5322
Effects of MR-Guided Focused Ultrasound Pallidotomy on Dyskinesia and Cerebral Regional Homogeneity in Parkinson’s Disease1Diagnostic Radiology and Nuclear Medicine, University of Maryland, School of Medicine, Baltimore, MD, United States, 2University of Maryland, School of Medicine, Baltimore, MD, United States, 3Neurosurgery, University of Maryland, School of Medicine, Baltimore, MD, United States, 4Neurology, University of Maryland, School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: Parkinson's Disease, Focused Ultrasound
MR-guided Focused Ultrasound (MRgFUS) pallidotomy is a promising, non-invasive neurosurgical approach for treating the primary and secondary symptoms, such as levodopa-induced dyskinesia, of Parkinson’s Disease (PD). While the behavioral effects of MRgFUS pallidotomy in PD have been previously established, its impacts on brain circuity and how these changes relate to symptom resolution are currently unclear. In the current study, we compared measures of Regional Homogeneity (ReHo), a metric of spatiotemporal correlation thought to reflect the integrity and modularity of mesoscopic circuity, before and after FUS lesion of the Globus Pallidus internus (GPi).Introduction
MR-guided Focused Ultrasound (MRgFUS) pallidotomy is a promising, non-invasive neurosurgical approach for treating the primary and secondary symptoms, such as levodopa-induced dyskinesia, of Parkinson’s Disease (PD). While the behavioral effects of MRgFUS pallidotomy in PD have been previously established1, its impacts on brain circuity and how these changes relate to symptom resolution are currently unclear. In the current study, we compared measures of Regional Homogeneity (ReHo)2, a metric of mesoscopic spatiotemporal correlation that has been shown to be reliably disrupted in PD, before and 1 month after MRgFUS lesion of the Globus Pallidus internus (GPi). By comparing post-surgical ReHo changes against ReHo abnormalities previously reported in the PD literature3, we were able to evaluate whether MRgFUS pallidotomy reverses these ReHo abnormalities and they relate to behavioral outcomes.Methods
Imaging:MRI were acquired on a 3T Siemens Tim Trio MR scanner. T1 structural images were acquired in the sagittal orientation using a MPRAGE GRAPPA protocol and imaging parameters of repetition time (TR) = 2300 ms, echo time (TE) = 2.98 ms, flip angle (FA) = 90, field of view (FOV) = 240 x 256 mm2, and voxel size = 1 x 1 x 1 mm3. For resting stage fMRI, T2*-weighted images were acquired using a 2D single-shot EPI sequence with TE = 30 ms, TR range = 3.14 – 3.75 seconds, slice range: 52-63, voxel size 2.7 × 2.7 × 2.7 mm3, and a total of 200 volumes acquired over ~ 11min.
Subjects:
Data was collected from eleven patients (7 Male, Age: mean = 55.63, range = 40 -74) participating in a prospective, IRB-approved, multicenter study of GPi pallidotomy for the treatment of motor complications of Parkinson’s disease (registration no. NCT02263885). MRI were acquired pre-treatment and 1 month post MRgFUS treatment. Behavioral Data were collected pre-treatment and 1, 3, 6, and 12 months after treatment.
Data Preprocessing:
Structural T1-MPRAGE and rs-fMRI data were preprocessed using the default pipeline in the CONN toolbox4 (i.e., realignment to the mean, slice-time correction, segmentation, normalization, and smoothing). Nuisance variables, including estimates of rotation and translation of the head and BOLD signals from WM and CSF were regressed from functional images to remove motion and non-neuronal contributions to the estimated BOLD signal. In addition, TRs containing extreme amounts of frame-wise movement were censored from further analysis.
Regional Homogeneity (ReHo) was calculated using the Integrated Local Correlation (ILC) algorithm5. Voxel-wise Integrated Local Correlation was investigated using a 25mm FWHM Kernel and ILC values were z-scored on a per image basis to ensure that each ILC map had a mean of 0 and standard deviation of 1.
Statistical Analysis:
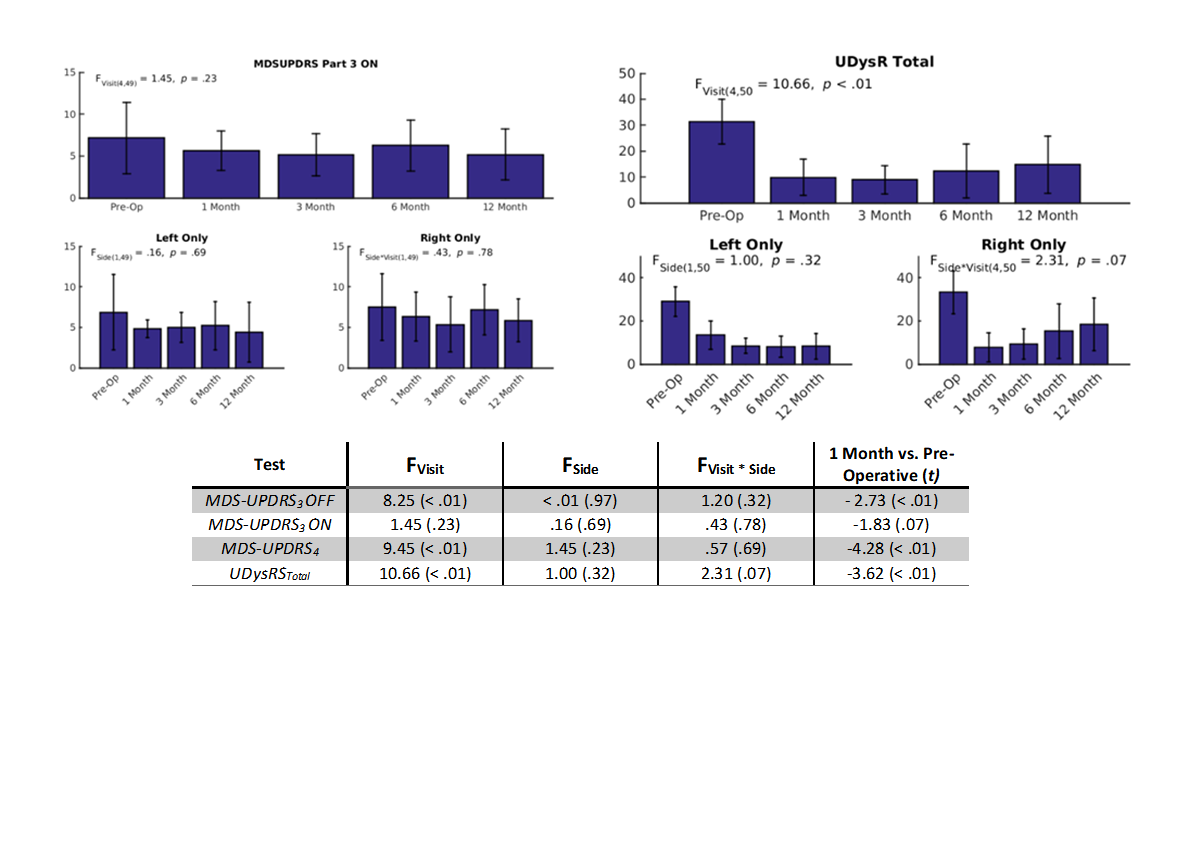
Scores from the MDS-UPDRS Part 3 (The Movement Disorder Society sponsored revision of the Unified Parkinson’s Disease Rating Scale) and UDysRS Total (The Unified Dyskinesia Rating Scale ) were analyzed with linear mixed models including fixed effect terms for Visit (Pre-Operative, 1 Month, 3 Month, 6 Month, and 12 Months Post-Operative), Lesion Side (Right & Left) and the interaction between Visit and Lesion Side as well as a random effects intercept for each individual patient.
Whole-brain, voxel-wise ReHo was analyzed with a paired T-test comparing the Pre-Operative and 1 Month time points and evaluated using an uncorrected height threshold of p < .01 and an FDR-corrected cluster-level threshold of p < .05. In addition, ReHo changes were predicted using a multiple regression model including terms for changes to the MDS-UPDRS Part 3, UDysRS Total, as well as total lesion volume.
Results
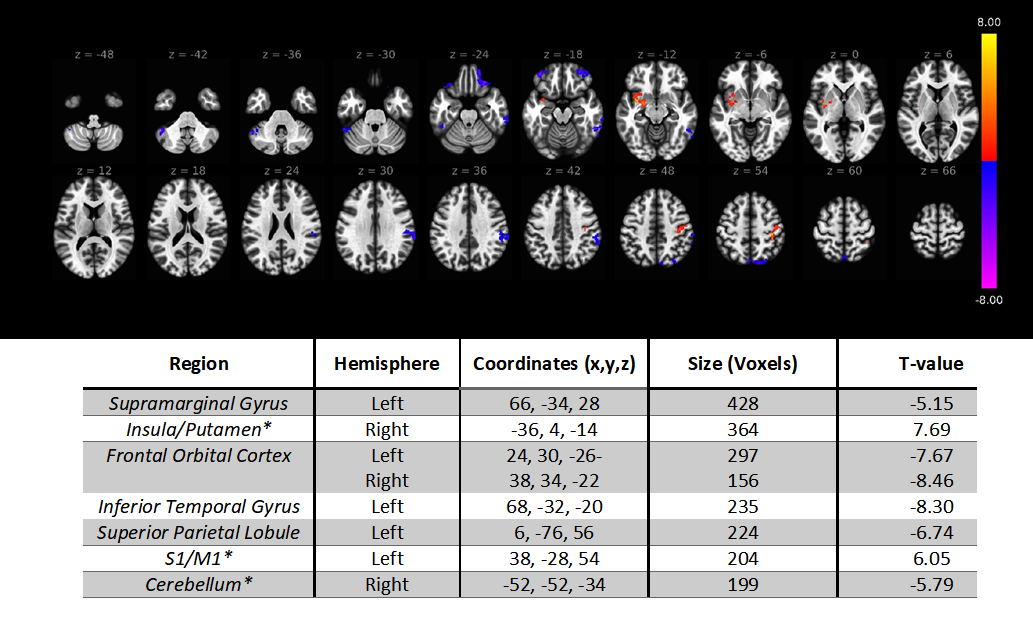
Figure 1 displays changes to the MDS-UPDRS Part 3 and UDysRS Total following GPi Pallidotomy. Significant decreases were observed in both the MDS-UPDRS Part 3 (Pre-Operative: mean = 19.46, s.d. = 3.91; 1 Month: mean = 11.00, s.d. = 4.77; t(50) = -2.73, p < .01) and UDysRS Total (Pre-Operative: mean = 31.31, s.d. = 8.59; 1 Month: mean = 9.81, s.d. = 6.98; t(50) = -3.62, p < .01).Figure 2 displays the brain regions demonstrating significant changes to ReHo following GPi Pallidotomy (warm = increase, cool = decrease). Significant clusters are documented in the associated table and regions demonstrating reversals of previously reported abnormalities are indicated with a star (*).
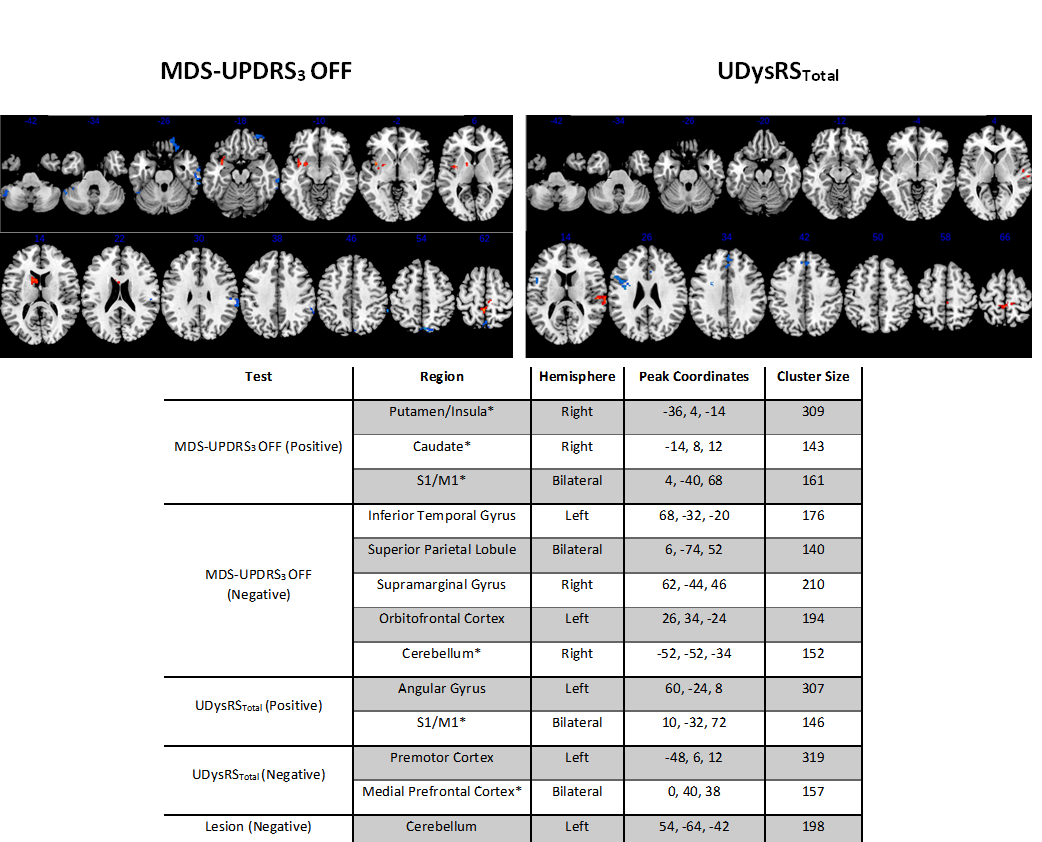
Figure 3 displays brain regions demonstrating significant correlations between ReHo changes and changes to behavioral outcomes (warm = positive correlation, cold = negative correlation). Significant clusters are documented in the associated table and regions demonstrating reversals of previously reported abnormalities are indicated with a star (*).
Discussion
One month after MRgFUS pallidotomy, PD patients demonstrated improvements in primary and dyskinesia symptoms as well as robust changes to ReHo in several notable regions. The observed ReHo changes in S1/M1, Insula/Putamen, medial Prefrontal Cortex, and Cerebellum are particularly striking as they represent reversals of previously documented ReHo abnormalities in PD3. For example, cerebellar ReHo has been previously found to be increased in PD but was found to have decreased after MRgFUS pallidotomy. Conversely, S1/M1 & Putamen ReHo has been reported to be decreased in PD but was found to have increased following MRgFUS pallidotomy. In total, these results provide some of the first insights into the neural mechanisms by which MRgFUS pallidotomy may combat disease progression in PD.Acknowledgements
No acknowledgement found.References
1. Eisenberg, H. M., Krishna, V., Elias, W. J., Cosgrove, G. R., Gandhi, D., Aldrich, C. E., & Fishman, P. S. (2020). MR-guided focused ultrasound pallidotomy for Parkinson’s disease: safety and feasibility. Journal of Neurosurgery, 135(3), 792-798.
2. Zang, Y., Jiang, T., Lu, Y., He, Y., & Tian, L. (2004). Regional homogeneity approach to fMRI data analysis. Neuroimage, 22(1), 394-400.
3.Pan, P., Zhan, H., Xia, M., Zhang, Y., Guan, D., & Xu, Y. (2017). Aberrant regional homogeneity in Parkinson’s disease: a voxel-wise meta-analysis of resting-state functional magnetic resonance imaging studies. Neuroscience & Biobehavioral Reviews, 72, 223-231.
4. Whitfield-Gabrieli, S., & Nieto-Castanon, A. (2012). Conn: a functional connectivity toolbox for correlated and anticorrelated brain networks. Brain connectivity, 2(3), 125-141.
5. Deshpande, G., LaConte, S., Peltier, S., & Hu, X. (2009). Integrated local correlation: a new measure of local coherence in fMRI data. Human brain mapping, 30(1), 13-23.
Figures