5342
Exploring the Frontal Aslant Tract in Tourette syndrome: a connectivity study1Neuroradiology Department, Fondazione IRCCS (Istituto di Ricovero e Cura a Carattere Scientifico) Istituto Neurologico Carlo Besta, Milan, Italy, 2Department of Health Sciences, Università degli Studi di Milano, Milan, Italy, 3Neurosurgery Department, Fondazione IRCCS (Istituto di Ricovero e Cura a Carattere Scientifico) Istituto Neurologico Carlo Besta, Milan, Italy, 4Department of Neurological Surgery, University Medical Center Mainz, Mainz, Germany, 5Parkinson's Disease and Movement Disorders Unit, Department of Clinical Neurosciences, Fondazione IRCCS (Istituto di Ricovero e Cura a Carattere Scientifico) Istituto Neurologico Carlo Besta, Milan, Italy
Synopsis
Keywords: White Matter, Tractography & Fibre Modelling
This study investigates for the first time microstructural alteration of the Frontal Aslant Tract (FAT) in nine subjects with TS compared to twelve healthy subjects. FAT was reconstructed trough Spherical Deconvolution (SD) and parameters derived from Diffusion Tensor Imaging (DTI) and Neuritis Orientation Dispersion and Density Imaging (NODDI) were extracted. We observed a Fractional Anisotropy (FA) reduction, indicating a greater disorganization of fibers, and accordingly an increased Orientation Dispersion Index (ODI), which indicates more dispersed fibers. We also highlighted a negative correlation between motor tic severity (quantified by the YGTSS) and neurite density (ND) and free water fraction (FISO).Introduction
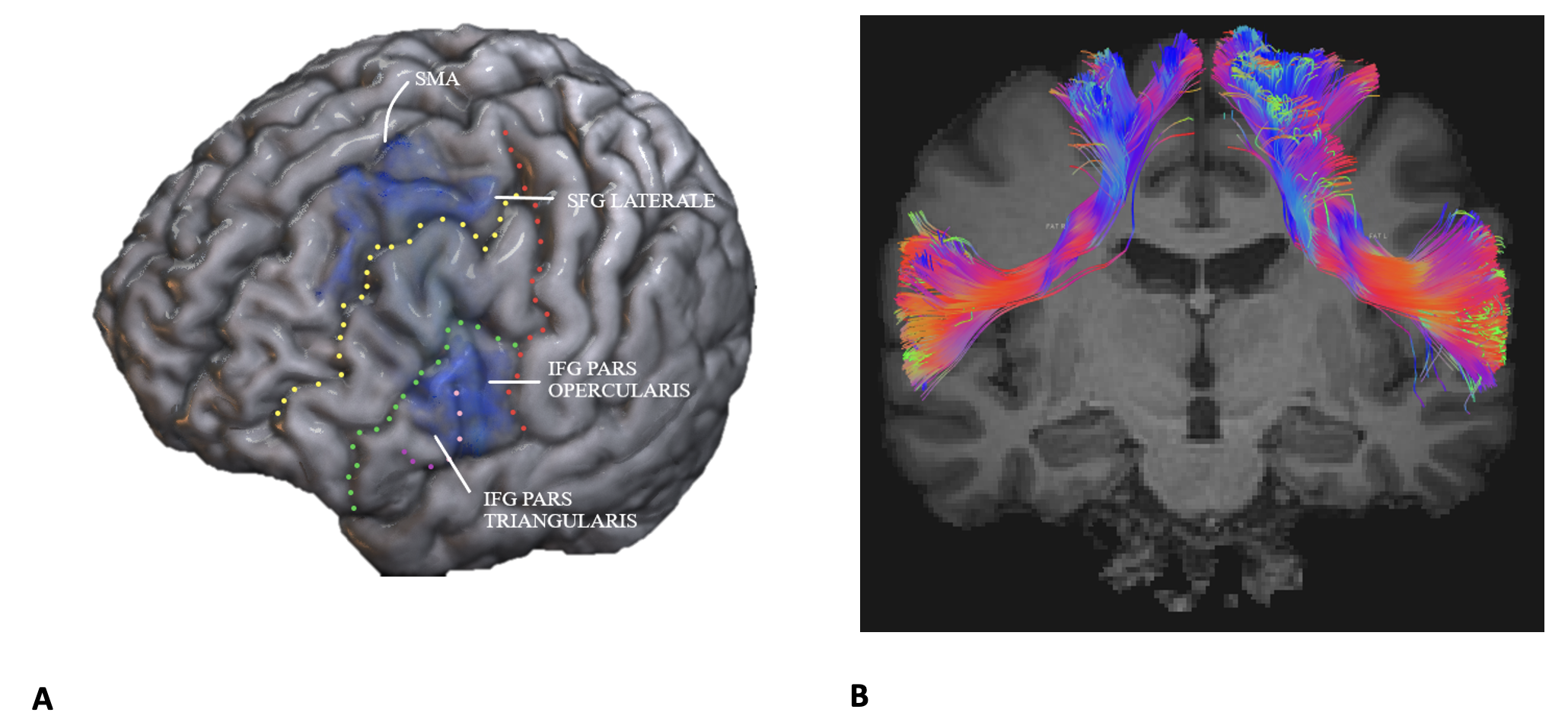
Tourette’s syndrome (TS) is a neurodevelopmental disorder characterized by motor and vocal tics that affects up to 1% of the adult population. The etiology of the syndrome is unknown, but several genetic factors seem to be implicated in the pathogenesis, determining structural changes in brain connectivity in TS. Alterations of the cortico-striatum-thalamo-cortical circuit and of the fronto-striatal tract are described In literature and further alterations are observed in the supplementary motor area (SMA) and the inferior frontal gyrus (IFG). According to our hypothesis, these alterations could include structural alteration of the frontal aslant tract (FAT), a recently described white matter tract connecting the posterior Superior and Inferior Frontal Gyri, which has aninhibitory role in motor and vocal processing that may be altered in subjects with TS. FAT alterations have also been associated to Attention Deficit And Hyperactivity Disorder (ADHD) main comorbidity of Tourette syndrome.The aim of this study is to investigate possible microstructural FAT alterations in a sample of TS patients compared to a sample of healthy controls, through diffusion MRI (dMRI). The secondary aim is to correlate the obtained metrics with clinical scales quantifying the severity of TS, namely the Yale Global Tic Severity Score (YGTSS) and the Premonity Urge For Tic Scale (PUTS), in order to elucidate any correlations between the severity of the clinical phenotype and microstructural alterations of FAT.Methods
From 2020 to 2022, 9 right-handed adults suffering from Tourette's syndrome, free from comorbidities such as ADHD, OCD, and 12 age and sex-matched healthy controls were enrolled. The mean age of TS patients and controls was 35 ± 12 years 35 ± 9 years respectively. Among patients, women were 5/9 (55.6%) and among healthy subjects 4/12 (33.3%). The neuroradiological protocol applied consists in the acquisition of a conventional diagnostic sequence and two specific sequences for the study of white matter; i) a NODDI sequence (TR=8400ms, TE=85ms, FOV=240x240mm, voxel size=2.5x2.5x2.5mm, 185 sections, two shells with b-value = 711/2400 s/mm2 and respectively composed of 30 and 61 non-collinear directions of application of diffusion gradients) and ii) a T1-weighted volumetric sequence (TR= 9.86ms, TE=4.85ms, FOV=256x256mm, voxel size=1x1x1mm, 160 sections). Raw-images were pre-processed for artifacts correction (motion, eddy, geometrical distorsions and signal drift) and for the tractographic reconstruction, by means of Constrained Spherical Deconvolution (CSD), using ExploreDTI (https://www.exploredti.com). From the reconstructed FAT we estimate four DTI metrics (fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD) and radial diffusivity (RD)) and three NODDI metrics (neurite density (ND), Orientation Dispersion Index (ODI) and free water fraction (FISO)). The FAT was reconstructed by two blinded operators. For the analysis average results between the two operators were used after verifying that the inter rater reliability (ICC) between the two operators was high for all the parameters analyzed.Neurological reassessment was performed using YGTSS and PUTS and a non-parametric correlation between the YGTSS (total, and vocal and motor scores separately) and the diffusion metrics was performed.Results
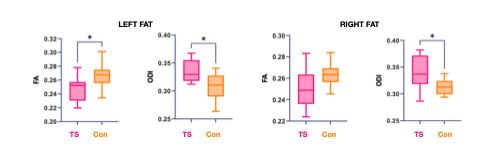
Compared to control subjects, in TS patients we observed reduced FA in the left FAT (p=0.0278) and increased ODI in both the left (p=0.0278) and the right FAT (p=0.0409).A negative correlation (p=0.0254) between motor YGTSS and Neurite Density (ND) and Free Water Fraction (FISO) was observed.A FAT lateralization in patients or controls was not observed.Discussion
We observed FA reduction and increased ODI in patients with TS suggesting anisotropy reduction and a greater dispersion of fibers.We also highlighted a negative correlation (p=0.0254) between motor tic severity and ND and FISO.In this study, for the FAT of each hemisphere, 9 metrics were analyzed. Hence, the correction for multiple comparisons was necessary. After this correction the results discussed above are no longer significant, this may be due to the small sample. In literature FAT lateralization in healthy subjects is debated, in our sample a lateralization was not observable neither in TS subjects nor in controls.Conclusions
Since in TS the alteration occurs at an early time during neurogenesis, probably for genetics reasons, numerous brain networks are involved. To our knowledge this is the first study that uses dMRI to investigate a possible correlation between TS and microstructural alterations of FAT. The obtained results, although suffering from the low sample size, are suggestive of a decreased isotropy and increased fibers dispersion in FAT, supporting the hypothesis of an involvement of the FAT in the pathogenesis of TS. In conclusion, the results obtained encourage to continue this study by enrolling new subjects.Acknowledgements
No acknowledgement found.References
La Corte, E., Eldahaby, D., Greco, E., Aquino, D., Bertolini, G., Levi, V., Ottenhausen, M., Demichelis, G., Romito, L. M., Acerbi, F., Broggi, M., Schiariti, M. P., Ferroli, P., Bruzzone, M. G., & Serrao, G. (2021). The Frontal Aslant Tract: A Systematic Review for Neurosurgical Applications. In Frontiers in Neurology (Vol. 12, p. 51). Frontiers Media S.A. https://doi.org/10.3389/fneur.2021.641586
Schlemm, E., Cheng, B., Fischer, F., Hilgetag, C., Gerloff, C., & Thomalla, G. (2017). Altered topology of structural brain networks in patients with Gilles de la Tourette syndrome. Scientific Reports. https://doi.org/10.1038/s41598-017-10920-y
Cheng, B., Braass, H., Ganos, C., Treszl, A., Biermann-Ruben, K., Hummel, F. C., Müller-Vahl, K., Schnitzler, A., Gerloff, C., Münchau, A., & Thomalla, G. (2014). Altered intrahemispheric structural connectivity in Gilles de la Tourette syndrome. NeuroImage: Clinical. https://doi.org/10.1016/j.nicl.2013.11.011
Figures