5341
Dynamic Alterations of Spontaneous Neural Activity and Its Association with Neurocognitive Function in Sport-related Concussion1Lanzhou University Second Hospital, Lanzhou, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Traumatic brain injury, fMRI (resting state), sports-related concussion
Sports-related concussion (SRC) is a complex and heterogeneous injury with psychological, cognitive, and functional consequences. Cognitive impairment is common following SRC, but the neural basis is unclear. In this study, the regional homogeneity (ReHo) and dynamic ReHo (d-ReHo) were obtained from rs-fMRI of both 31 SRC athletes and 7 non-SRC (NSRC) athletes. We found increased ReHo and d-ReHo in the SRC group, and the changes of d-ReHo in the right precuneus correlated with cognitive function. Our findings suggested that altered dynamics in the intrinsic brain activity might be a potential biomarker for explaining the cognitive function decline of SRC.Introduction
Sport-related concussion (SRC) is a major public health concern that affects millions of individuals every year1. SRC is common in collision sports, such as boxing and taekwondo, yet the chronic neurological effects of recurrent concussions and sub-concussions are still unclear. Neuroimaging biomarkers can detect the pathologic changes in gray and white matter after SRC and predict the long-term outcomes2,3. Considering that the conventional regional brain activity measurement is less sensitive to changes over time, dynamic measurement has the potential to capture the temporal variability of regional brain activity. This study aims to apply the regional homogeneity (ReHo) and dynamic ReHo (d-ReHo) to detect the regional activity differences between SRC and non-SRC (NSRC) groups and study their relationship with the neurocognitive impairment of SRC.Methods
Participants Our Institutional Review Board approved the scan protocol and written informed consent was obtained from each subject before the scan. 31 athletes (boxing and taekwondo) with a history of concussion (HoC) and 7 non-injured athletes (Kayak and rowing) with matched age, gender, and education experience were recruited. Athletes were interviewed to determine their years in sports, the number of prior concussions, and the duration since the last SRC.Neuropsychological testing All subjects underwent the same cognitive and affective measures before the MRI scan: (i) Trail Making Tests A (TMTA) and B (TMTB); (ii) the Rey Auditory Verbal Learning Test (RAVLT); (iii) Stroop Colour Naming; and (iv) Digit-span Test; (v)MoCA; (vi)Hamilton Depression Scale (HAMD); and (vii) Hamilton Anxiety Scale (HAMA).
Data Acquisition All MRI examinations were performed on a 3T MR scanner (SIGNATM Premier; GE Healthcare, Waukesha, WI, USA) with a 48-channel head coil. The T1-weighted images with 1-mm isotropic resolution were acquired using a 3D Magnetization Prepared-Rapid Gradient Echo imaging (MP-RAGE) sequence: FOV = 25.6 × 25.6 cm2, 392 slices, TR/TE = 2632/3 ms, TI = 1000 ms. Resting-state functional MRI (rs-fMRI) data were collected using gradient-echo echo-planar image (EPI) with FOV = 24 × 24 cm2, in-plane resolution = 2.5 × 2.5 mm2, 45 slices with thickness/gap = 3.2/0 mm, TR/TE = 1000/30 ms, number of volumes = 300.
Post-processing Rs-fMRI dates were pre-processed using DPARSF software (http://www.restfmri.net) based on SPM12 (http://www.fil.ion.ucl.ac.uk/spm). For ReHo, Kendall’s coefficient of concordance of the time course of every 27 nearest neighboring voxels was calculated. The d-ReHo was estimated by calculating the coefficient of variation maps of ReHo through 116 windows (a sliding window of 60 TRs (64 s) and a shifting step size of 2 TRs (2 s)) at each voxel.
Statistical analysis An independent samples t-test was applied to find the differences of ReHo and d-ReHo between the two groups. Statistical significance in the voxel level was set at P < 0.001 and the cluster level was P < 0.05 with AlphaSim corrected. Relationships between ReHo and d-ReHo measures and clinical characteristics were determined using Spearman correlation.
Results
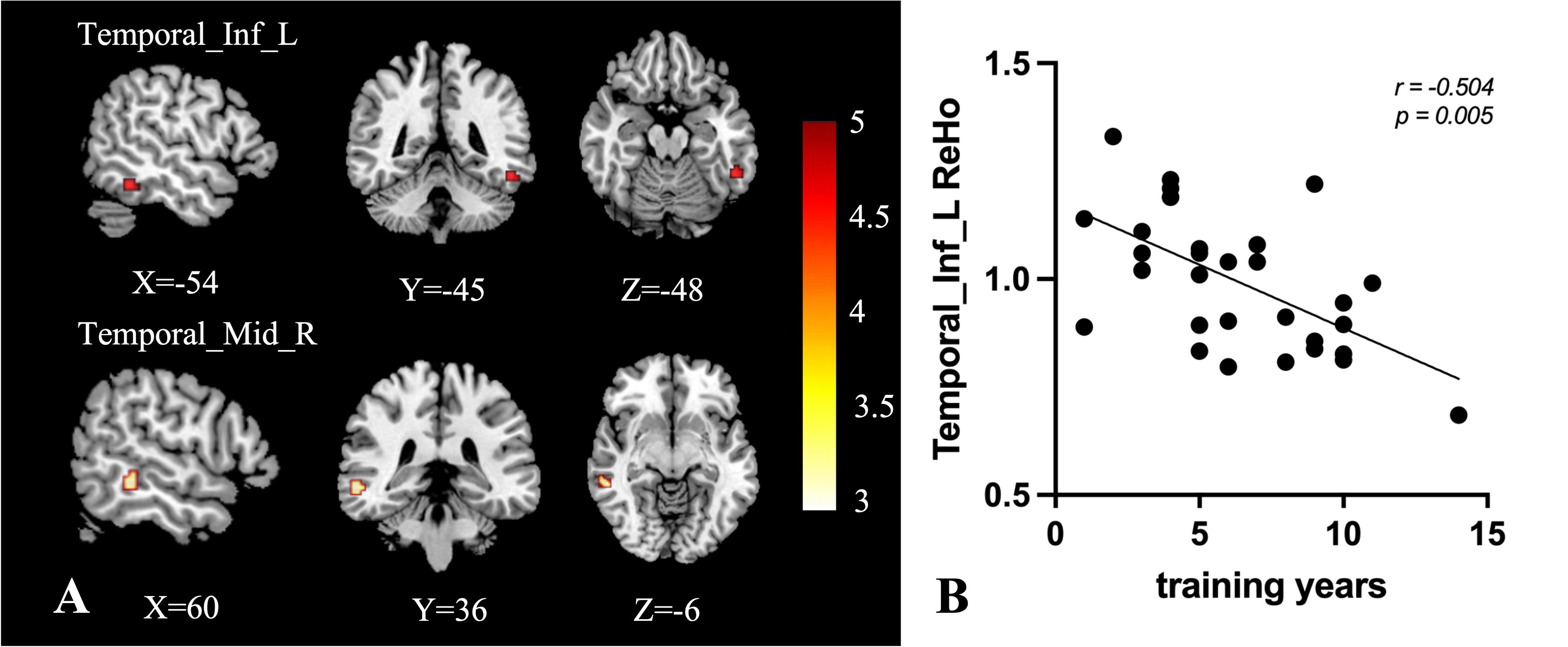
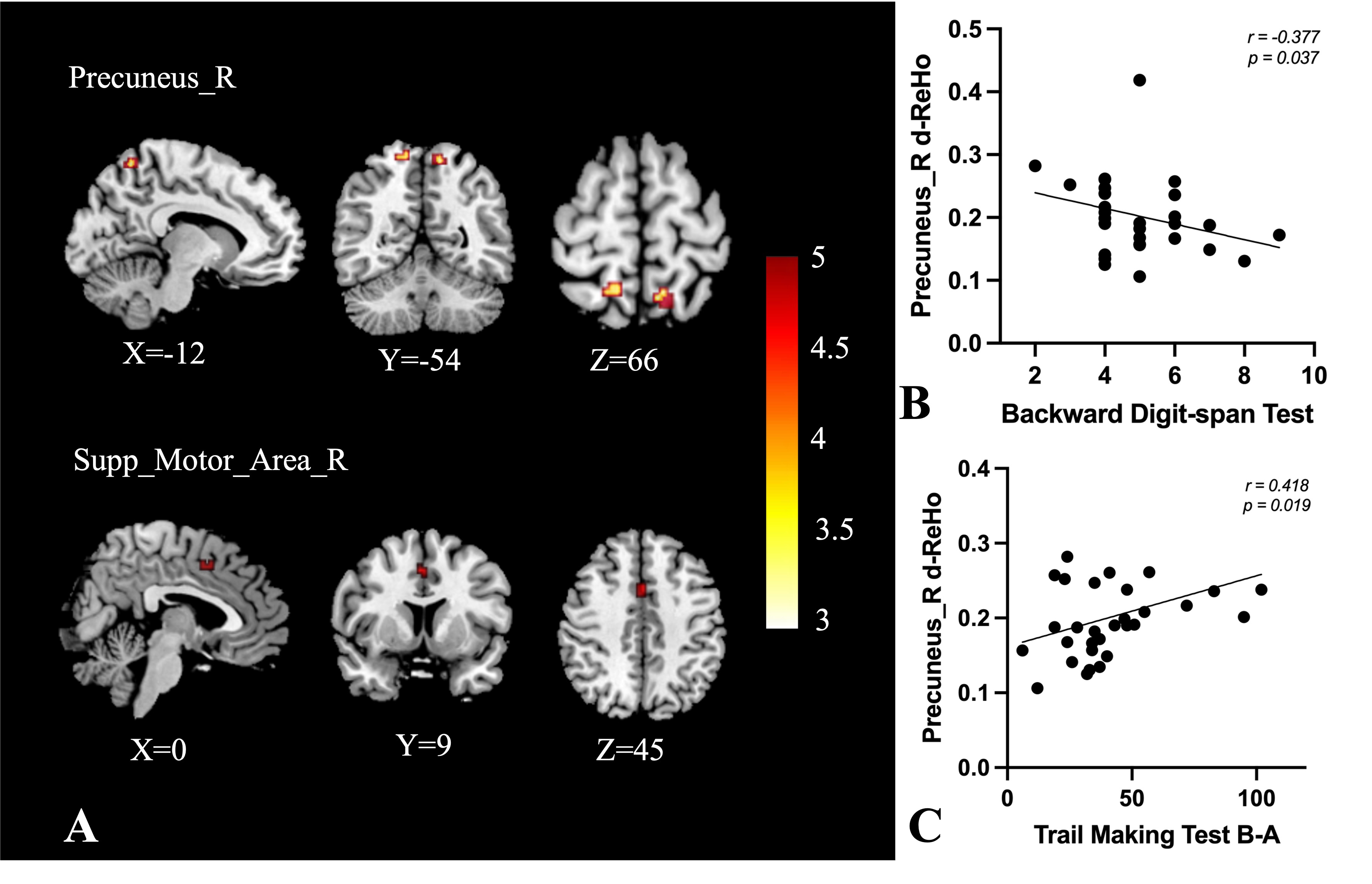
There were no group differences in age, sex composition, and years of education. Compared to the NSRC group, the SRC group had more years of training (Table 1). For the neuropsychological testing, the concussed group performed more poorly than the control groups on cognitive measures of processing speed, and executive function (Figure 1). Depression and anxiety scores were not significantly different between the two groups. The significant differences in ReHo and d-ReHo were as shown in Table 2. Compared with the NSRC group, increased ReHo was found in the left inferior temporal gyrus and the right middle temporal gyrus (Figure 2A), and increased d-ReHo was found in the bilateral precuneus and the right supplementary motor area (Figure 3A) in the SRC group. The spearman analysis showed that the ReHo in the left inferior temporal was negatively correlated with training years in the SRC group (Figure 2B). Importantly, significant correlations were found between d-ReHo in the right precuneus and cognitive measures (Figure 3B-C).Discussion
This study showed higher ReHo areas in the SRC group compared with the NSRC group. A study also report that concussed athletes had elevated ReHo at the 24 h visit but returned to normal levels by the asymptomatic visit4. In fact, multiple prior studies have documented persistent differences in rs-fMRI metrics following SRC, similar to our findings. In addition, with the increase of exercise years, ReHo of the left inferior temporal gyrus decreased, indicating that ReHo could as a reliable biomarker of SRC in determining an athlete's true level of recovery trajectory. Increased d-ReHo has been found in the bilateral precuneus and the right supplementary motor area in the SRC group in the present study. Regions with high d-ReHo were regarded as functional ‘hubs’ connecting remote brain regions5. Furthermore, dynamic functional changes in the local region could be associated with cognitive states. Increased d-ReHo of the right precuneus tends to be associated with the cognitive decline in the SRC group, indicating the role of dynamics of this area in explaining the cognitive decline of SRC.Conclusion
In conclusion, ReHo and d-ReHo measurements may enrich the diversity of methods for variation of regional brain activity to provide insight into normal brain functioning and reveal potential biomarkers of an athlete's recovery trajectory.Acknowledgements
This work was supported by the Science and Technology Project of Gansu Province (No. 21JR7RA403).References
1. GESSEL L M, FIELDS S K, COLLINS C L, et al. Concussions among United States high school and collegiate athletes [J]. J Athl Train, 2007, 42(4): 495-503.2.
2. MAJOR B, SYMONS G F, SINCLAIR B, et al. White and Gray Matter Abnormalities in Australian Footballers With a History of Sports-Related Concussion: An MRI Study [J]. Cereb Cortex, 2021, 31(12): 5331-8.3.
3. WU Y C, HAREZLAK J, ELSAID N M H, et al. Longitudinal white-matter abnormalities in sports-related concussion: A diffusion MRI study [J]. Neurology, 2020, 95(7): e781-e92.4.
4. MEIER T B, GIRALDO-CHICA M, ESPANA L Y, et al. Resting-State fMRI Metrics in Acute Sport-Related Concussion and Their Association with Clinical Recovery: A Study from the NCAA-DOD CARE Consortium [J]. Journal of Neurotrauma, 2019.5.
5. DENG L, SUN J, CHENG L, et al. Characterizing dynamic local functional connectivity in the human brain [J]. Scientific Reports, 2016, 6.
Figures
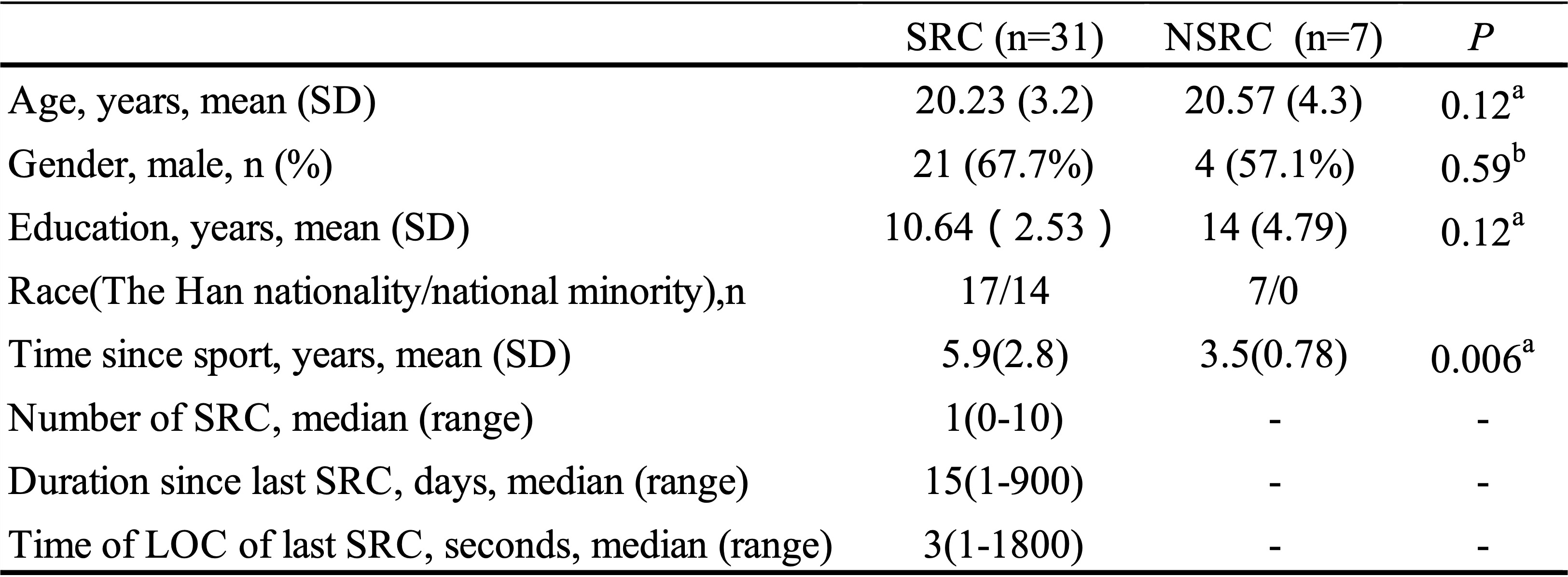
Table 1 Demographic and clinical characteristics of all participants
Note: SRC = sport-related concussion; NSRC = non-sport-related concussion; LOC = Loss of consciousness; a two-sample t-test; b chi-square t-test; Values are mean ± standard deviations (SD).
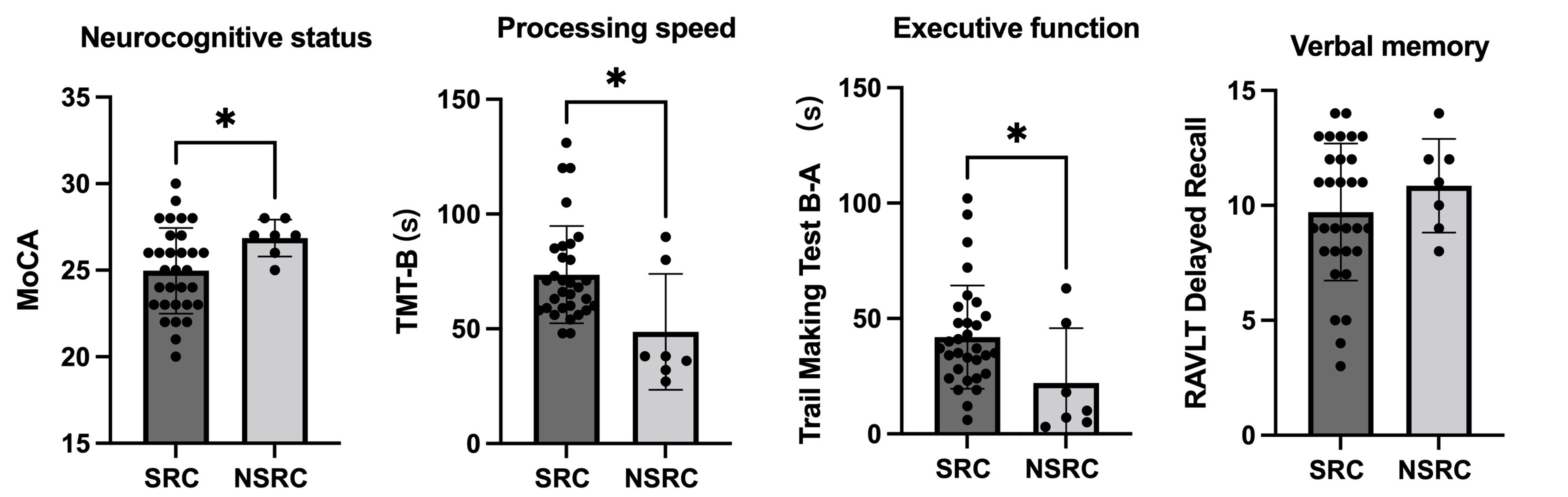
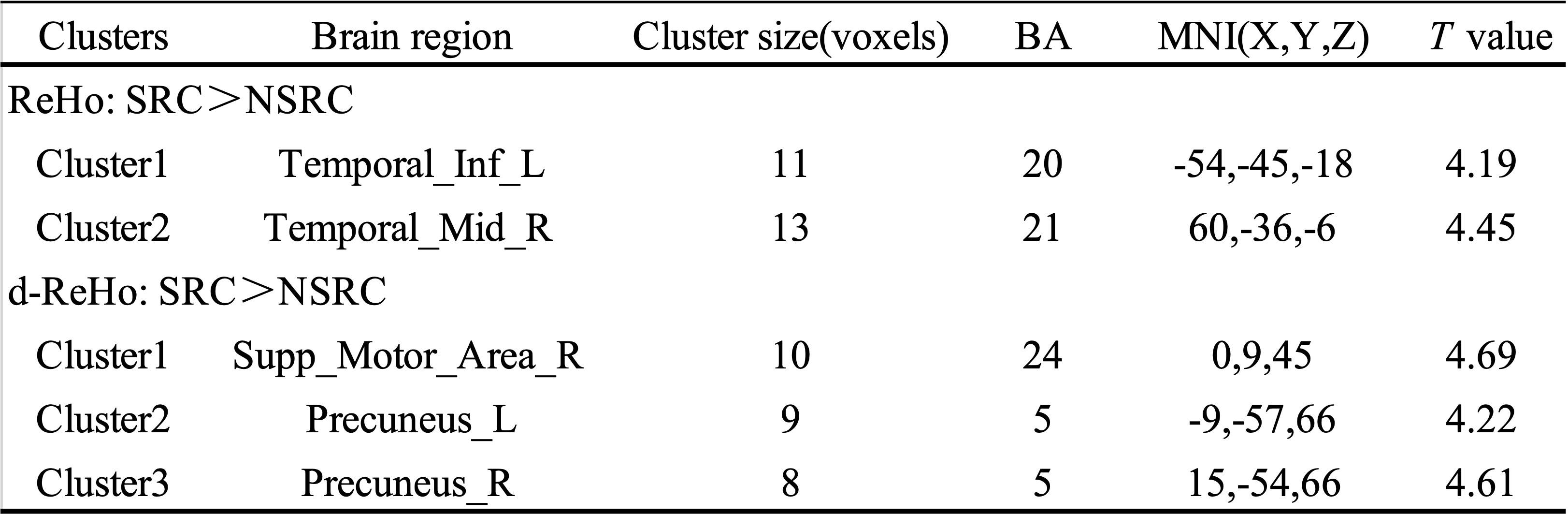
Table 2 Differences of ReHo and d-ReHo between SRC and NSRC groups
Note: SRC = sport-related concussion; NSRC = non-sport-related concussion; MNI = Montreal Neurological Institute. X, Y, Z, coordinates of primary peak locations in the MNI space. BA = Brodmann’s area. T value represents the statistic value of two sample t-tests at P < 0.001, AlphaSim corrected.