5243
Indirectly Prediction of Cardiac Adverse Events Based on Hemodynamics Change Induced by Exercise Using 4D flow MRI
Jiali Li1, Qian Liu1, Min Tang1, Wanying Qi1, Qianfeng Luo1, Tao Liu1, Xiaoyong Zhang2, and Jing Chen1
1The Affiliated Hospital of Southwest Medical University, Luzhou, China, 2Clinical Science, Philips Healthcare, Chengdu, China
1The Affiliated Hospital of Southwest Medical University, Luzhou, China, 2Clinical Science, Philips Healthcare, Chengdu, China
Synopsis
Keywords: Heart, Cardiovascular
In this study, we aimed to implement and evaluate methods for indirectly prediction of cardiac adverse events inside athletes based on hemodynamic changes in heart and aorta of four-dimensional (4D) flow MRI. The results showed that advanced parameters such as wall shear stress, energy loss and relative differential pressure were increased in athletes' hearts with late gadolinium enhancement and/or cardiac remodeling compared to controls, and the probability of remodeling in the exercising heart could be predicted by predictive models. This suggests that exercise-induced hemodynamic changes could be detected by 4D flow, which could predict the occurrence of adverse cardiovascular events.Introduction
As a special group, athletes' health has been widely concerned. More and more sudden deaths due to cardiovascular adverse events of athletes have been reported1,2. Sports will increase the cardiovascular load, which can be reflected by hemodynamic parameters3. Four-dimensional flow MRI (4D flow MRI) could be used to analyze complex hemodynamic models in vivo by quantifying blood flow parameters and deriving characteristics. The aim of this present study was to obtain the hemodynamic changes of the heart and aorta in athletes for predicting the risk of myocardial late gadolinium enhancement (LGE) and/or cardiac remodeling (CR).Methods
This study was approved by the institutional ethics committee. 213 athletes and 32 matched sedentary health controls were prospectively enrolled for cardiac magnetic resonance (CMR) examination on a clinical 3.0T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany), equipped with a 18-channel body coil. Four-dimensional flow was performed with the scan parameters listed as follows: TE = 2.88 ms; echo spacing = 5.7 ms; TR = 45.36 ms; spatial resolution = 1.8 × 1.8 × 3.5 mm3; velocity encoding = 150 cm/s in all three velocity-encoding directions. Routine cardiac cine and LGE sequences were also conducted for references. The cardiac function, 4D flow parameters (Figure 1) for the left ventricle and aorta (plane 1-8), and myocardial LGE extent were measured and compared between two groups, positive athletes group with LGE and/or CR and negative athletes group. The least absolute shrinkage and selection operator penalized regression was used to construct the clinical prediction model for LGE and/or CR. Continuous variables were compared using the t-test or Mann-Whitney U-test between athletes and controls, positive and negative groups; p<0.05 was considered statistically significant.Results
In the exercise group, there were 35 male exercisers with CR. Moreover, nine male exercisers with myocardial LGE in left ventricle (LV) were found. For 4D flow parameters, 9 indexes of LV and 10–17 indexes of the aorta in planes 1–8 have a statistically significant difference between controls and exercises (p < 0.05), including wall shear stress, energy loss, some general parameters of the aorta and volume, and peak velocity of the LV. The wall shear stress and energy loss were higher in athletes, general parameters of the aorta and volume, and peak velocity of the LV were lower in athletes. Within the positive and negative groups in exercisers, there was a statistically significant difference for 17 indexes of LV and 4–7 indexes of aorta planes, including wall shear stress, relative pressure and some general parameters. The wall shear stress and relative pressure were higher in positive group, general parameters were lower higher in positive group (p < 0.05). The prediction model with the area under the receiver operating characteristic curve of 0.806, included the factors of weight, maximum wall shear stress, maximum relative differential pressure of plane 7 of aorta, and aortic valve net positive volume (Figure 2).Conclusion
There were statistical increase of wall shear stress, relative pressure, and energy loss in the athletes compared with sedentary controls, which may not be potentially beneficial to the heart and aorta. Furthermore, a clinical prediction model of CR and/or LGE, including hemodynamic parameters, was successfully constructed with good prediction efficiency and excellent goodness-of-fit value. It is suggested that the 4D flow CMR has the applicable value for assessing the hemodynamic changes and predicting the cardiac adverse events for athletes, which should provide an adoptive frequency for follow-up and exercise plan.Acknowledgements
noneReferences
1. Emery, M. S. & Kovacs, R. J. Sudden Cardiac Death in Athletes. JACC Heart Fail 6, 30–40 (2018).
2. Landry, C. H. et al. Sudden Cardiac Arrest during Participation in Competitive Sports. N Engl J Med 377, 1943–1953 (2017).
3. Liu, H.-L. et al. Efficacy and Safety of Pulmonary Arterial Hypertension-specific Therapy in Pulmonary Arterial Hypertension: A Meta-analysis of Randomized Controlled Trials. Chest 150, 353–366 (2016).
Figures
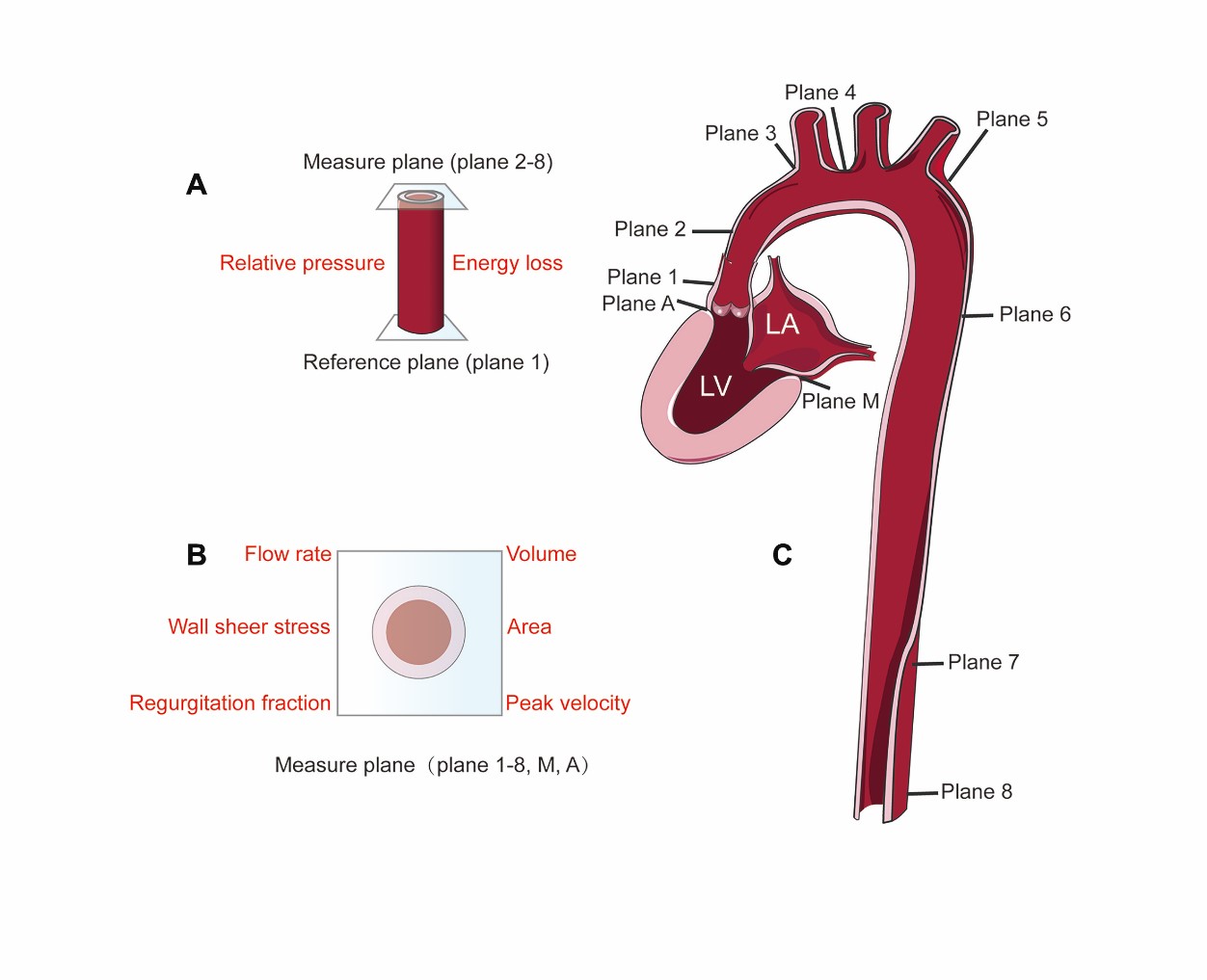
Figure
1: Measured sketch of 4D flow parameters.
Figure (A)(B) shows the parameters that can be
measured in 4D flow images. Figure (C) shows the left ventricular hemodynamic
parameters measured and the eight measurement planes set up according to aortic
hemodynamics.
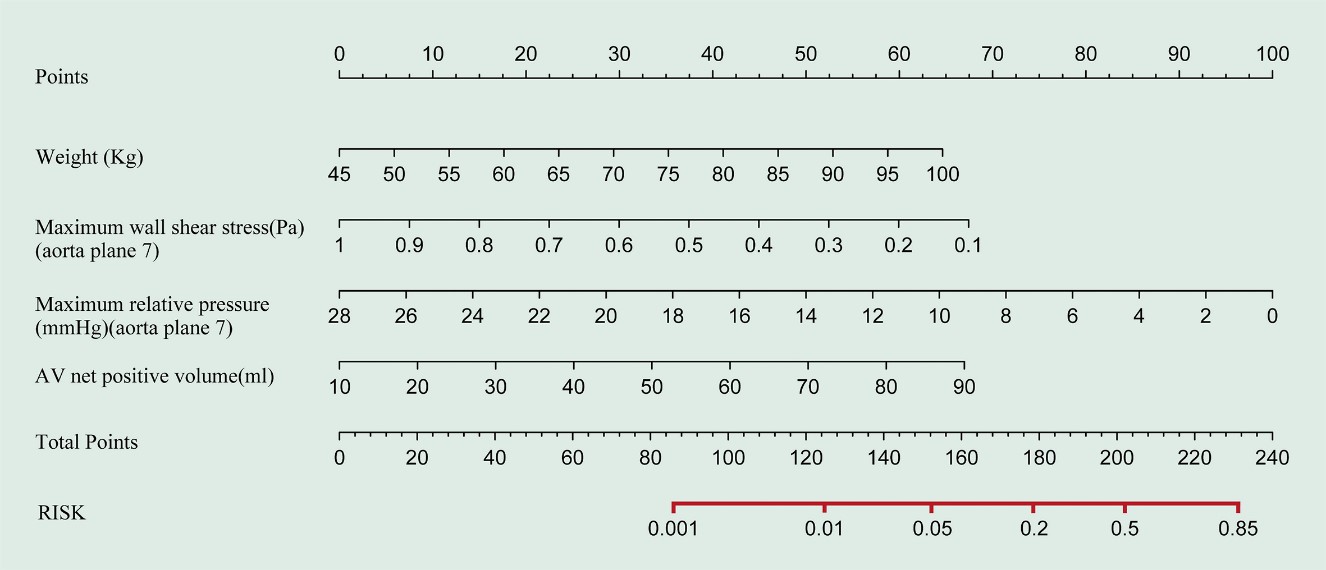
Figure
2: The nomogram of the clinical prediction model for cardiac remodeling and/or
late gadolinium enhancement.
Each value within these variables was
assigned a score on the point scale. By summing up the total score and locating
it on the total point scale, we could get the nomogram-predicted probability.
Note:
AV, aortic valve.
DOI: https://doi.org/10.58530/2023/5243