5138
Cine MRI reconstructed from 3T contrast-enhanced free-running 5D coronary MRA: comparison to standard 2D cine MRI
Haruno Ito1, Masaki Ishida1, Masafumi Takafuji1, Shinichi Takase1, Yoshiaki Komori2, Davide Piccini3,4, Jessica A.M. Bastiaansen4, Jérôme Yerly4,5, Matthias Stuber4,5, and Hajime Sakuma1
1Radiology, Mie University Hospital, Tsu, Mie, Japan, 2Siemens Healthcare K.K., Tokyo, Japan, 3Advanced clinical imaging technology, Siemens Healthineers International AG, Lausanne, Switzerland, 4Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 5CIBM Center for Biomedical Imaging, Lausanne, Switzerland
1Radiology, Mie University Hospital, Tsu, Mie, Japan, 2Siemens Healthcare K.K., Tokyo, Japan, 3Advanced clinical imaging technology, Siemens Healthineers International AG, Lausanne, Switzerland, 4Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 5CIBM Center for Biomedical Imaging, Lausanne, Switzerland
Synopsis
Keywords: Heart, Heart, Cine MRI
Cine MRI derived from 3T contrast-enhanced free-running 5D whole-heart coronary MRA (free-running cine MRI) was compared with standard 2D cine MRI in 30 patients with suspected CAD. In a selected patient, temporal width was optimized to 50 ms. Then, in the remaining 29 patients, free-running cine MRI provided good agreement in LV volume and function quantification with standard 2D cine MRI with a good inter-observer reproducibility. The results suggest that free-running cine MRI allows for a shorter scan protocol by skipping the standard 2D cine MRI.Introduction
Free-running 5D whole-heart coronary MRA is a free-breathing and non-electrocardiogram-triggered that can reduce scanning complexity by removing the need for specific slice orientations, respiratory gating, or cardiac triggering. This novel technique is based on compressed sensing (CS) for the reconstruction of highly under-sampled multidimensional datasets, allowing for the reconstruction of 5D (x-y-z-cardiac-respiratory) whole-heart coronary MRA1. Recent studies demonstrated that free-running 5D whole-heart coronary MRA can be performed using a bSSFP sequences without contrast injection at 1.5T2 and with a GRE sequences with slow infusion of gadolinium contrast medium at 3T3. An advanced CS reconstruction of the free-running dataset provides motion-resolved whole-heart images for the entire cardiac and respiratory dimension1. Typically, only one or two cardiac and respiratory bins are used for evaluating coronary MRA, whereas the rest of the images are discarded regardless of the motion information they contain. However, if motion-resolved images reconstructed along cardiac dimension can be utilized from the same dataset, total scan time can be reduced by skipping standard 2D cine MRI. Therefore, we sought to compare cine MRI reformatted from the 3T contrast-enhanced 5D free-running whole-heart coronary MRA dataset (free-running cine MRI), with standard breath-hold, ECG-gated 2D cine MRI for validation of LV volume and function quantification.Methods
Contrast-enhanced free-running 5D whole-heart coronary MRA and standard 2D short-axis cine MRI was performed at 3T (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) in 30 patients with suspected CAD. The research free-running 5D whole-heart MRA was acquired during slow infusion of gadobutrol (0.1mmol/kg) incorporating a prototype non-interrupted fully self-gated 3D golden-angle radial spoiled GRE sequence and LIBRE water excitation4 (TR/ TE= 3.93/2.19 ms, flip angle=15°, receiver bandwidth= 868 Hz/px, FOV= 220x220x220 mm3, readout matrix= 192, isotropic spatial resolution= 1.15x1.15x1.15 mm3, number of segments= 22, radial lines=126478, constant scan time= 8 min 17s.) The readouts were sorted into non-overlapping cardiac bins with a temporal width ranging from 20 to 100 ms with 10 ms increments, and into four non-overlapping respiratory bins. The binned k-space was reconstructed into motion-resolved 5D images by CS. On the end-expiratory bin, short-axis cine images were reformatted matching the slice thickness and orientation with the standard 2D short-axis cine MRI. 2D short-axis cine MR images covering the entire LV were acquired using bSSFP sequence (TR/ TE= 20.5/1.13 ms, flip angle=40°, receiver bandwidth= 1603 Hz/px, FOV= 360x270 mm2, readout matrix= 208x139, reconstructed spatial resolution= 0.87x0.87 mm2, slice thickness = 10 mm, slice gap= 0 mm, compressed sensing acceleration factor= 7.1, cardiac phase= 25). Firstly, in a selected patient, 5 radiologists traced standard 2D cine images and free-running cine images of each temporal width independently and obtained end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), EF, and LV mass to determine the optimal temporal width for free-running cine images. Then, 2 radiologists independently traced both cine datasets in the remaining 29 patients. Linear regression and Bland-Altman analyses and coefficients of variation (CV) were obtained to assess the correlation and agreement between these LV measurements and to evaluate inter-observer reproducibility in free-running cine MRI. CV was defined as the standard deviation of the differences divided by the mean x100 (%).Results
Representative sets of free-running cine and standard 2D cine MRI are shown in Figure 1. Comparison of EDV, ESV, SV, EF, and LV mass between free running cine MRI with different temporal resolution and 2D cine MRI is shown in Figure 2. Temporal resolution of 50 ms was selected as optimal for free-running cine MRI since each value of LV parameters were closest to those determined by standard 2D cine MRI. There were no significant differences in SV and LV mass between free-running cine MRI and standard 2D cine MRI (Figure 3). Compared to standard 2D cine MRI, however, a small but significant overestimation of EDV and ESV and underestimation of EF was noted on free-running cine MRI. Nevertheless, there was good agreement between the 2 methods for all measurements on linear regression analysis (Figure 4). On Bland-Altman analysis, the mean differences and CV in LV measurements between standard 2D cine and free-running cine MRI were as follows: EDV, -5.6mL (95% CI: −21.1 to 9.7mL) and 5.1% ; ESV, -5.6mL (95% CI: −18.7 to 7.4mL) and 8.8%; SV, −0.1mL (95% CI: −10.0 to 9.9mL) and 6.4%; EF, 2.0% (95% CI: −3.9 to 7.9%) and 5.6%; and LV mass, 0.07g (95% CI: −.27.3 to 27.5g) and 17.8%, respectively (Figure 5). The inter-observer reproducibility for free-running cine MRI measurements was good with CV of 5.3% for EDV, 8.3% for ESV, 9.3% for SV, 6.6% for EF, and 13.9% for LV mass.Discussion and Conclusion
Using the optimal temporal widths of 50ms to resolve cardiac motion, free-running cine MRI derived from 3T contrast-enhanced free-running 5D whole-heart coronary MRA dataset provides good agreement in LV volume and function quantification with standard 2D cine MRI, despite small overestimation of EDV, ESV and small underestimation of EF with a good inter-observer reproducibility. The results in the current study suggest that free-running cine MRI allows for significant shortening of the scan protocol by skipping the standard 2D cine MRI in patients with suspected CAD who needs the assessment of coronary stenosis.Acknowledgements
No acknowledgement found.References
1. Di Sopra L, et al. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. MRM. 2019;82:2118-2132.
2. Masala N, et al. Free-running 5D coronary MR angiography at 1.5T using LIBRE water excitation pulses. Magn Reson Med. 2020;84:1470- 1485.
3. Ishida M, et al. Development of an optimal protocol for contrast-enhanced free-running 5D wholeheart coronary MRA at 3T. Magn Reson Med Sci. Revision.
4. Bastiaansen JAM, t al. Noncontrast free-breathing respiratory self-navigated coronary artery cardiovascular magnetic resonance angiography at 3 T using lipid insensitive binomial off-resonant excitation (LIBRE). J Cardiovasc Magn Reson. 2019;21:38.
Figures
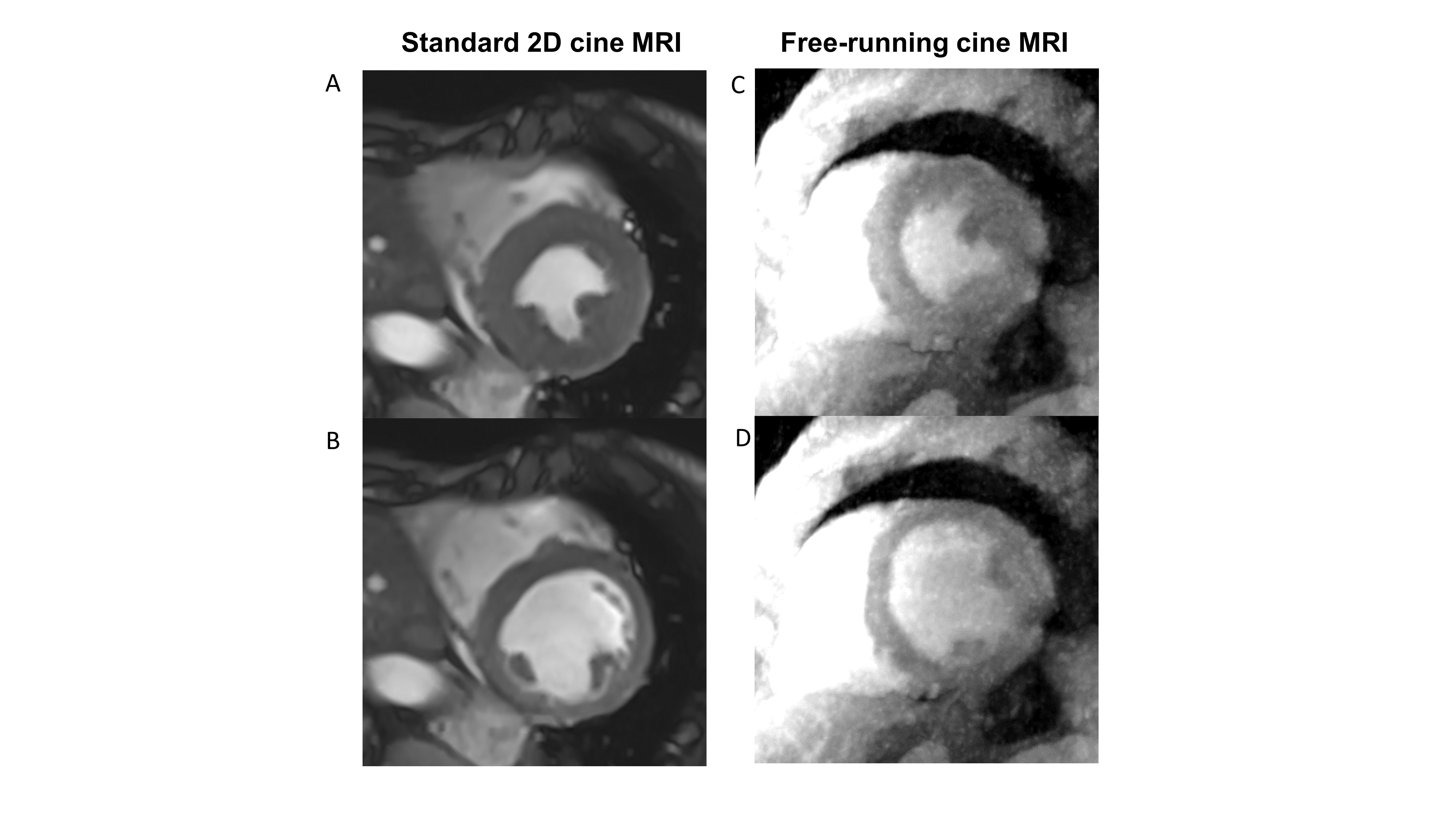
Figure 1. Representative standard 2D cine MRI (A, B), and
free-running cine MRI reconstructed from the 3T contrast-enhanced 5D
free-running whole-heart coronary MRA dataset (C, D) of a 82-year old male with
suspected coronary artery disease. End-diastolic (A, C) and end-systolic (B, D)
short-axis MR images of mid left ventricular slice
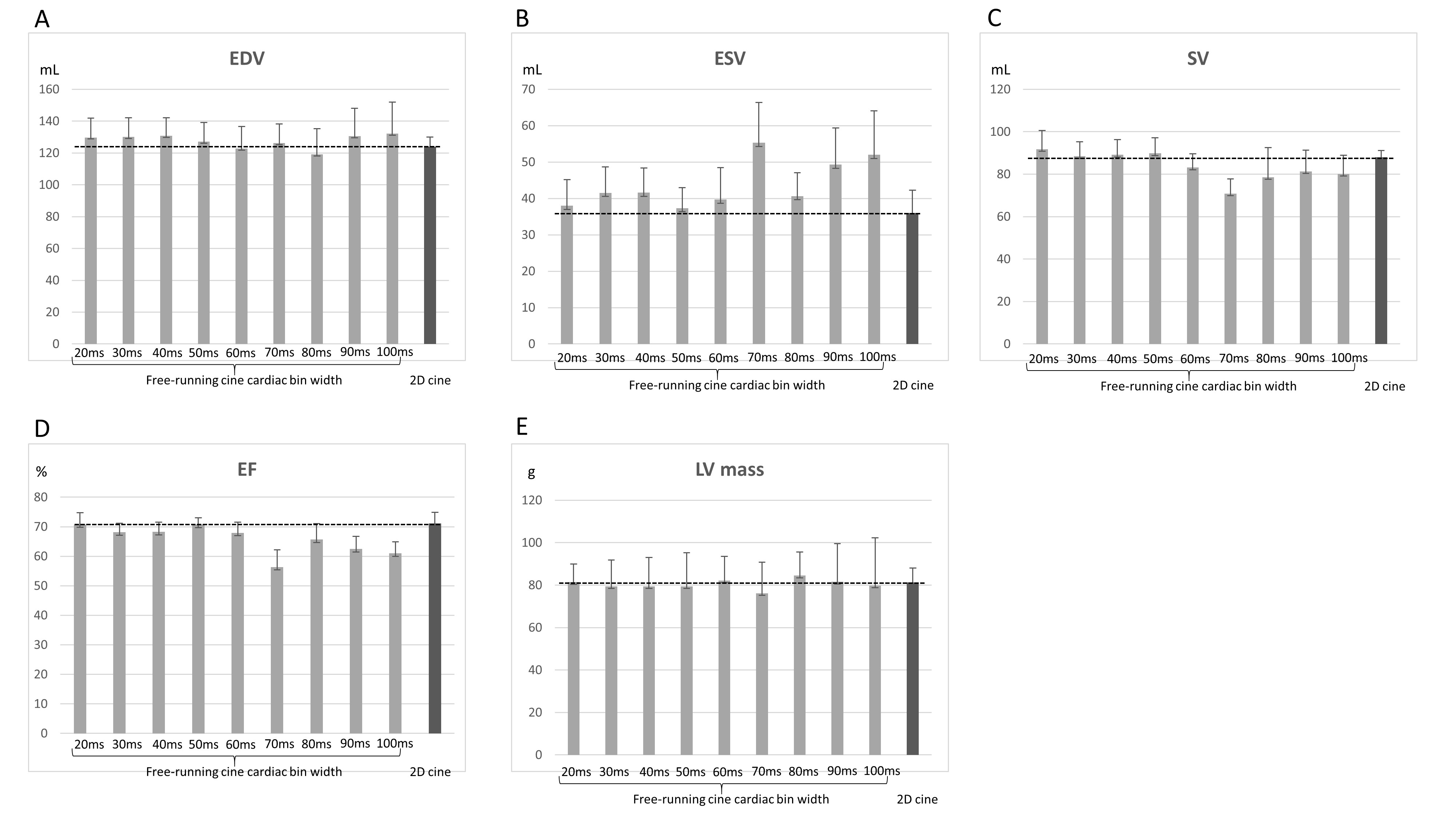
Comparison of EDV (A), ESV (B), SV (C), EF (D), and LV
mass (E) between 2D cine MRI (dark bar) and free running cine MRI with temporal
resolution ranging from 20 to 100 ms with 10 ms increments (gray bars). Each
bar indicates the mean ± standard deviation of measured values by 5 independent
radiologists.
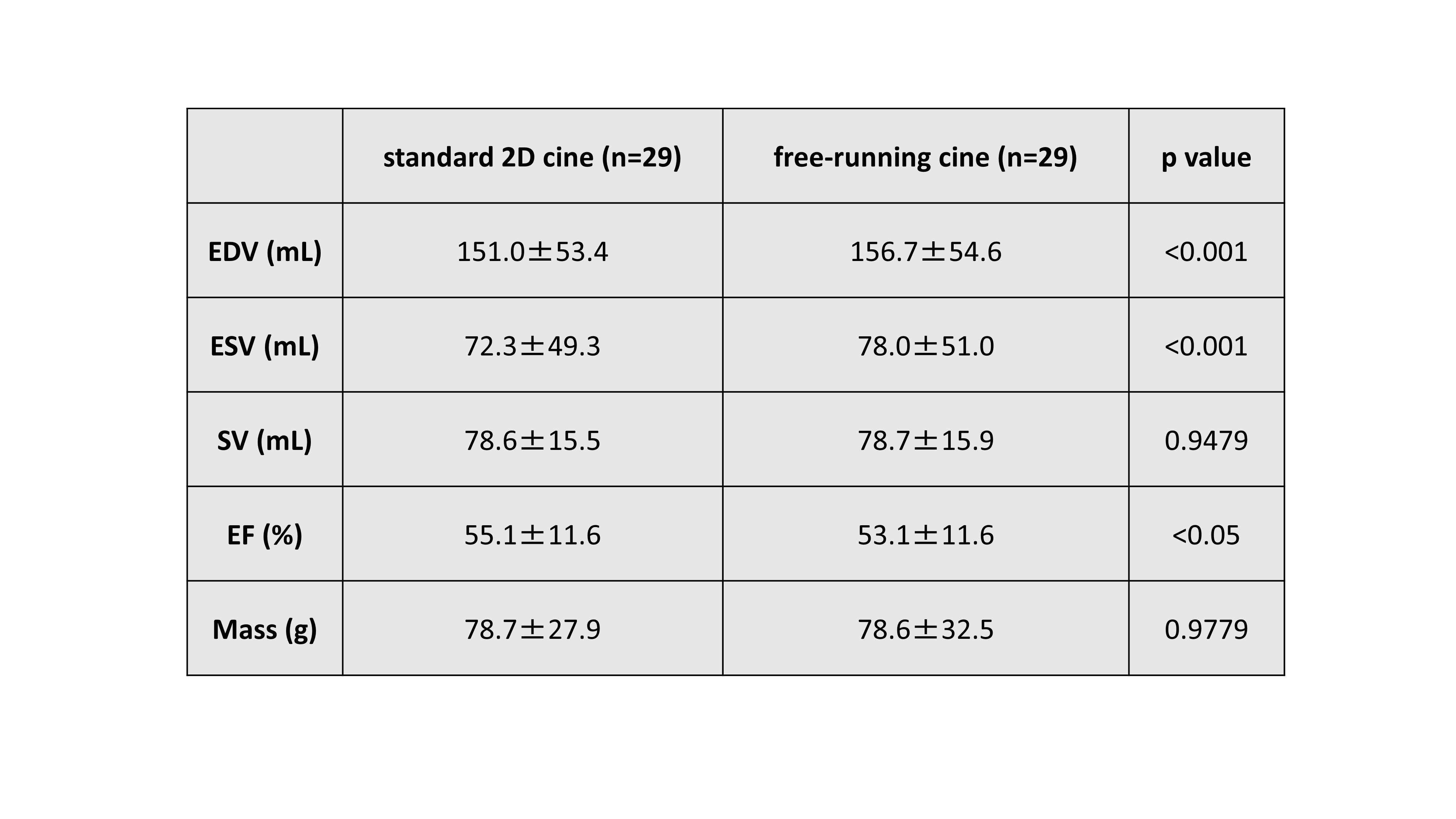
Figure 3. Results of LV volumetry for 2D cine MRI and free
running cine MRI of temporal width of 50ms. Data are given as the mean ± standard deviation.
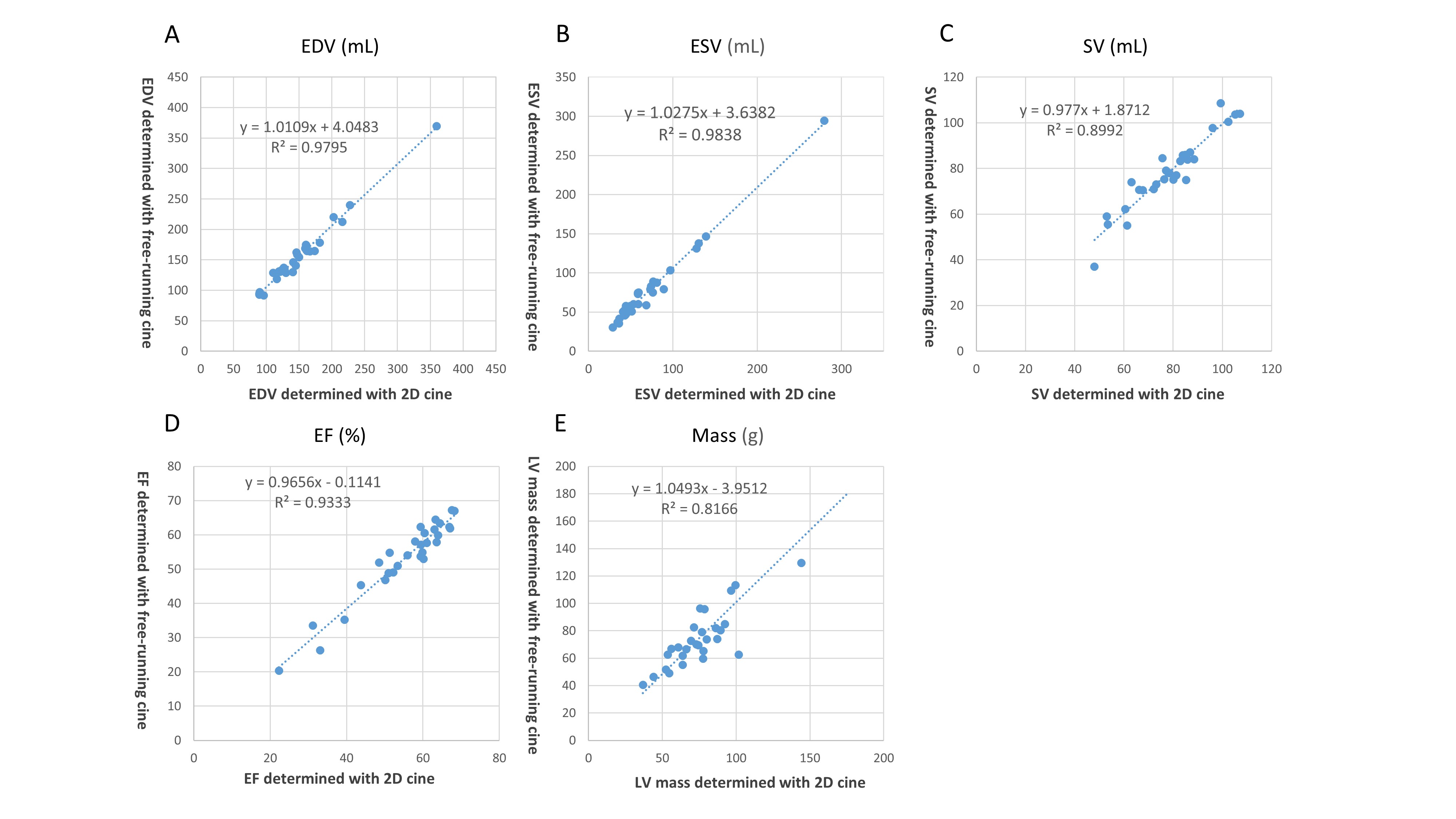
Figure 4. Correlation between 2D cine MRI and free running
cine MRI of temporal width of 50ms for EDV (A), ESV (B), SV (C), EF (D) and LV
mass (E). Good agreement between the 2 methods was shown for all measurements
on linear regression analysis.
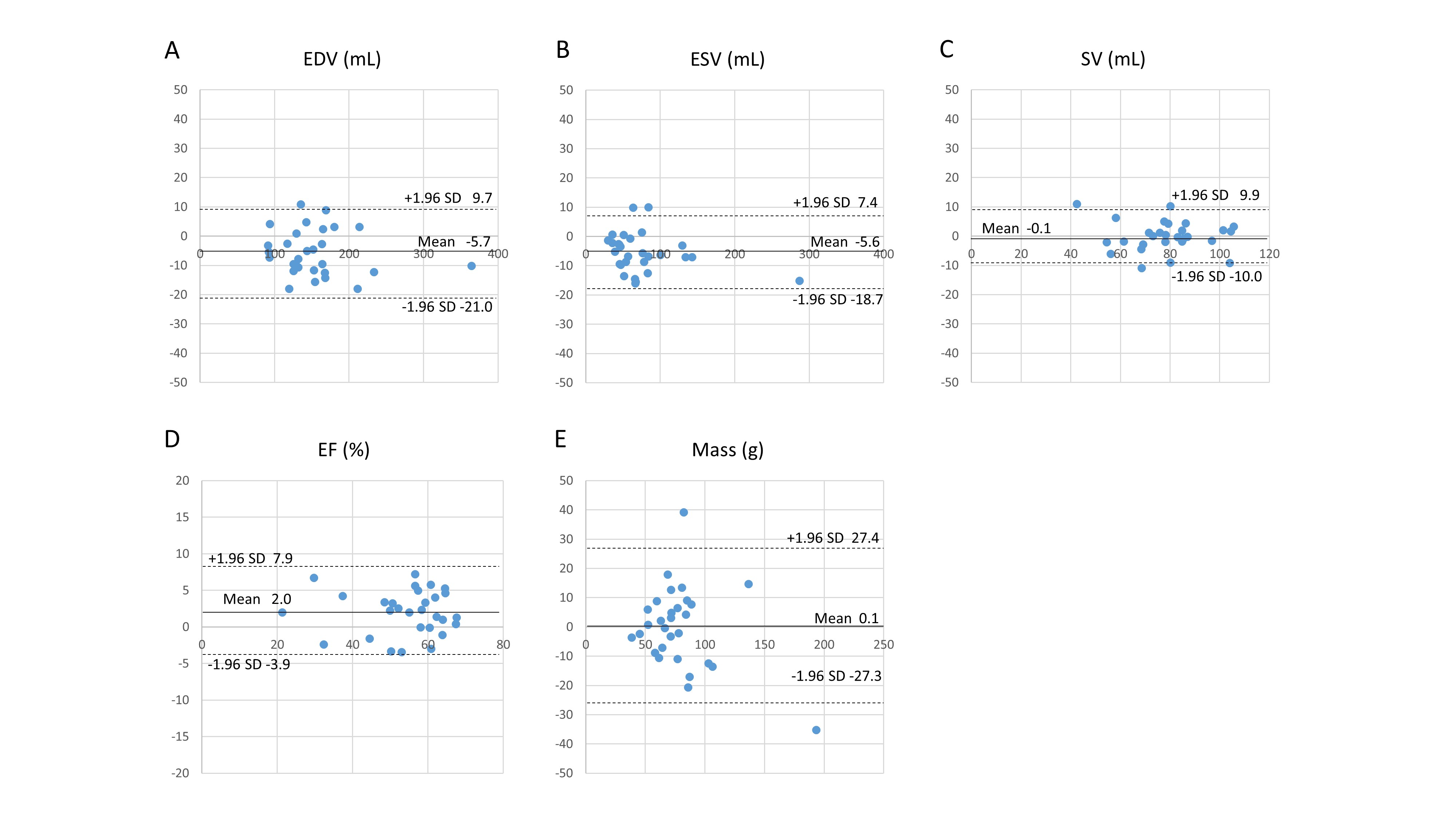
Figure 5. Mean differences in left
ventricle (LV) measurement between breath-hold standard and free-breathing
compressed sensing cine magnetic resonance imaging: (A) EDV; (B) ESV; (C) SV;
(D) EF; and (E) LV mass. (––) Mean difference; (– – –) 95% limits of agreement
(i.e., mean ±1.96 SD).
DOI: https://doi.org/10.58530/2023/5138