5307
Free breathing, multi-shot real-time imaging using adaptive k-space sampling (ARKS) for iCMR
Nuri Chung1, Ana Rodriguez-Soto2, Sanjeet Hegde3, Eleanor L. Schuchardt3, Brent M. Gordon3, Ileen Cronin3, and Francisco Contijoch1,2
1Bioengineering, University of California San Diego, La Jolla, CA, United States, 2Radiology, University of California San Diego, La Jolla, CA, United States, 3Pediatrics, Rady Children's Hospital-San Diego, Heart Institute, San Diego, CA, United States
1Bioengineering, University of California San Diego, La Jolla, CA, United States, 2Radiology, University of California San Diego, La Jolla, CA, United States, 3Pediatrics, Rady Children's Hospital-San Diego, Heart Institute, San Diego, CA, United States
Synopsis
Keywords: Cardiovascular, Heart
Adaptive k-space sampling (ARKS) enables real-time multi-shot imaging by quickly finding data acquired during similar cardiac phases1. In this study, we used pediatric physiologic signals to simulate ARKS and extended the approach to incorporate respiratory gating and enable free breathing acquisition. Respiratory gating was performed by cross-correlating the recent respiratory signal with previously acquired values. A correlation cutoff was used to select similar periods. As expected, higher correlation cutoffs led to lower acceptance rates. For a search period of 32 beats, respiratory gating with a correlation cutoff of 0.5 identified 6 heartbeats for multi-beat imaging.Introduction
iCMR imaging relies on real-time, low latency, single-shot acquisitions for guidance of catheterization. As a result, image quality is limited by both the amount of data and time available for image reconstruction. Adaptive radial k-space sampling (ARKS) is an approach that could enable multi-shot data collection in real-time1 and thus benefit iCMR. However, to date, ARKS has been applied for adults performing breathholds and therefore does not account for respiratory motion, which will occur in sedated patients undergoing iCMR. Additionally, children physiologically experience prominent sinus arrhythmia, or RR variation with the respiratory cycle. In this study, we extend ARKS to incorporate respiratory phase information and enable free breathing, multi-shot real-time data acquisition.Methods
This study had IRB-approved waiver of consent. ECG data and respiratory waveforms were recorded from 10 sedated children during 4D flow imaging (median age: 1.9 years old, age IQR: 0.5-8 years, 60% female). The median heart rate (HR) was 106.8 bpm (IQR: 85.1 to 126.3 bpm).A 2D radial bSSFP acquisition was simulated with a TR= 2.6ms for 200 seconds for each patient (MATLAB 2022b, Mathworks, Natick MA). Figure 1 shows how we simulated the cardio-respiratory gating process.
Briefly, ARKS has previously shown that cross-correlation of the ECG can quickly and robustly identify prior periods of similar cardiac phase and collect a multi-beat dataset1,2. For each patient, the most recent ECG data (first row, black points) is cross correlated across the entire time window. The short window was set as the median RR interval based on trigger values detected by the scanner. In this work, we add analysis of the respiratory signal via cross-correlation of the respiratory waveform. Since respiratory trigger/cycle information was not available, the respiratory search window (second row, black points) was set to 4 times the duration of the ECG search interval. The cross-correlation result (bottom) is shown for the ecg (blue) and respiratory (red) signals. ECG peaks are automatically detected and selected if the cross-correlation value was >0.9 (horizontal dashed black line). Respiratory gating was applied by only selecting ECG peaks (black points) with respiratory correlation greater than the respiratory cross correlation threshold (shown by thick red points). The respiratory cutoff threshold was 0.5 in this example.
We evaluated the impact of respiratory gating on the number of beats accepted for multi-shot reconstruction as well as the respiratory acceptance rate (i.e., the ratio of accepted beats to overall beats in the search window). We evaluated the impact of the respiratory cutoff threshold and the impact of varying the overall search window from 16 to 64 heartbeats.
Results
The respiratory correlation cutoff (RCC) was strongly, inversely correlated to the number of beats (Nbeats) and acceptance rate (AR) of the multi-shot approach (Figure 2). Specifically, Nbeats= -14.6 RCC + 13.7, r2=0.997 and AR = -0.50 RCC +0.50, r2=0.9987, respectively.A lower respiratory cutoff value accepts more beats but enforces less stringent respiratory similarity. RCC = 0.25 led to AR=35.7% (IQR: 30.0-36.7%) while a RCC=0.75 led to AR=14.3% (IQR: 6.6-16.4%). For a search window of 32 RR-intervals, this led to selection of 9.5 and 3 beats for multi-shot imaging, respectively. RCC=0.5 resulted in an AR=24.4% (IQR: 15.5-26.8%) and acceptance of 6 beats (IQR: 4-8 beats).
Nbeats varied as a function of the overall time window (Figure 2, top right) but narrowing or extending the overall search window did not significantly affect the acceptance rate (Fig 2, bottom right).
Discussion
Respiratory gating was successfully combined with an ECG-based approach to perform real-time, multi-shot imaging. The cross-correlation is a fast approach to analyze respiratory signals and enables control over the acceptance/rejection of data via a correlation cutoff. While the time window duration impacted the number of beats available for multi-shot imaging, it did not affect the acceptance rate which suggests a specific cutoff could be identified based on physiologic variation and applied to multiple imaging scenarios.Conclusion
Multi-shot imaging could significantly improve the quality of real-time imaging by increasing the amount of data available for reconstruction and decreasing the demands on the reconstruction algorithm. However, robust identification of data at the correct cardio-respiratory phase is challenging. We’ve shown that ARKS can be adapted to analyze cardio- and respiratory phase information in children to generate free breathing, multi-shot imaging data in fast approach compatible with real-time imaging.Acknowledgements
No acknowledgement found.References
1. Contijoch F, Han Y, Kamesh Iyer S, et al. Closed-loop control of k-space sampling via physiologic feedback for cine MRI. PLoS One. 2020;15(12):e0244286. Published 2020 Dec 29. doi:10.1371/journal.pone.0244286
2. Chung N, Rodriguez-Soto A, Hegde S, Lehnert Schuchardt E, Gordon BM, Cronin I, Contijoch F. Adaptive k-space sampling enables multi-shot real-time imaging in pediatric patients. Paper will be presented at: 26th Annual Society for Cardiovascular Magnetic Resonance; January 27, 2023; San Diego, CA
Figures
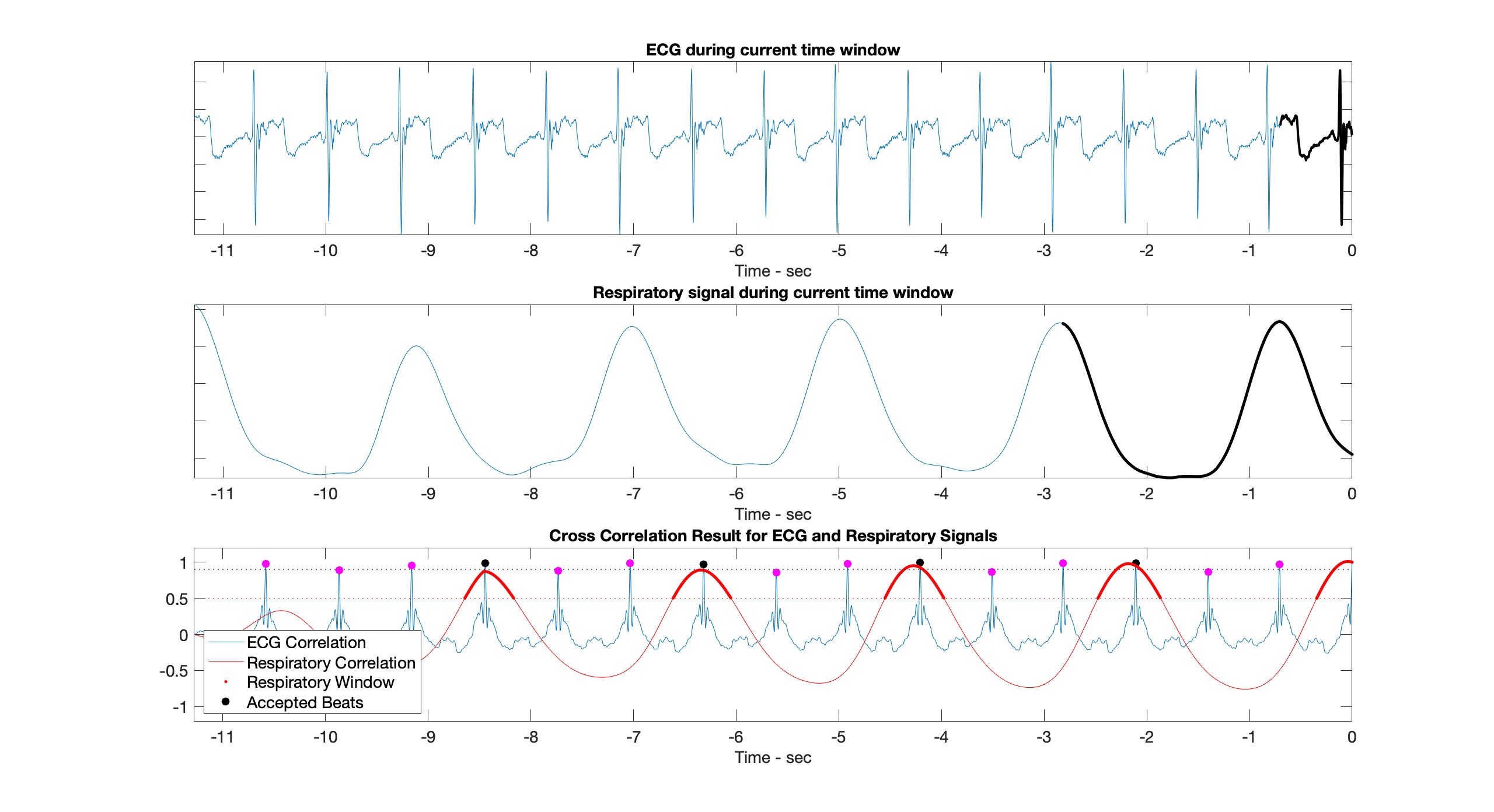
Figure 1. Example analysis of ECG and respiratory signals. Top: Recent ECG signal (16 RR intervals). The most recent 1 RR interval is shown in black. Middle: Recent respiratory signal. Respiratory period was assumed to be 4 times the median RR interval (most recent portion is shown in black). Bottom: Cross-correlation results illustrate both ECG and respiratory matching. ECG beats are only accepted (black) if they coincide with the correct respiratory position (dark red line) based on a respiratory cutoff (horizontal dashed line, 0.5) and an ecg cutoff (black-dashed line, 0.9)
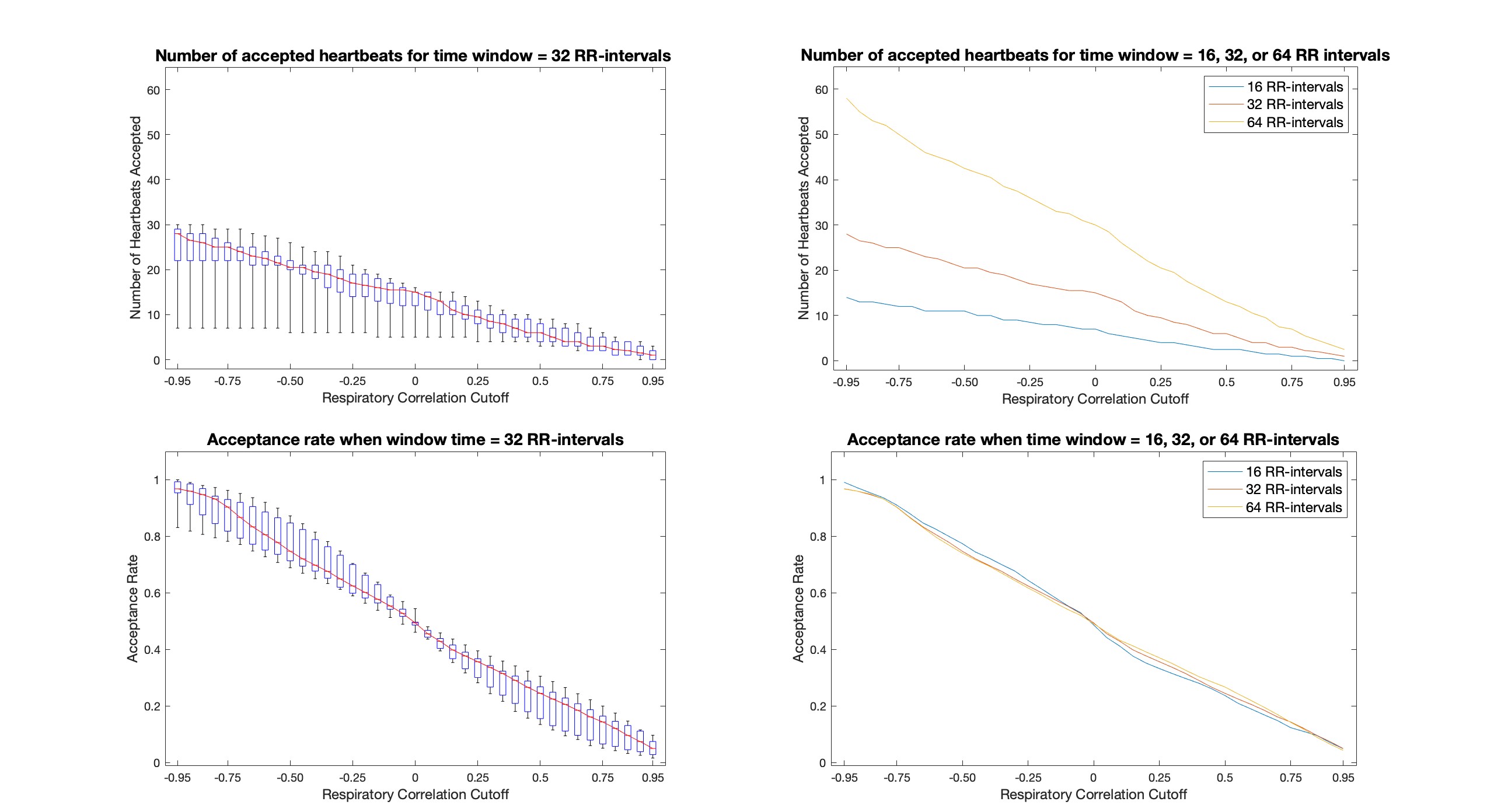
Figure 2. Left: The impact of respiratory correlation cutoff on the number of beats accepted (top) and the acceptance rate (bottom) illustrate how the extent of respiratory gating can be controlled. Box plots represent interquartile ranges and the whiskers span the minimum and maximum values. Right: Application of cardio-respiratory gating to shorter/longer periods changes the number of accepted beats but does not affect the acceptance rate.
DOI: https://doi.org/10.58530/2023/5307