5159
MRE navigator for rapid estimation of liver stiffness.1Charité - Universitätsmedizin Berlin, Berlin, Germany, 2MR Application Development, Siemens Healthcare, Erlangen, Germany, 3Physikalisch-Technische Bundesanstalt(PTB), Braunschweig and Berlin, Berlin, Germany, 4University of Wisconsin, Madison, WI, United States, 5Experimental and Clinical Research Center (ECRC), DZHK partner site Berlin, Berlin, Germany, 6HELIOS Klinikum Berlin Buch, Berlin, Germany
Synopsis
Keywords: Elastography, Data Acquisition
MR elastography (MRE) can noninvasively detect liver fibrosis based on elevated stiffness values. However, a complete MRE scan is time-consuming and typically extends over multiple breath-holds. Therefore, a multi-shot gradient echo sequence with spiral readout was developed to provide full two-dimensional elastograms of the liver in less than one second. The new sequence can be used as an MRE navigator to provide immediate feedback on wave penetration and data consistency for parameter optimization prior to running full multi-dimensional MRE. Moreover, the method can be used to rapidly track potential changes in liver stiffness such as those induced by respiration.Introduction
Liver fibrosis is a prevalent disease that can be monitored noninvasively with MR elastography (MRE) based on shear wave excitation and encoding. Compared with ultrasound elastography, MRE provides better 3D coverage of the liver with higher fidelity of anatomic detail, but suffers from longer scan time. Therefore, MRE examinations of the liver are usually spit into several breath-holds.[1] Alternatively, multifrequency MRE was proposed, which was applied under free breathing to avoid measurement times exceeding five minutes[2]. For an efficient MRE setup with optimal control over shear wave amplitudes and driver settings, it would be beneficial to perform short monofrequency MRE navigator scans before more time-consuming examinations with multifrequency or breath-hold MRE protocols. The aim of this work was to develop an MRE navigator that could either provide immediate feedback on wavefield amplitudes in-vivo or be used for time-resolved mapping of liver stiffness under altered physiological conditions.Methods
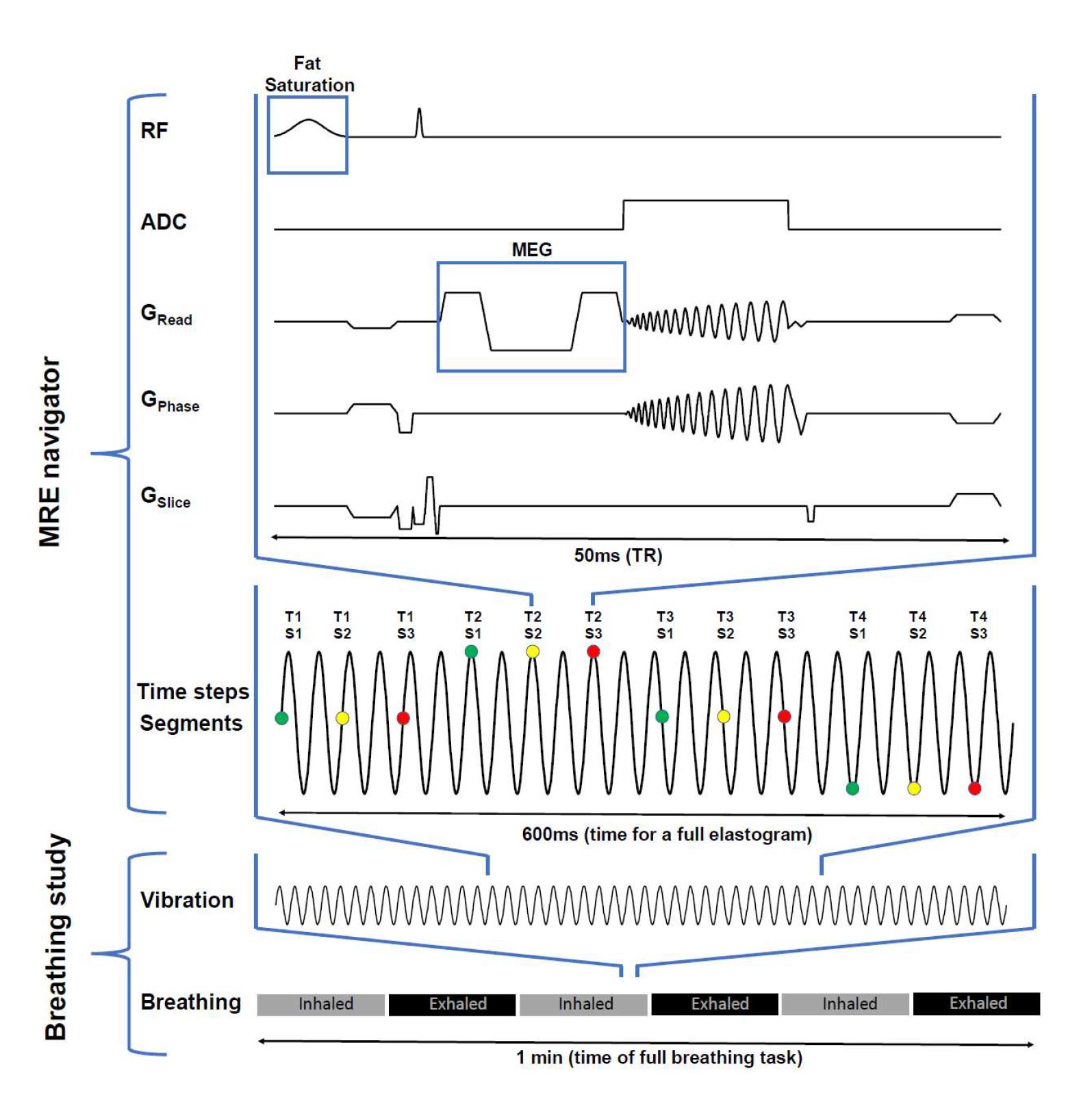
Ten healthy volunteers (40±13years) were investigated. Four compressed air drivers were attached onto the chest with a Velcro belt (two anterior, two posterior) and fed with a pulsed air flow of 40-Hz frequency. Experiments were performed in a 3-Tesla MRI scanner (MAGNETOM Lumina, Siemens, Germany) using a 12-channel receiver coil. Figure 1 shows the custom MRE navigator sequence based on a multi-shot, gradient-echo spiral sequence (FOV 360×360mm², 2.5×2.5×5.0mm³ voxel size, TR=50ms, TE=14ms, 6/3 Spiral Interleaves designed/played-out, PAT-factor 2). One field component along the readout direction and 4 instances over a vibration cycle were acquired. Total acquisition time was 600ms. Overall, two experiments were performed in each subject. First, the capability of the sequence as MRE navigator was tested in a transversal slice. The obtained MRE maps were compared with 2D spin-echo EPI MRE of 11 slices, three encoding directions and 8 time steps over a vibration cycle which took approximately 25 seconds. In a second experiment, series of MRE maps were acquired in a coronal slice orientation continuously for one minute to investigate whether liver stiffness changes with respiration. Therefore, the breathing state was altered from inspiration to expiration after every ten seconds following the oral instructions of the operator. Stiffness maps in terms of shear wave speed (SWS, in m/s) were reconstructed using the k-MDEV method[3]. For the second experiment, image registration was performed based on spatial normalization[4] to align the liver position within the 2D-image slice to the initial region of interest over the entire measurement time.Results
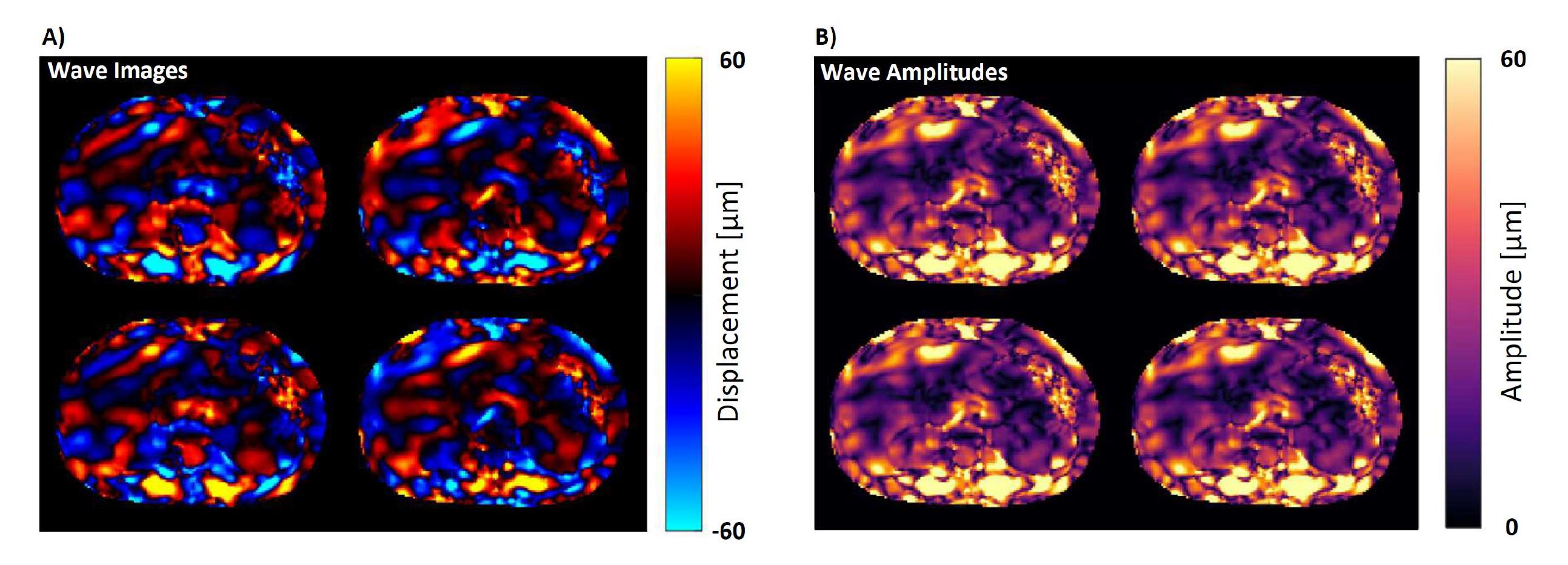
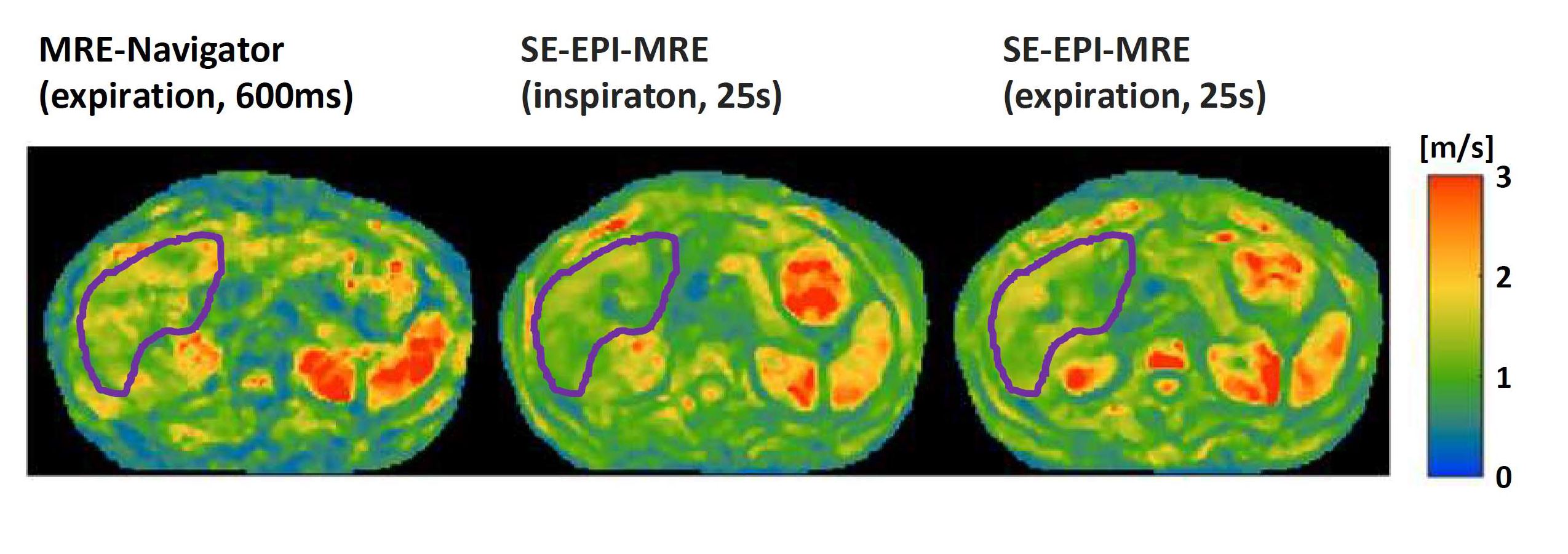
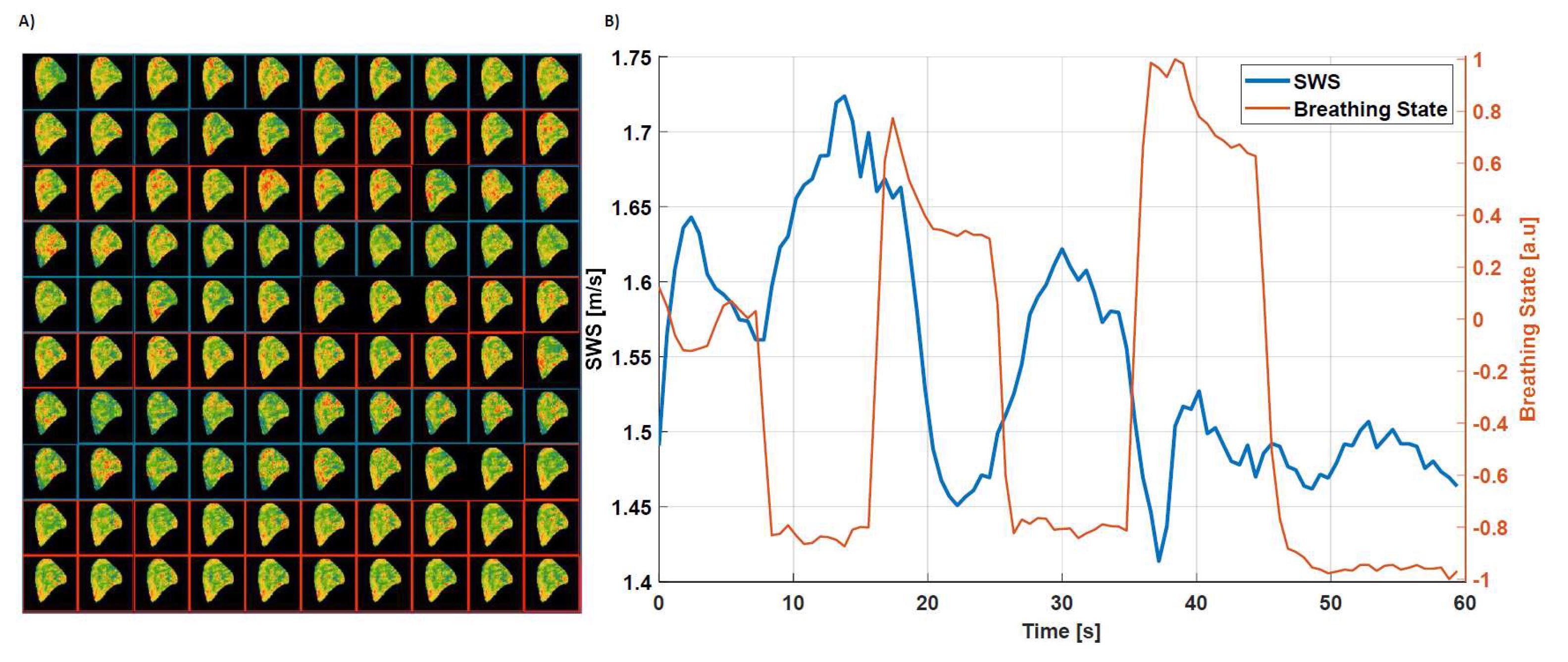
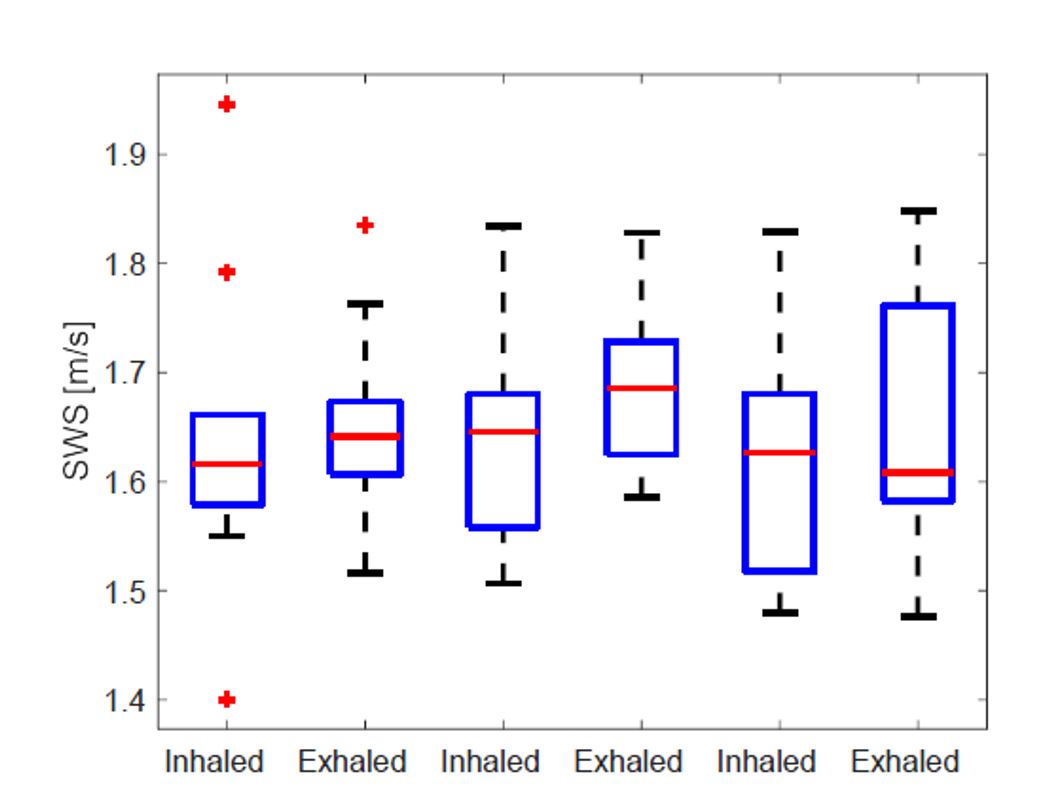
Figure 2 shows wave images and total wave amplitudes in a volunteer obtained by navigator MRE. Wave amplitudes were in the order of 60µm and showed shear waves within the entire field of view with indicating sufficient wave penetration of the abdomen. The attenuation of shear waves toward the center of the liver provides information about the viscosity of the tissue. Figure 3 shows transversal SWS maps in a representative subject obtained from 600ms-navigator MRE and 25s-EPI MRE in two respiration states. SWS values within the liver are slightly higher for the MRE navigator (1.40±0.46m/s) than for EPI-MRE (1.26±0.31m/s, p=0.042). There was no significant difference between liver stiffness measured by EPI-MRE in inspiration (1.15±0.27m/s) and expiration (1.26±0.31m/s, p=0.517). Figure 4 shows the variation of liver stiffness during alternating breathing states in one volunteer. The respiratory curve was generated from the displacement along the superior-inferior axis as obtained from the motion-correction. The group statistics in figure 5 showed no significant alteration of SWS with breathing, although some variation in SWS in synchrony with respiratory motion was observed in individual subjects.Discussion
This work presented a preliminary study using a novel MRE navigator based on a multi-shot, gradient-echo sequence with spiral readout. With an acquisition time of 600ms for full SWS maps of the abdomen, this sequence offers, to our knowledge, the fastest MRE method for liver studies to date. As shown in two single experiments, the method can be used to optimize the driver based on in-vivo wave amplitudes prior to lengthy higher-dimensional MRE acquisitions or to rapidly track potential changes in liver stiffness due to physiological changes such as geometry, blood flow, or abdominal pressures. Previous work has shown that liver stiffness decreases with increased abdominal pressure induced by the Valsalva maneuver, which is associated with a decrease in hepatic blood flow[5,6]. Similar effects, albeit to a lesser extent, may occur through respiration, which was indeed observed in some of our subjects. Therefore, expiration, when hepatic blood flow through the hepatic vein is at its maximum capacity, is the preferred breathing state for MRE studies. As a limitation, we observed a significant difference between navigator MRE and EPI-MRE, which deserves further investigations. We assume that reduction of field encoding to only one component (read-out) limits the stability of MRE against diffraction effects resulting in slightly higher values. In ongoing studies, we are testing the encoding of the thru-plane component as it is used in standard 2D-MRE of the liver[1].Conclusion
Navigator MRE for abdominal stiffness measurements in less than one second is feasible. This viable method can be used for rapid testing and parameter optimization of MRE driver hardware and post-processing pipelines, as well as for measuring potential stiffness variations due to respiratory-induced deformations of the liver.Acknowledgements
The authors gratefully acknowledge funding from the German Research Foundation (GRK2260, BIOQIC).References
[1] Venkatesh, S. K., Yin, M., & Ehman, R. L. (2013). Magnetic resonance elastography of liver: technique, analysis, and clinical applications. Journal of Magnetic Resonance Imaging, 37(3), 544-555.
[2] Shahryari, M., Meyer, T., Warmuth, C., Herthum, H., Bertalan, G., Tzschätzsch, H., ... & Sack, I. (2021). Reduction of breathing artifacts in multifrequency magnetic resonance elastography of the abdomen. Magnetic Resonance in Medicine, 85(4), 1962-1973.
[3] Tzschatzsch, H., Guo, J., Dittmann, F., Hirsch, S., Barnhill, E., Johrens, K., Braun, J. & Sack, I. (2016). Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal, 30, 1-10.
[4] Ashburner, J. (2009). Computational anatomy with the SPM software. Magnetic Resonance Imaging, 27(8), 1163-1174.
[5] Ipek‐Ugay, S., Tzschätzsch, H., Braun, J., Fischer, T., & Sack, I. (2017). Physiologic reduction of hepatic venous blood flow by the Valsalva maneuver decreases liver stiffness. Journal of Ultrasound in Medicine, 36(7), 1305-1311
[6] Meyer, T., Tzschätzsch, H., Wellge, B., Sack, I., Kröncke, T., & Martl, A. (2022). Valsalva Maneuver Decreases Liver and Spleen Stiffness Measured by Time-Harmonic Ultrasound Elastography. Frontiers in Bioengineering and Biotechnology, 10.
Figures