5139
Evaluation of image quality and global cardiac function for deep learning accelerated cardiac Cine
Xucheng Zhu1, Suryanarayanan Kaushik2, Frandics Chan3, Melany Atkins4, Prashant Nagpal 5, Reed Busse2, and Martin Janich6
1GE Healthcare, Menlo Park, CA, United States, 2GE Healthcare, Waukesha, WI, United States, 3Radiology, Stanford University, Palo Alto, CA, United States, 4Radiological Consultants, Inova Fairfax Hospital, Fairfax, VA, United States, 5Radiology, University of Wisconsin–Madison, Madison, WI, United States, 6GE Healthcare, Munich, Germany
1GE Healthcare, Menlo Park, CA, United States, 2GE Healthcare, Waukesha, WI, United States, 3Radiology, Stanford University, Palo Alto, CA, United States, 4Radiological Consultants, Inova Fairfax Hospital, Fairfax, VA, United States, 5Radiology, University of Wisconsin–Madison, Madison, WI, United States, 6GE Healthcare, Munich, Germany
Synopsis
Keywords: Heart, Image Reconstruction, Deep learning, reconstruction
Cardiac bSSFP Cine is widely used clinically; however, it is time consuming and requires multiple breath-holds. Deep learning-based accelerated Cine (DLCine) is a novel technique combining accelerated variable density sampling and deep learning regularized reconstruction that allows much higher acceleration compared to conventional Cine with parallel imaging. The purpose of this work was to compare image quality and global cardiac function utilizing DLCine versus conventional Cine by three expert readers. The results demonstrate that DLCine can be used to reduce the scan time while maintaining image quality and providing accurate global cardiac function measurement.Introduction
Cardiac bSSFP Cine is widely used clinically for visualizing anatomic structure and quantifying cardiac function. bSSFP Cine is the gold standard for assessing cardiac function. However, conventional Cine utilizing parallel imaging acceleration requires long breath-holds to complete a single slice acquisition, and typically more than 10 breath-holds are necessary to cover the whole ventricle for cardiac function measurement.A newly developed method, Deep Learning Cine (DLCine), uses variable density sampling and a deep learning based regularized reconstruction. This method allows much higher acceleration compared to conventional Cine with parallel imaging, and consequently, reduces the total cardiac MR scan time. Additionally, this method improves patient comfort by reducing the duration and number of breath-holds needed.
In this work, three expert readers evaluated DLCine and conventional Cine, assessing qualitative image quality (IQ) and quantitative global cardiac function (CF).
Methods
DLCine implementationDLCine is based on retrospectively cardiac gated 2D bSSFP Cine, combining Cartesian variable density undersampling acquisition scheme [1] and a deep learning-based reconstruction. Deep learning reconstruction uses an unrolled neural network including both data consistency updates and CNN based regularizers [2, 3]. The model uses 12 unrolls and includes 6.6M trainable parameters. The model is trained with 6480 images, an l1-loss function, and Adam optimizer.
Data acquisition
All in vivo data for the reader studies were collected with IRBs approval and de-identified. Data was acquired on 1.5T and 3.0T wide-bore GE Healthcare MR scanners. Image quality evaluation data included 25 patients and 7 healthy volunteers, and CF evaluation included 12 patients and 7 healthy volunteers. ASSET Cine (acceleration up to 2.0) and DLCine (acceleration up to 12.0) images were acquired during breath holding with comparable settings: standard geometric orientation, FOV, temporal resolution, slice coverage, and post-processing filters. ASSET Cine image series were acquired within 6-10 heart beats scan time (6-10RR), and DLCine were acquired with three different RR settings (1RR, 3RR, and 6RR).
For the image quality evaluation, short-axis (SAX), long-axis (LAX, including 2-, 3-, and 4-chamber), and aortic valve (AoV) series were acquired. Each series included one or more 2D slices covering the complete cardiac cycle. For global cardiac function assessment, SAX stack of slices covering whole left ventricle (LV) were acquired, with corresponding LAX view for localization of the mitral valve.
Data processing
Both ASSET Cine and DLCine series were randomized and reassigned with new identification numbers before being sent to the readers for blinded evaluation.
Reader study design
Three board-certified radiologists, selected for their expertise in Cardiac MR, conducted evaluations for cases in this study. Each radiologist was asked to rate each Cine images series on a likert scale of 1-5 (Table 1-I). Readers rated images individually and not in a paired fashion. In addition, each radiologist was asked to use a commercially available CMR post-processing software (Circle cvi42, NeoSoft suiteHEART, and Medis QMass) to measure global cardiac function based on each Cine series (metrics summarized in Table 1-II).
Results
Representative image examples, ASSET Cine and corresponding 1RR, 3RR, and 6RR DLCine in different cardiac views, are shown in Figure 2. IQ evaluation Likert scales ratings distribution is summarized in Table 3-I and the mean and standard deviation of the average ratings are summarized in Table 3-II. ASSET Cine obtained 98.5% of its ratings in the diagnostically acceptable range, while DLCine obtained 94.5% of its ratings in the diagnostically acceptable range. For the SAX and AoV views, the 6RR DLCine got a higher averaged likert scale rating than the ASSET Cine scans. We also compared the relative scan time differences in Table 3-III. All DLCine categories show significant scan time reduction of 30-80% compared to ASSET Cine. Global cardiac function evaluation Table 4 shows coefficient of variability for the CF measurements. Variability between ASSET Cine and DL Cine was comparable or smaller compared to intra-method variability across all CF metrics. In addition, Figure 5 shows Bland-Altman plots for the LVEF (%) for each DLCine category using the number from ASSET Cine as a reference. LVEF quantification with DLCine demonstrated no bias compared to ASSET Cine.Conclusion
In this work, we evaluated image quality and cardiac function measurements for DLCine and ASSET Cine. The results demonstrate that (1) DLCine can shorten acquisition scan time and preserve image quality, (2) DLCine can largely shorten scan time while maintaining diagnostic image quality, and (3) global cardiac function measurements based on DLCine are comparable to ASSET Cine.Acknowledgements
No acknowledgement found.References
[1] Lai, Peng, and Anja Brau. "Improving cardiac cine MRI on 3T using 2D kt accelerated auto-calibrating parallel imaging." Journal of Cardiovascular Magnetic Resonance 16.1 (2014): 1-2.
[2] Sandino, Christopher M., et al. "Accelerating cardiac cine MRI using a deep learning‐based ESPIRiT reconstruction." Magnetic Resonance in Medicine (2020).
[3] Zucker, Evan J., et al. "Free-breathing Accelerated Cardiac MRI Using Deep Learning: Validation in Children and Young Adults." Radiology (2021): 202624.
Figures
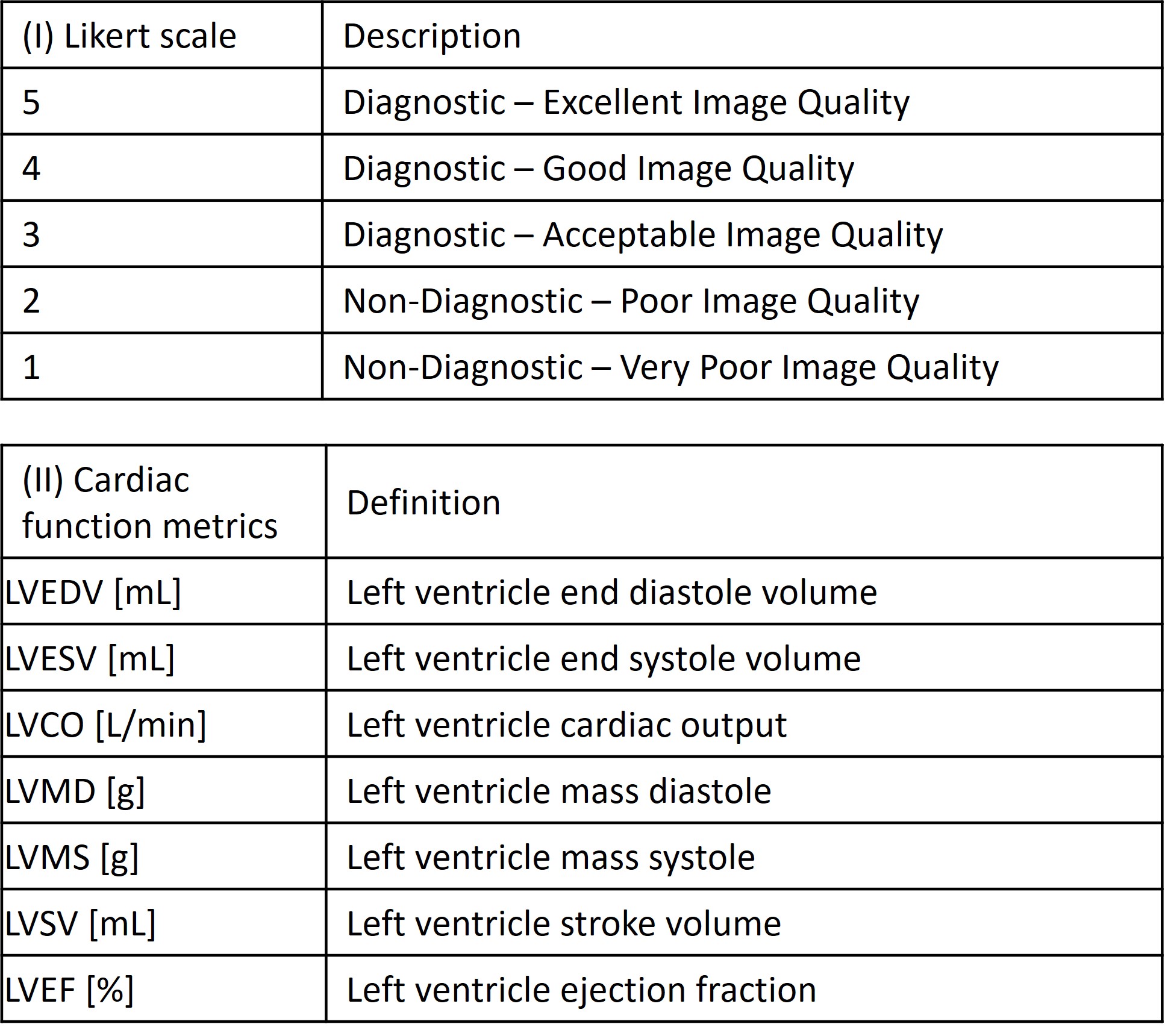
Table 1
Reader study criteria. Likert scale descriptions for image quality study are
summarized in chart (I), scale at 3 or above represents diagnostic image
quality. Global cardiac function metrics for the cardiac function measurement
study are listed in chart (II), include LVEDV, LVESV, LVCO, LVMD, LVMS, LVSV,
and LVEF.
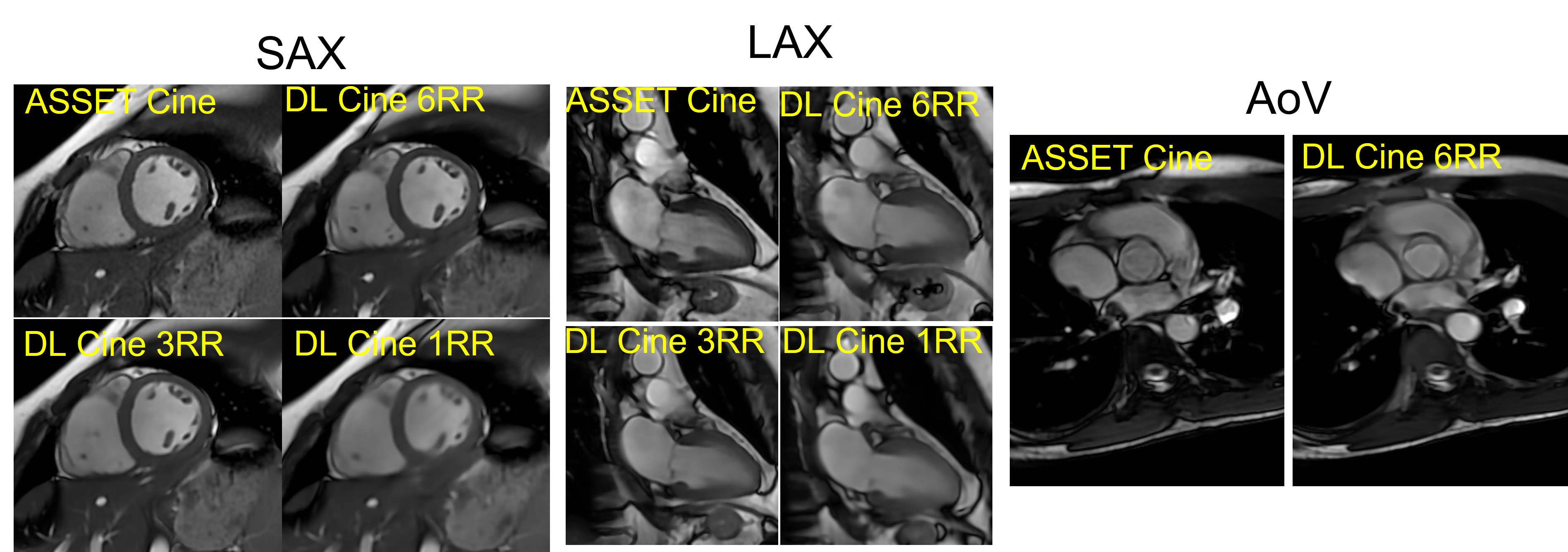
Figure 2
Example images for reader study. Examples of the Cine images used on the reader
study are plotted, include short axis (SAX), long axis (LAX), and aortic valve
(AoV) view.
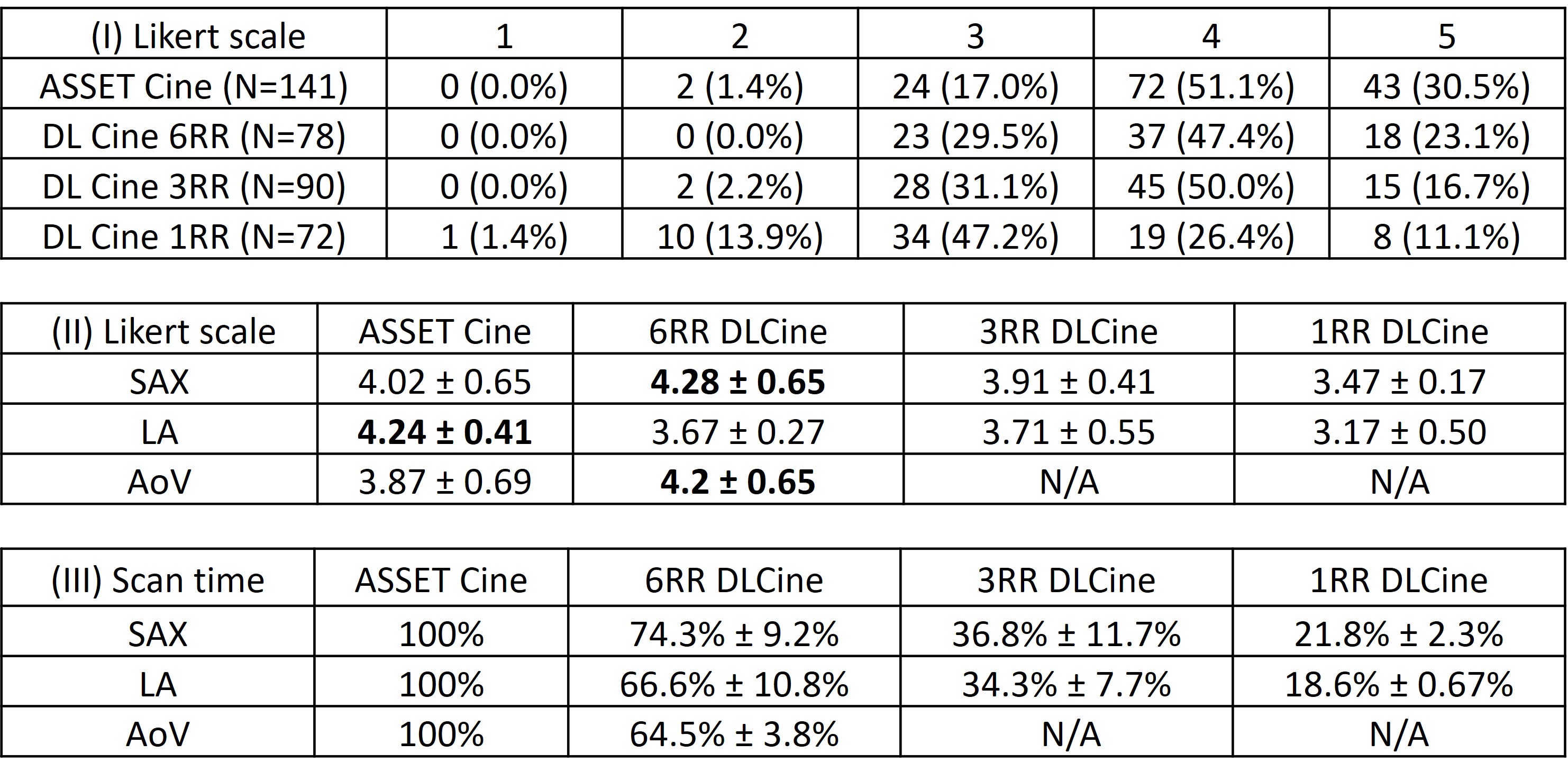
Table 3 IQ
study results. (I) presents the distribution of likert scales from all three
readers, ASSET Cine obtained 98.5% of its ratings in the diagnostically
acceptable range, while DLCine 6RR
obtained 100% of its ratings in the diagnostically acceptable range and DLCine
3RR obtained 97.7% of its ratings in the diagnostically acceptable range. (II)
shows the mean and standard deviation of the likert scales in different cardiac
view. (III) shows the relative scan time ratio compared to corresponding ASSET
Cine scans.
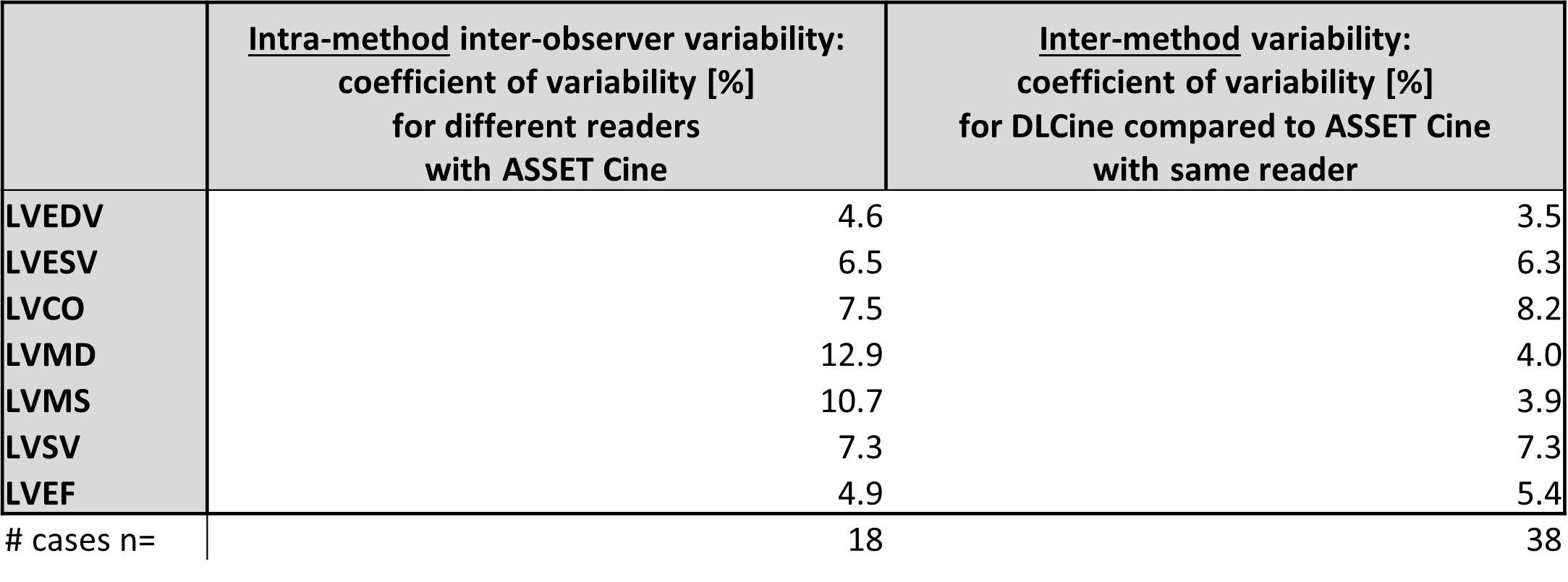
Table 4 Global cardiac function measurement variability summary. Coefficients
of variability (CV) of CF measurements based on ASSET Cine from different
readers and CV of DLCine compared to ASSET Cine from the same reader are
reported.
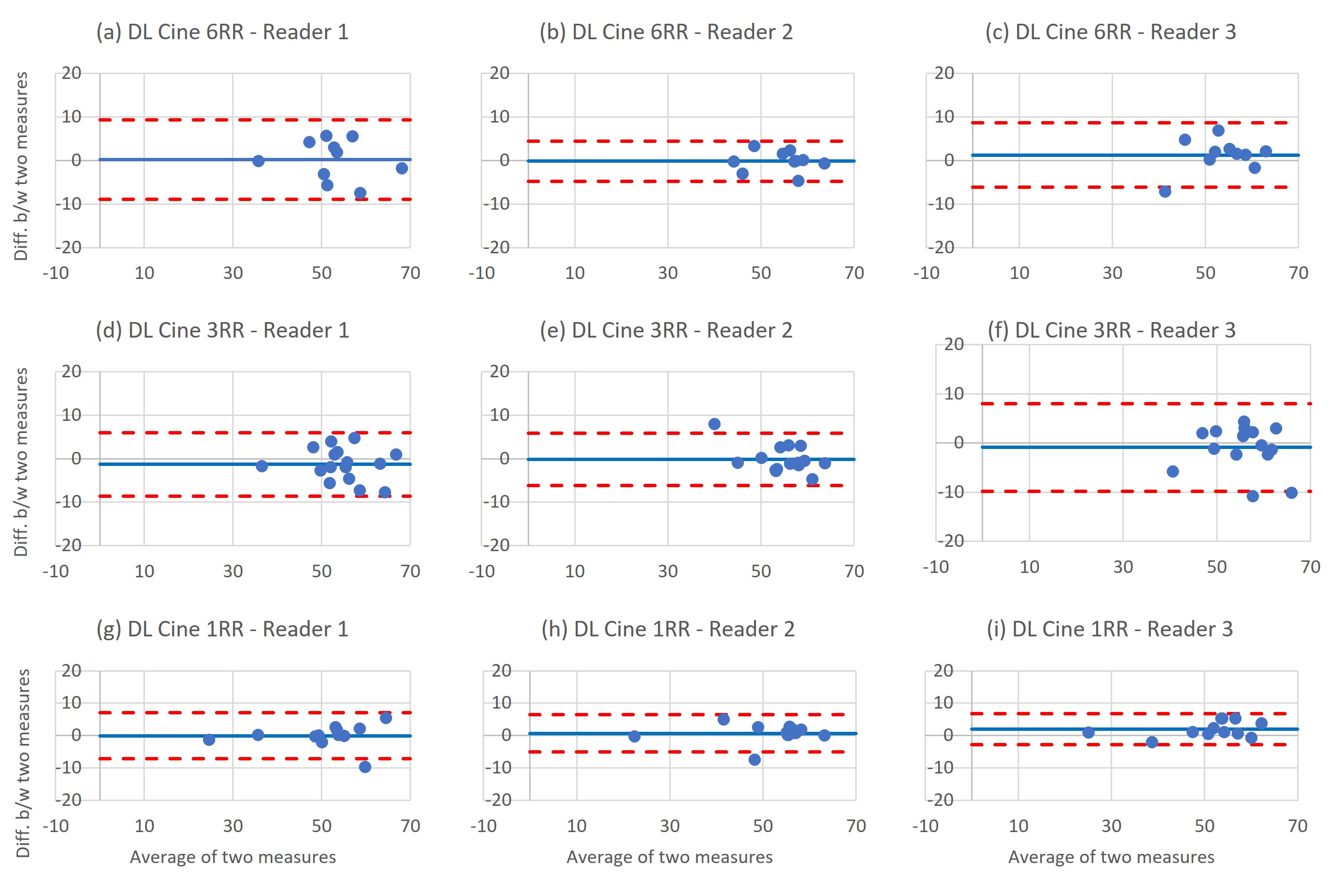
Figure 5
Bland-Altman plots for the LVEF (%) for each DLCine category and across
readers, using the number from ASSET Cine as a reference.
DOI: https://doi.org/10.58530/2023/5139