5173
Multi-orientation ZOOMit diffusion-weighted imaging in the preoperative T staging of gastric cancer1Department of Radiology, the First Affiliated Hospital with Nanjing Medical University, Nanjing, China, 2MR Collaboration, Siemens Healthineers Ltd, Shanghai, China, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Diffusion/other diffusion imaging techniques, Diffusion/other diffusion imaging techniques, ZOOMit diffusion-weighted imaging
Magnetic resonance imaging has been demonstrated to be a useful tool in the preoperative diagnosis of gastric cancer. With improved imaging quality and flexible imaging orientation, ZOOMit diffusion-weighted imaging (DWI) is attracting attention in gastric tumor imaging. The stomach is a hollow organ with variable morphology. Thus, multi-orientation ZOOMit DWI imaging provides a complete view of the lesion compared with axial DWI, thus leading to more accurate preoperative staging in treatment strategy determination.Introduction and aim
The early detection and accurate preoperative staging of gastric cancer (GC) are crucial for treatment strategy determination. Magnetic resonance imaging (MRI) has been reported to be comparable to multi-detector computed tomography in the local staging of GC 1. Diffusion-weighted imaging (DWI) can help assess the depth of tumor invasion by providing excellent soft tissue contrast between malignant tissues and normal walls. Nevertheless, conventional DWI is usually acquired with axial orientation, and information can be missed. However, ZOOMit DWI 2 selectively excites a small region of interest, and fewer phase encodings enable single-shot acquisition on any orientation with reduced artifacts. This study aimed to determine the added value of coronal and sagittal ZOOMit DWI images in improving the accuracy of GC T staging compared with axial images only.Method
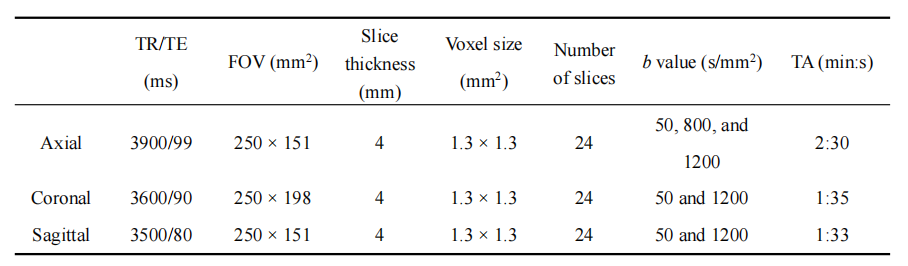
In this prospective study, 47 patients with endoscopically proven GC, who underwent gastric MRI between June 2022 and September 2022 were included. All patients underwent MRI on a 3T scanner (MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany) with an 18-channel body coil. The protocol of the research application ZOOMit DWI sequence with tilted excitation plane 3 is depicted in Table 1. Fifteen patients with unresectable factors and 2 patients with poor image quality were excluded from this study. Two experienced radiologists independently evaluated the T staging of each patient on both axial images only and multi-orientation images. In the case of disagreements on the T staging of a patient, the radiologists would discuss the case until an agreement was reached. All reviewers were blinded to the surgical and pathologic findings but were aware that the patients had GC. The accuracy of T staging evaluation was compared using the chi-square test or Fisher's exact test between the 2 methods.Results
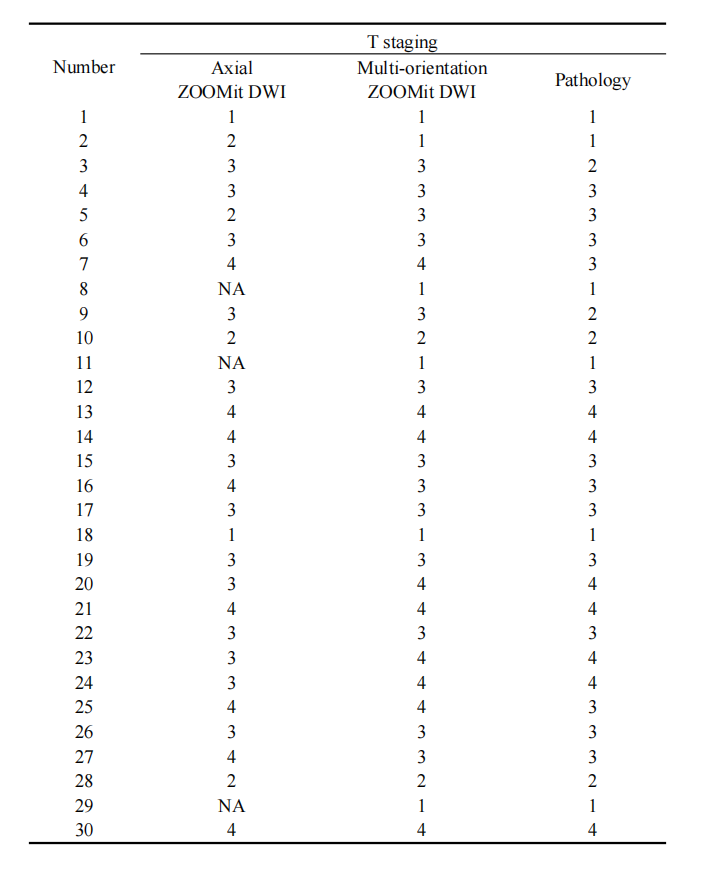
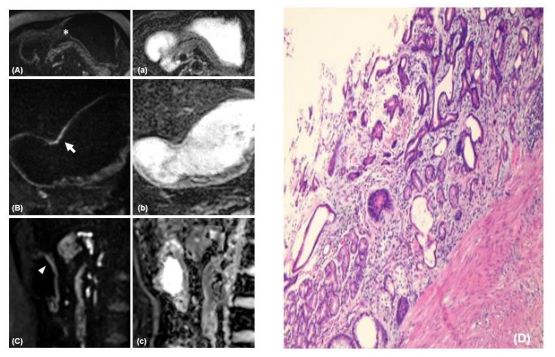
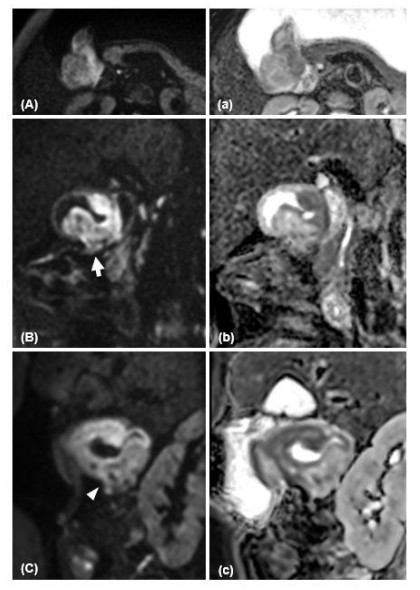
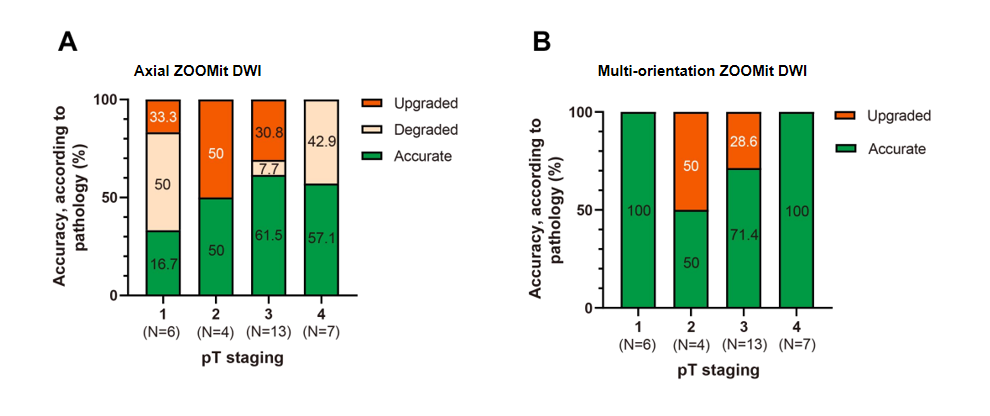
Thirty patients (age range, 40–80 years; mean age, 63.7 years) were included. Pathologically, 6 patients had early-stage GC (EGC, pT1) and 24 patients had advanced GC (AGC, pT2–pT4). Of the 30 enrolled patients, 16 were diagnosed correctly with both axial and multi-orientation images. The multi-orientation ZOOMit DWI images corrected 10 cases of wrong staging using axial DWI. In 3 of the 10 patients, the lesions of EGC were not detected on axial images; however, they were depicted distinctly on coronal or sagittal images (Table 2 and Fig. 1). Five patients with AGC were adjusted to achieve a correct T staging evaluation (Table 2 and Fig. 2). Overall, the multi-orientation ZOOMit DWI images were superior to axial DWI in predicting GC T staging (P < 0.01), especially in pT1 and 4 (Fig. 3).Discussion
Conventional DWI is limited in imaging orientation for body imaging due to serious image distortion along the phase-encoding direction when field of view is large. However, detecting EGC with axial DWI may be difficult especially when the tumor is confined to the submucosal layer. ZOOMit DWI selectively excites a small region of interest and can use all image orientations with small image artifacts. Current data suggested that multi-orientation DWI outperformed axial DWI. Three patients had relatively smooth lesions in the axial DWI, implying no signs suggesting T4. However, a breakthrough of the serosa was seen in the coronal or sagittal position. In addition, the lesions in 2 patients were considerably irregular on axial images, whereas lesions were still confined to the serosa in other orientations, especially coronal images. This could be explained by partial volume effects when the gastric wall was tangent to the axial scan, such as at the greater or lesser curvature of the gastric antrum or angle. The higher diagnostic accuracies of the T3- and T4-stage cancers using multi-orientation DWI than axial DWI indicated its clinical importance for AGC. The depth of invasion of a tumor is one of the remarkable prognostic factors for patients with GC: the 5-year survival rate markedly decreases to less than 50% in the case of serosa invasion 4.Conclusion
The multi-orientation ZOOMit DWI improves the capability for detecting early-stage GC and identifying the serosa invasion status of advanced GC.Acknowledgements
No acknowledgement found.References
1. Joo I, Lee J M, Kim J H, et al. Prospective comparison of 3T MRI with diffusion-weighted imaging and MDCT for the preoperative TNM staging of gastric cancer[J]. Journal of magnetic resonance imaging: JMRI, 2015, 41(3): 814–821.
2. Hu Lei, Wei Liming, Wang Shuhao, et al. Better lesion conspicuity translates into improved prostate cancer detection: comparison of non-parallel-transmission-zoomed-DWI with conventional-DWI.[J].Abdom Radiol (NY), 2021, 46: 5659-5668.
3. Finsterbusch Jürgen, Improving the performance of diffusion-weighted inner field-of-view echo-planar imaging based on 2D-selective radiofrequency excitations by tilting the excitation plane.[J]. J Magn Reson Imaging, 2012, 35: 984-92.
4. Zhang X-F, Huang C-M, Lu H-S, et al. Surgical treatment and prognosis of gastric cancer in 2,613 patients[J]. World Journal of Gastroenterology, 2004, 10(23): 3405–3408.
Figures