5338
Intra-plaque hemorrhage of the basilar artery is a risk factor for recurrent pontine infarction1Liaocheng People's Hospital, Liaocheng, China, 2Philips Healthcare, Shang Hai, China
Synopsis
Keywords: Blood vessels, Ischemia
Compared with the first episode of pontine acute infarction, the risk factors of the basilar artery (BA) wall of recurrent pontine acute infarction have not been fully defined. In this study, high-resolution magnetic resonance vessel wall imaging (HRMR-VWI) was used to compare the changes of BA wall in patients with first-onset and recurrent pontine acute infarction, to find the risk factors of the BA wall in patients with recurrent pontine acute infarction. The result showed intra-plaque hemorrhage (IPH) of the BA wall identified on HRMR-VWI is associated with recurrent ischemic stroke.Introduction
BA atherosclerosis is the most common cause of posterior circulation stroke. Patients with symptomatic pontine infarction often have unstable plaques of the basilar artery with higher plaque load, higher degree of stenosis and larger remodeling index, and the recurrence rate of pontine infarction is 23% higher than that of anterior circulation infarction. 1 But among these vulnerable features, the risk factor for recurrent pontine infarction is not defined, and determination of factors associated with pontine stroke recurrence can help optimize clinical management to prevent future strokes. 2 HRMR-VWI is an effective, reproducible, and convenient technique to identify atherosclerotic lesions. This study compared patients who have first-onset stroke with ones who have recurrent stroke, to investigate the association between BA plaque features and recurrent pontine stroke.Methods
MRI experimentsAll scans were performed on a 3T MR scanner (Ingenia; Philips Healthcare, Best, The Netherlands) with a 16-channel phased-array head coil.The imaging parameters for the HRMR-VWI were TR, 800 ms; TE, 18.0 ms; field of view 200×186×105 mm3, NSA 1. Acquisition voxel size was 0.5 ×0.6×0.5 mm3. The cross-sections were constructed automatically with 0.5 mm slice thickness. Additionally, all patients also underwent DWI (b value=1000 s/mm²; TR/TE = 2900/94 ms), T2-weighted imaging (Turbo Spin Echo; TR/TE = 3000/80 ms) and time of flight imaging (three-dimensional fast gradient echo; TR/TE = 25/3.5 ms).SubjectsFrom October 2019 to May 2021, 73 patients (male: female=41:32, mean age=66.40±11.00 years) with acute pontine infarction diagnosed according to DWI were enrolled. All of the patients were subdivided into first-onset group (n = 46) and recurrent group (n = 27) according to the presence of malacoplakia or not in T2-weighted image. The IPH, remodeling index, plaque area, lumen stenosis rate, and plaque load of the basilar artery were compared between the two groups. The ROC curve was used to determine the predictive value of plaque area, luminal stenosis rate, and plaque load on the recurrence of pontine infarction.Results
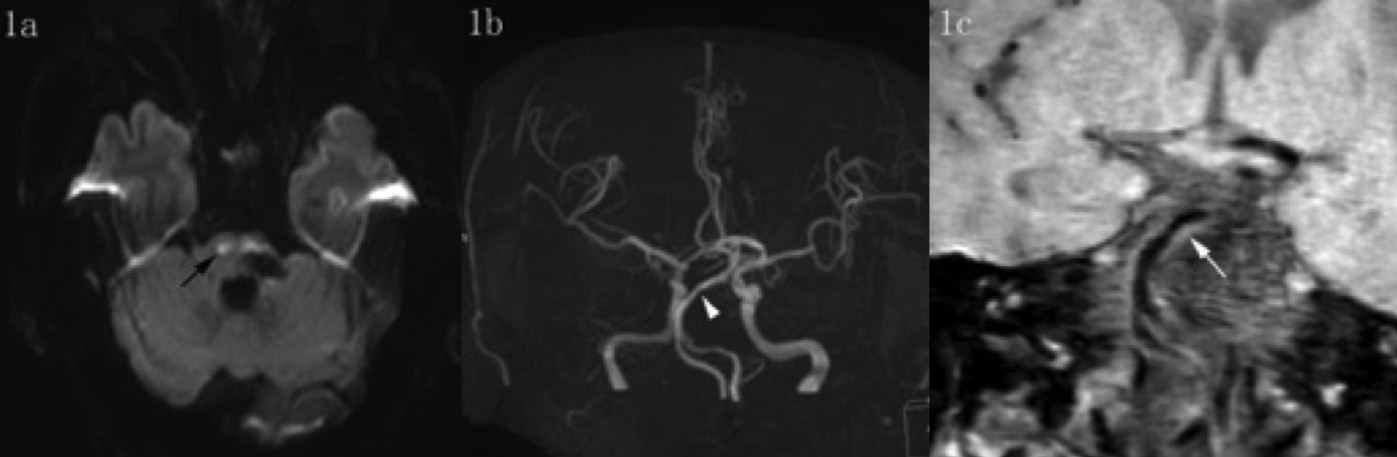
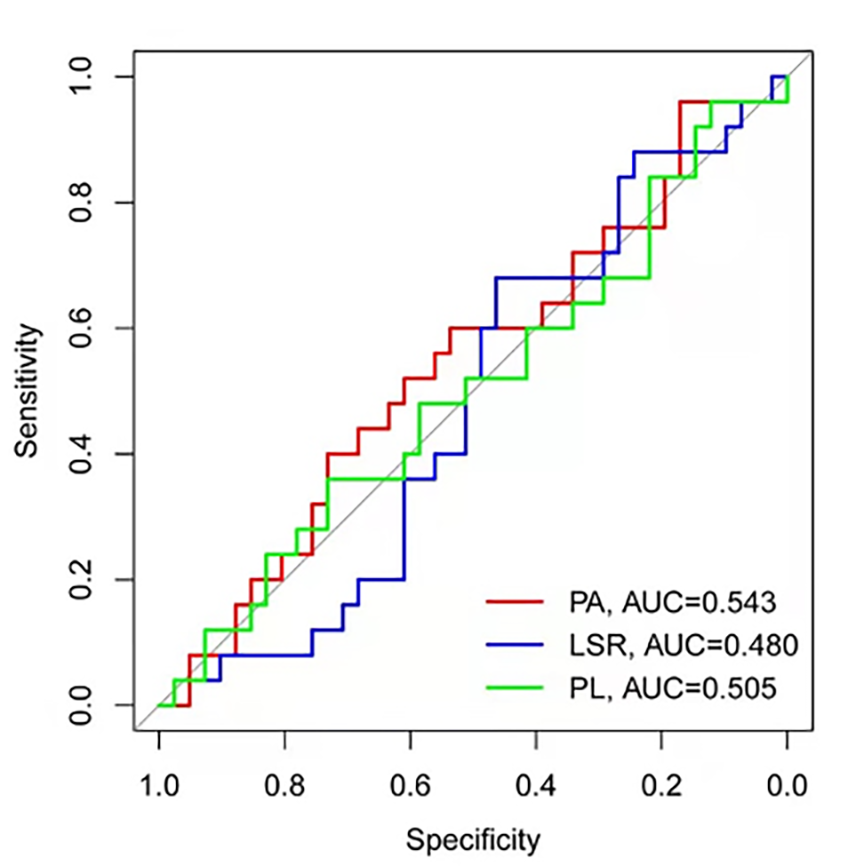
The rate of IPH in the recurrent group was higher than that in the first-onset group (10/27 VS 7/46, P= 0.033, Fig 1a-c), and the difference was statistically significant. Compared with the first-onset group, the recurrent group had a greater rate of positive remodeling (21/27 VS 28/46),although statistical significance was not achieved, a trend towards significance was observed for this parameter (P=0.138). There was no significant difference in plaque area[(5.57±4.91)mm2 VS (7.35±5.28)mm2, P =0.556], lumen stenosis rate[(50.17±26.78)% VS (48.31±21.82)%, P=0.771], and plaque load [(34.11±17.10)% VS (34.07±16.43)%, P=0.993] between the two groups. The ROC curve analysis of plaque area, lumen stenosis rate, and plaque load revealed a predictive ability no better than chance (AUC was 0.543, 0.480 and 0.505, respectively, Fig 2).Discussion
The presence of IPH is a feature of vulnerable plaques, which was shown in previous studies, and is associated with acute cerebral infarct. 3In the progression of atherosclerotic plaque, IPH is an accelerating factor and can increase the risk of rupture.4 In this study, comparing other features in vulnerable plaque, IPH of basilar artery plaque is also a risk factor for the recurrence of pontine infarction. Ran et al 2 reported higher plaque burden of the middle cerebral artery (MCA)was associated with recurrent ischemic stroke, but in this study, high plaque burden of the BA did not show association with pontine ischemic stroke. Maybe the difference in hemodynamics between MCA and BA is the reason for it.Limitations of this study: no contrast-enhanced scan was performed. However, HRMR-VWI plain scan can provide most of the information on basilar artery plaque. Without contrast agent injection, it can evaluate the risk factors of recurrence with multiple parameters, which is conducive to popularization in clinical application.Acknowledgements
This abstract is supported by Science Foundation of Liaocheng People’s Hospital (No. LYQN201924).References
1. Abuzinadah AR, Alanazy MH, Almekhlafi MA, et al. Stroke recurrence rates among patients with symptomatic intracranial vertebrobasilar stenoses: systematic review and meta-analysis. J Neurointerv Surg 2016;8:112-116.
2. Ran Y, Wang Y, Zhu M, et al. Higher Plaque Burden of Middle Cerebral Artery Is Associated With Recurrent Ischemic Stroke: A Quantitative Magnetic Resonance Imaging Study. Stroke 2020;51:659-662.
3. Yang D, Liu Y, Han Y, et al. Signal of Carotid Intraplaque Hemorrhage on MR T1-Weighted Imaging: Association with Acute Cerebral Infarct. AJNR Am J Neuroradiol 2020;41:836-843.
4. Takaya N, Yuan C, Chu B, et al. Presence of intraplaque hemorrhage stimulates progression of carotid atherosclerotic plaques: a high-resolution magnetic resonance imaging study. Circulation 2005;111:2768-2775.
Figures