5141
A feasibility study of deep learning cardiac cine comparing image quality and volumetry with the conventional ASSET cine1Radiology, Keio University School of Medicine, Tokyo, Japan, 2Keio University Hospital, Tokyo, Japan, 3GE Healthcare Japan, Tokyo, Japan, 4GE Healthcare, Menlo Park, CA, United States
Synopsis
Keywords: Heart, Cardiovascular, Accelerated cine
Accelerated cardiac cine was obtained with deep learning reconstructed technique on ten patients (DL Cine). Three series of DL Cine with different parameters were acquired, including reduction factor (RF) of 12 under free breathing (FB), RF of 12 during one breathhold (R12) and RF = 9 dividing the left ventricular short axis into two slabs during each breathhold (R9). The two readers evaluate image quality (IQ) score and measure the cardiac functional parameters and compared them with the conventional ASSET cine. Although the IQ score was smaller than ones of the conventional cine, they are clinically acceptable. We found good correlations between volumetry on the conventional and DL cine.Background
The cardiac MRI study is time consuming due to the limitation of image acquisitions under the patients’ breathholds. Several techniques have been proposed to shorten exam time, and recently, the deep learning (DL) reconstruction technique has developed1-9,with undersampling cine technique10-12. The aim of this study is to compare the image quality and evaluate the interchangeability in the volumetry between these two techniques.Material and Methods
A total of ten patients (including four men) was enrolled in this study. This study was performed with written informed consent from all subjects under permission of institutional review board. In this group, there were various causes for planning cardiac MRI (CMR), including old myocardial infarction (2), hypertrophic cardiomyopathy (HCM, 2), arrythmia (2), LV dysfunction (2), as well as two of normal subjects. The mean age was 46.4 years old (range from 21 to 81), and average height, weight and BMI were 167.3 cm, 66,8 kg and 23.9, respectively. The mean beats per minute (bpm) was 67.7 (range from 52 to 87) during CMR examination. Steady-state free precession (SSFP)-based DL Cine image stacks in short axis of the left ventricle (LV) were obtained following the conventional cine in routine clinical studies on a 3T clinical scanner (Discovery MR750 3.0T, GE Healthcare, USA). Three series of DL Cine with different parameters were obtained, including A) reduction factor (RF) = 12 under free breathing (FB), B) RF=12 during one breathhold (R12), C) RF = 9 dividing the whole SX into two slabs during each breathhold (R9). Slice thickness was 8 mm with gapless and image matrices were 224x224, excluding FB DL cine as 140x140. Two observers with 3 and 15 years of experience in CMR independently evaluated the image quality using 5-point scale (1=poot, 2=acceptable, 3=fair, 4=good, 5=excellent), in terms of the contrast between the cavity and myocardium, signal homogeneity, blurring, clarity and general imaging quality. The cine image data was transferred to an independent post processing software (Ziostation 2, Tokyo, Japan). Two observers independently corrected the semi-automatic segmentation of the outer and inner contours of LV wall, and cardiac function was calculated in values of the LV end-diastolic volume (LVEDV), stroke volume (SV), ejection fraction (EF), and LV mass (Mass). The averaged values derived from two readers were used for the comparison. The relationship between variables was evaluated with Spearman’s correlation coefficients. Differences between two techniques were also evaluated using Bland-Altman plots, expressing mean difference and 1.96 x standard deviation of the difference.Results
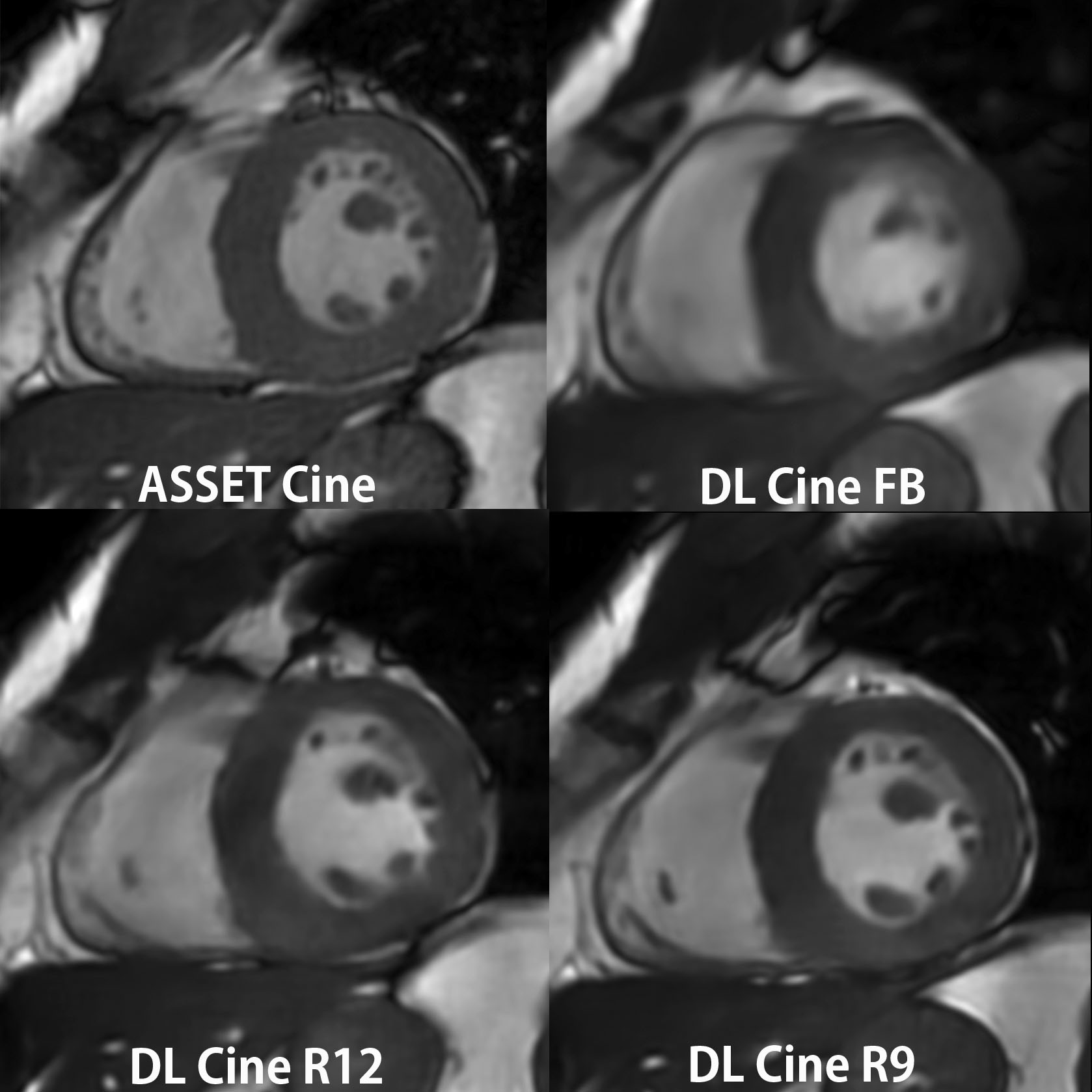
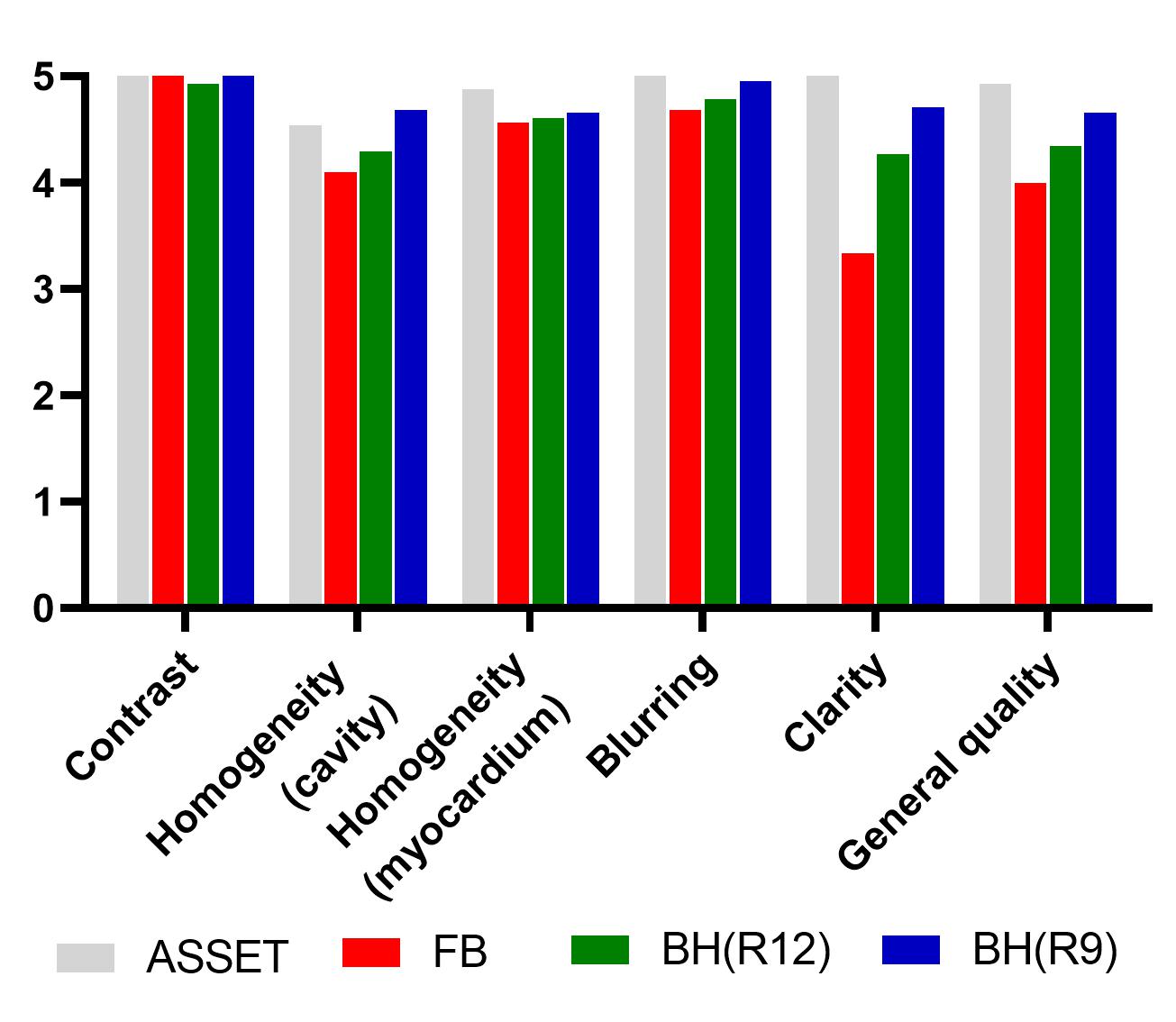
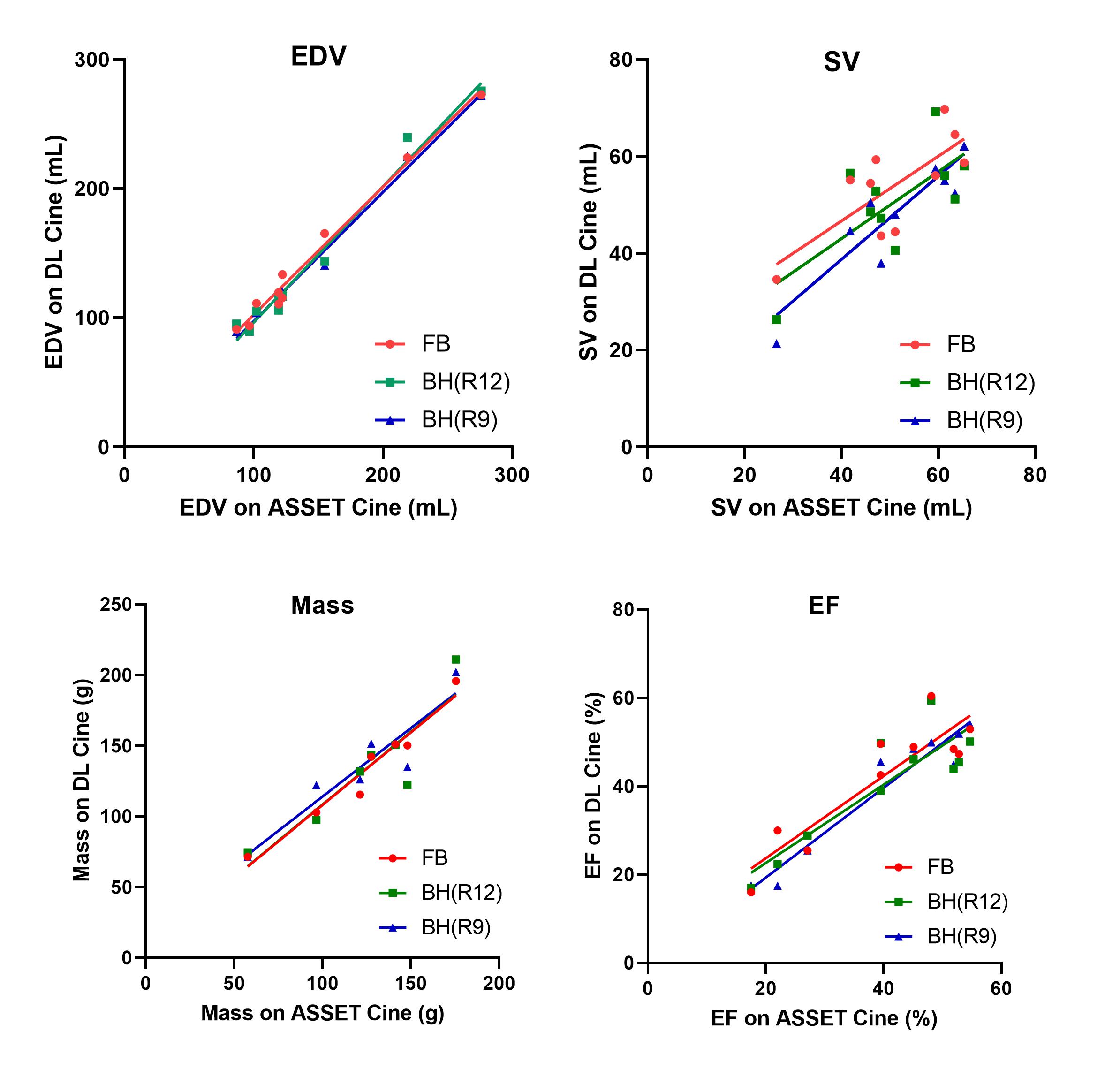
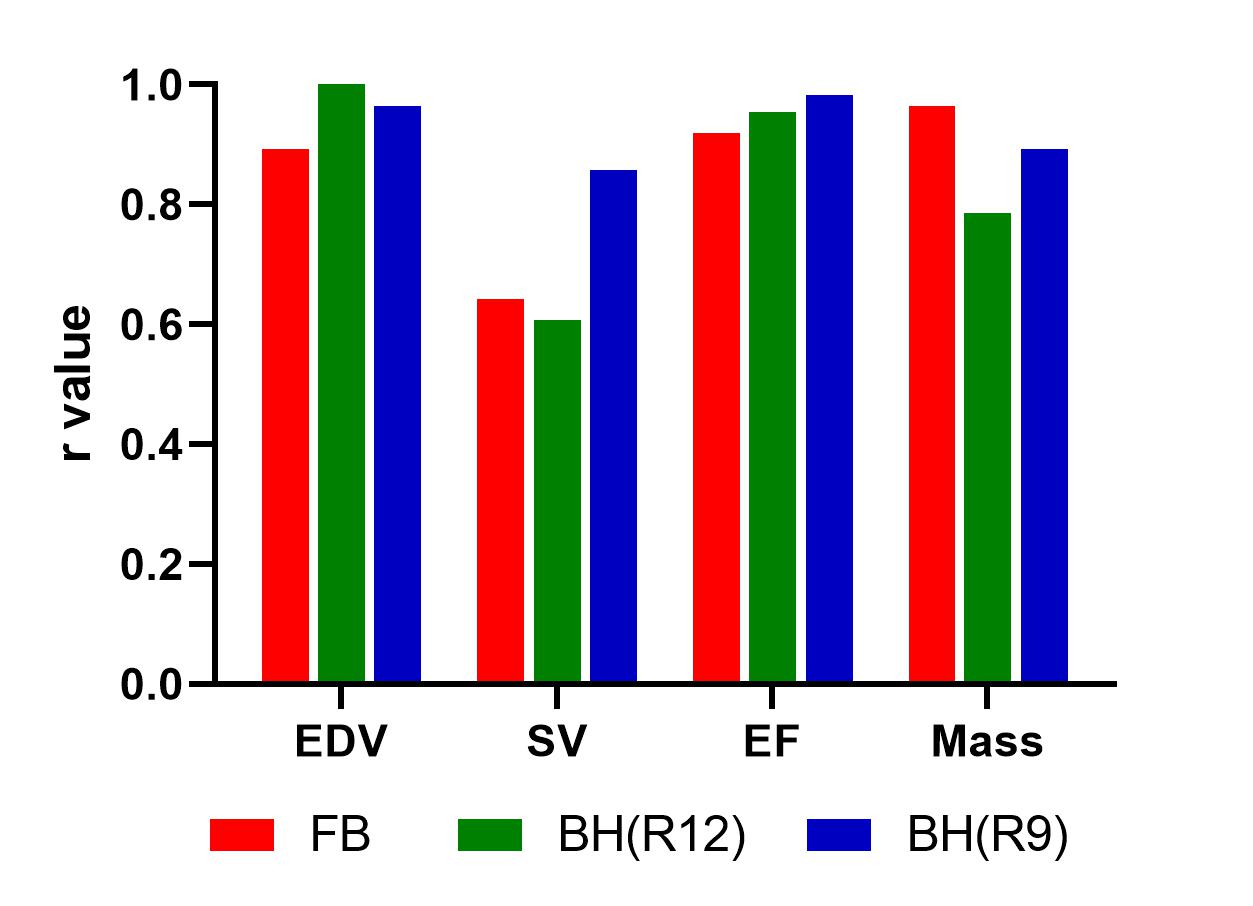
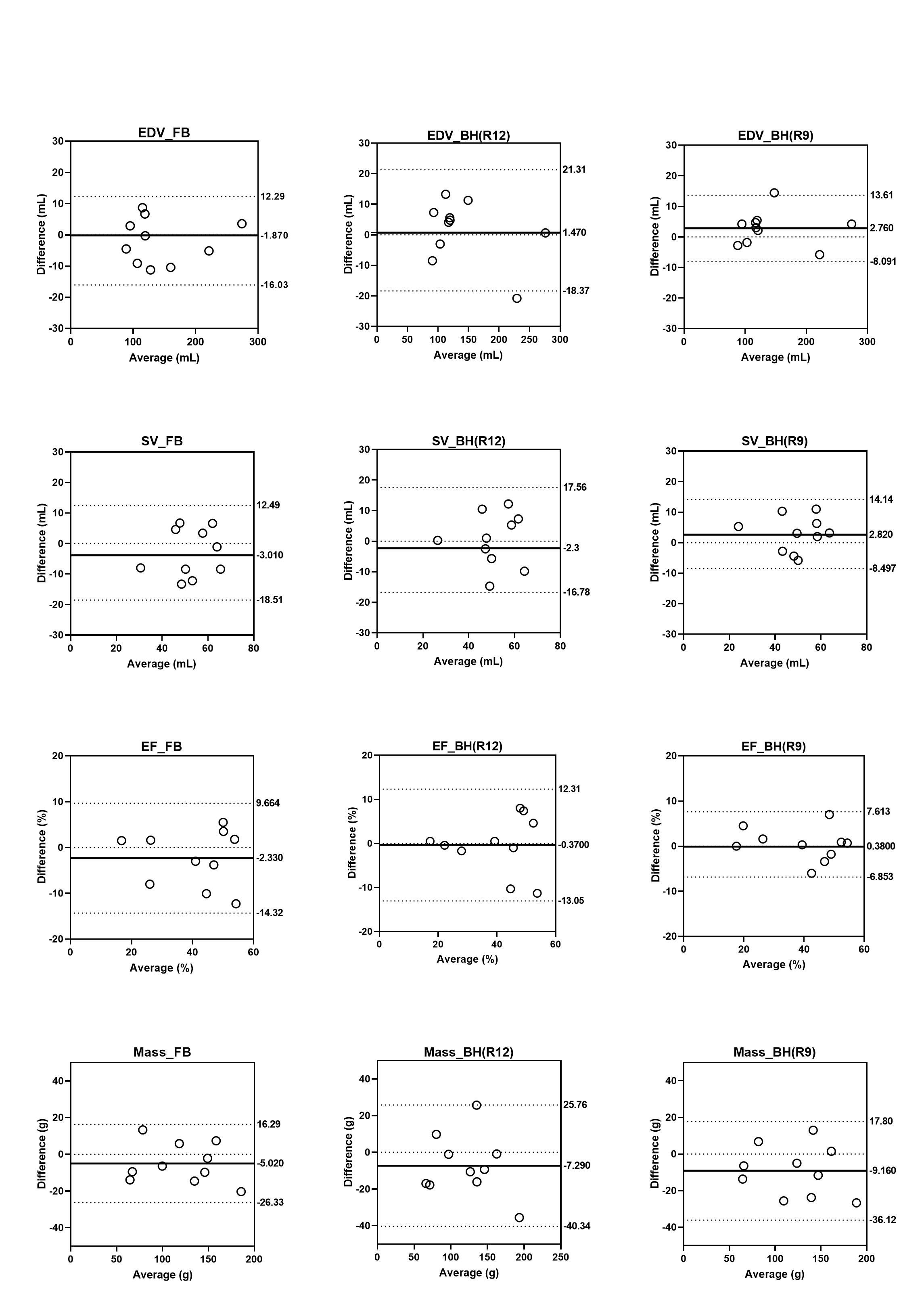
The representative images are demonstrated in Figure 1. The general imaging quality scores of DL Cine were 4.0 in FB, 4.3 in R12 and 4.7 in R9, which were lower than the score of 4.9 in ASSET cine. All scores were more than 4, excluding the blurring score of FB (3.3) (Fig 2). On the scatter plots between volumetric results from ASSET and DL Cines, strong correlations (r > 0.8) were found, excluding SV in FB and R12 (Fig 3). Although comparison of values measured on ASSET and DL Cines demonstrated substantial difference from zero in Mass (-5.0 g [-26.3,16.3], -7.3 g [-40.3, 27.8], -9.2 g [-36.1,17.8] on FB, R12 and R9, respectively). There were intermediate differences from zero in SV (-2.3 mL [-14.3,9.7]) and EF (-3.0% [-18.5,12.5]) on FB. Differences in other comparisons were not significant (Fig 4).Discussion
The image quality and the results of volumetry were compared between the conventional ASSET cine and DL Cine. The image quality of DL Cine was clinically acceptable. The blurring was obvious and intermediate difference in volumetry was found on FB, therefore, the DL cine was recommended to be used under breathhold when the patients can tolerate repeating breathholds. FB DL Cine is also feasible for obtaining cine image which has a clinical value to evaluate the morphology and wall motion. The potential difference is assumed between LV volumes with and without breathhold, which may affect the concordance of volumetry between BH and FB cine; however, it cannot be assessed because FB conventional cine is not Accelerated cine using compressed sensing (CS) technique has been reported in previous investigations13-15, which found significant correlations between values on the volumetry of the left and right ventricles. DL Cine might be comparable to accelerated CS-cine.Conclusion
Although substantial difference was found in LV mass measurements, cardiac cine using DL Cine (BH R9) is a promising method for evaluating cardiac function in two breath holds. In addition, free-breathing technique is also acceptable for cine study for patients with insufficient breathhold.Acknowledgements
No acknowledgement found.References
1. Barkhausen J, Ruehm SG, Goyen M et al. Radiology 2001;219:264–9.
2. Moon JC, Lorenz CH, Francis JM, et al. Radiology 2002;223:789–97.
3. Tsao J, Boesiger P, Pruessmann KP. Magn Reson Med 2003; 50:1031–42.
4. Lai P, Brau AC, Beatty PJ,et al. Proc Intl Soc Mag Reason Med 2009;17:767.
5. Lai P, Alley MT, Vasanawala SS, et al. Proc Intl Soc Mag Reson Med 2011;19:3378.
6. Jeong D, Schiebler ML, Lai P. et al. Int J Cardiovasc Imaging 2015;31:851-7.
7. Okuda S, Yamada Y, Tanimoto A. et al: Magn Reson Imaging. 2015;33:911-7.
8. Vial J, Bouzerar R, Pichois R. et al. AJR Am J Roentgenol 2020;215:807-17.
9. Orii M, Sugawara T, Takagi H. et al. Br J Radiol. 2021;94:20201249.
10. Sandino CM, Lai P, Vasanawala SS. Et al. Magn Reson Med 2021;85:152-67.
11. Zucker EJ, Sandino CM, Kino A. et al. Radiology 2021;300:539-48.
12. Morales MA, Assana S, Cai X. et al. J Cardiovasc Magn Reason 2022;24:47.
13. Kido T, Kido T, Nakamura M. et al. J Cardiovasc Magn Reason 2016;18:50.
14. Kido T, Kido T, Nakamura M. et al. Circ J. 2017;81:1463-8.
15. Kido T. Hirai K, Ogawa R. et al. J Cardiovasc Magn Reason 2021;23:10.
Figures