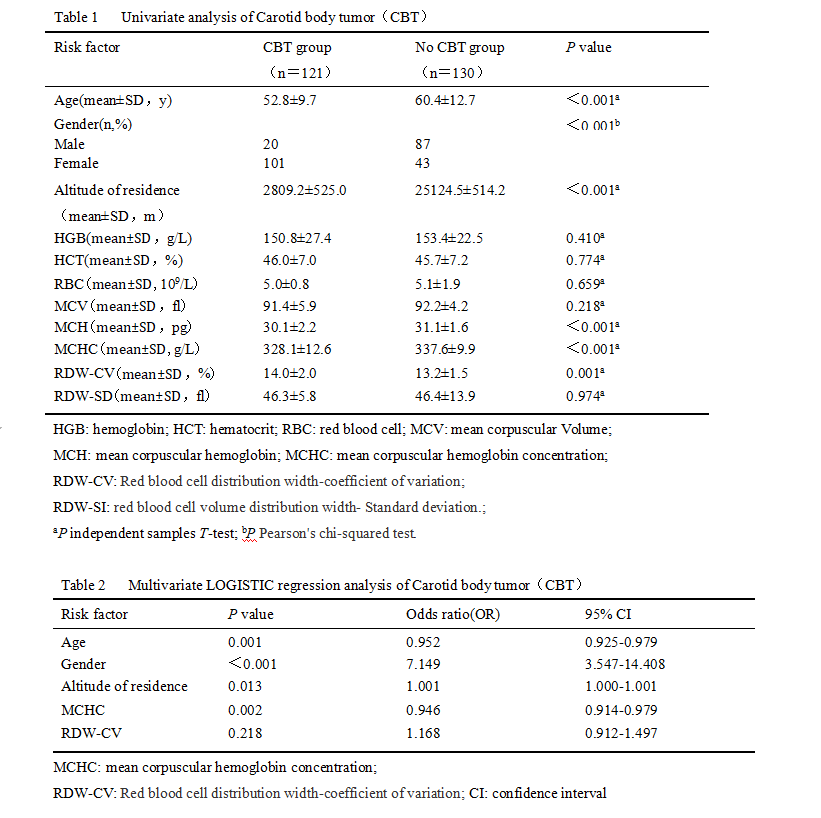
HGB: hemoglobin; HCT: hematocrit; RBC: red blood cell;
MCV: mean corpuscular Volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration;
RDW-CV: Red blood cell distribution width-coefficient of variation;
RDW-SI: red blood cell volume distribution width- Standard deviation;
aP independent samples T-test; bP Pearson's chi-squared test.