5290
Characterisation of pregnancies affected by pre-eclampsia using MRI1Centre for the Developing Brain, King's College London, London, United Kingdom, 2Department of Women and Children's Health, King's College London, London, United Kingdom, 3GKT School of Medicine, King's College London, London, United Kingdom, 4Centre for Medical Engineering, King's College London, London, United Kingdom
Synopsis
Keywords: Fetal, Fetus, Placenta; hypertension; clinical translation
Maternal cardiac, placental and fetal brain anatomical and functional MRI was obtained in 63 pregnancies, including 12 with pre-eclampsia. In pregnancies affected by pre-eclampsia, placental T2* was significantly reduced compared to normal pregnancy. All women with placental histopathological anomalies consistent with pre-eclampsia showed a reduced placental T2*. Fetal brain T2* was significantly lower in women with pre-eclampsia than those without, although brain volume was maintained. In women with pre-eclampsia, reduced fetal brain T2* was associated with middle cerebral artery Doppler abnormalities. Cardiac work was increased in women with pre-eclampsia.Summary of main results
Pre-eclampsia is significantly associated with decreased placental and fetal brain T2*.Introduction
Pre-eclampsia occurs in 2-5% of pregnancies and is associated with maternal and fetal mortality and serious morbidity [1]. Maternal risks include a life-long increase in cardiovascular disease [2]. In their infants, there is increased risk of cognitive dysfunction, but antenatal effects on brain development have been difficult to disentangle from the impact of subsequent iatrogenic preterm birth [3]. The complex pathophysiology of the disease calls for comprehensive assessment in pregnancy. We describe a multi-system approach to MRI investigation of pre-eclampsia with acquisition of maternal cardiac, placenta and fetal brain anatomical and functional imaging.Methods
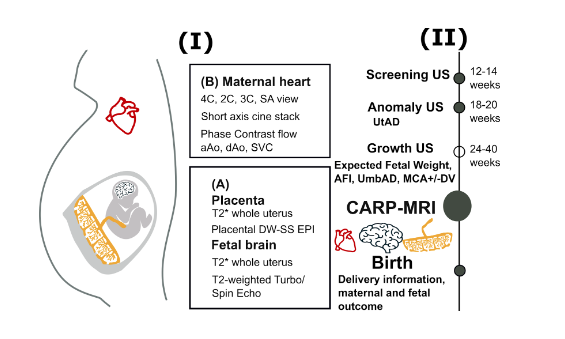
A prospective observational study was performed from 2019-2022 at Guy’s and St Thomas’ NHS Foundation Trust (London Dulwich Ethics Committee 08/LO/1958), recruiting healthy pregnant women, those with chronic hypertension, and those with pre-eclampsia. Clinical parameters including fetal ultrasound as well as information on maternal and neonatal outcomes were obtained. Controls who subsequently developed pregnancy pathologies were excluded. In addition, participants recruited from other ethically approved studies with similar cohorts were included in the analysis (London Dulwich Ethics Committee 16/LO/1573). The study protocol is summarised in Figure 1.An MRI scan was performed in two 30 minute blocks (‘A’ and ‘B’, alternating starting block between participants to remove bias associated with maternal anxiety) on a clinical 1.5T Philips Ingenia scanner using a 28 channel torso coil in maternal supported supine position with constant monitoring of physiological parameters and frequent verbal interaction.
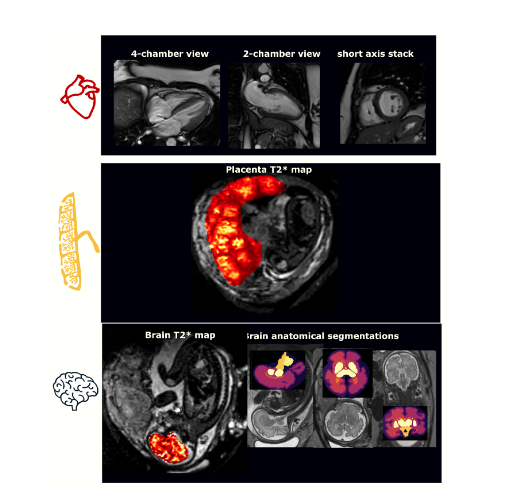
Block “A” included whole uterus anatomical TSE sequences in five planes (resolution 1.5x1.5x2.5mm, FOV=320x320x110mm, TE=180ms) as well as whole uterus multi-echo gradient-echo single-shot EPI (2.5mm isotropic, FOV=300x300x110mm, TE=11, 58, 117, 176ms) and a placental-focused diffusion-weighted single-shot EPI scan (1 b=0, 6 b=375, 6 b=750; transverse relaxation (TR)=6.6ms, TE=78ms, matrix = 512x512x56, resolution 2x2x4mm). Block “B” focused on the maternal heart including 4-chamber, 2-chamber, 3-chamber and short axis cardiac bSSFP sequences (30 cardiac phases, 11 second breath-hold, FA=60, TE/TR~2/4ms, resolution=1.7x1.7x8mm) as well as a whole short axis cine stack and phase-contrast flow measurements on the ascending aorta, descending aorta and superior vena cava (30 phases, 14 second breath-holds, sense=2, resolution=2.5x2.5x8mm). Total scan time was under 60 minutes. Obtained images are summarised in Figure 2.
The fetal brain and placenta images were segmented manually in all functional/T2* scans and T2* fitting was performed by mono-exponential decay using in-house scripts. Resulting quantified parameters were whole placental volume, T2* values, derived histogram skewness and kurtosis, fetal brain volume and T2* values. Key maternal cardiac parameters including mean blood pressures, cardiac output (defined as heart rate x stroke volume) and cardiac work (defined as cardiac output x aortic pressure, hence describing ventricular contractility) were determined.
Results
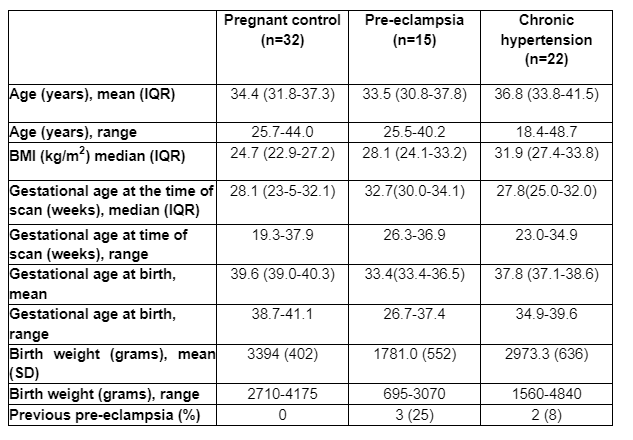
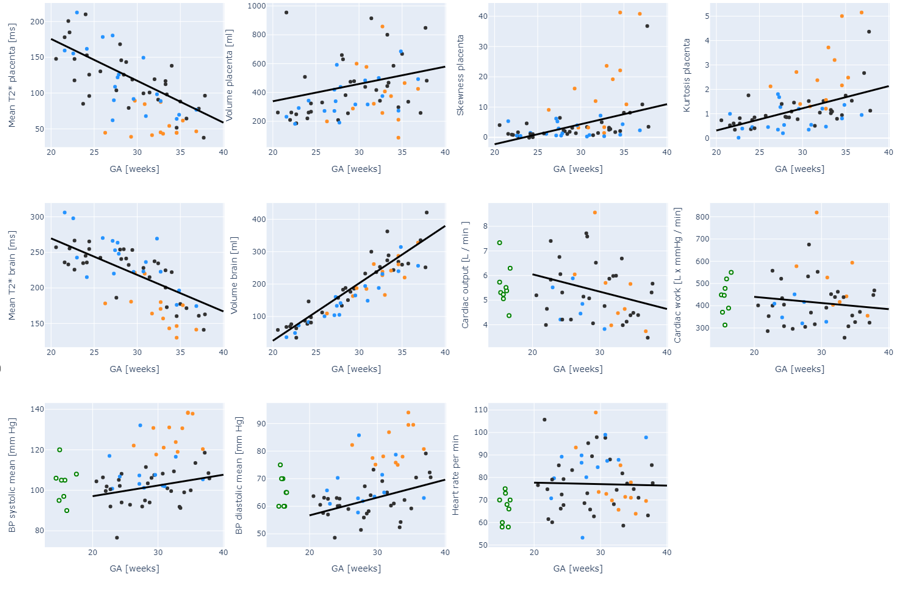
65 women were recruited; 11 had repeat scans (nine had two, and two had three scans); giving a total of 87 MRI scans. Cardiac assessment was not completed in two women: one owing to claustrophobia, and the other to worsening hypertension. No cardiac data were obtained for the 16 women included from the second study. 32, 22 and 15 women were included in the control, chronic hypertensive and pre-eclamptic cohorts respectively. Mean gestational age at birth and birthweight were significantly lower in the pre-eclampsia cohort compared to controls (39.6 versus 33.4 weeks’ gestation and 3394 vs 1781g respectively) (Figure 3).Placental T2* declined with gestational age in control pregnancies (6.5 ms/week) only and was significantly reduced in those with pre-eclampsia (p<0.001) and, to a lesser degree, in the chronic hypertension group. Placental volume was consistent across all cohorts. Placental T2* kurtosis and skewness were increased in pre-eclampsia compared to both other cohorts (p<0.001). All pre-eclamptic patients with abnormal placental T2* also had placental histopathological features of pre-eclampsia; in contrast, those with normal T2* values did not.
Brain T2* declined in the control cohort (5 ms/week) and was significantly reduced in the pre-eclampsia cohort (p<0.001 compared to the control group). Abnormal brain T2* in the pre-eclampsia cohort was significantly correlated with contemporaneous evidence of cerebral redistribution on Doppler US (p=0.03). Brain volumes increased with gestational age (18ml/week) and were not significantly different in the presence of pre-eclampsia (summarised in Figure 4).
Blood pressure was increased in chronic hypertensive and pre-eclamptic patients; there was an increasing non-significant trend in cardiac work in women with pre-eclampsia.
Discussion and conclusion
This study presents the first comprehensive MR-based analysis of women with pre-eclampsia encompassing the maternal cardiac system, placenta and the fetal brain. Reduced placental T2* values confirm trends observed in the literature [4,5]. The correlation between placental T2* and histopathology adds weight to MRI as a valuable antenatal predictive tool. Reduction in fetal brain T2* in women with pre-eclampsia is a novel finding that provides support that pre-eclampsia may compromise antenatal brain development, potentially through associated fetal growth restriction, and highlights MRI’s value in increasing in vivo understanding of obstetric disease. Further understanding of these effects, including longitudinal data in evolving pre-eclampsia, in relation to fetal growth restriction and associated Doppler studies, and linked to longer-term neonatal outcomes, would be valuable and may impact antenatal care, suggested treatments, and timing of delivery.Acknowledgements
The authors thank all pregnant women and their families for taking part in this study. The authors thank the research midwives and radiographers for their crucial involvement in the acquisition of these datasets. This work was supported by a Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z], a UKRI FL fellowship, an NIHR Fellowship [301664] and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z]. The views presented in this study represent these of the authors and not of Guy's and St Thomas' NHS Foundation TrustReferences
[1] Roberts CL, Ford JB, Algert CS, Antonsen S, Chalmers J et al. Population-based trends in pregnancy hypertension and pre-eclampsia: an international comparative study. BMJ Open (2011) 24:1(1):2000101
[2] Okoth K, Chandan, JS, Marshall T, Thangaratinam S, Thomson GN, Niranthakakumar K, Adderley NJ. Association between reproductive health of young women and cardiovascular disease in later life: Umbrella review. BMJ (2020) 7(371):m3502
[3] Gumusoglu SB, Chilukuri ASS, Santillan DA, Santillan MK, Stevens HE. Neurodevelopmental outcomes of prenatal pre-eclampsia exposure. Trends Neurosci (2020) 43(4):253-68
[4] Sinding M, Sorensen A, Hansen DN, Peters DA, Frokjaer JB, Petersen AC. T2* weighted placental MRI in relation to placental histology and birth weight. Placenta (2021) 114(10):52-5
[5] Ho AEP, Hutter J, Jackson LH, Seed PT, McCabe L, Al-Adnani M, Marnerides A, George S, Story L, Hajnal JV, Rutherford MA, Chappell LC. T2* placental magnetic resonance imaging in preterm pre-eclampsia: An observational cohort study. Hypertension (2020) 75(6):1523-31
Figures