5135
Assessment of cardiac function using free-breathing, motion corrected artificial intelligence cine: comparison with conventional cine
Lingping Ran1, Lu Huang1, Xianghu Yan1, Yun Zhao1, and Liming Xia1
1Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
1Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Synopsis
Keywords: Heart, Heart
Routine cardiac functional assessment with conventional balanced steady state free precession (bSSFP) cine sequence generally requires multiple breath-holding (BH) and long examination time. The purpose of this study was to evaluate the image quality and bi-ventricular functional analysis using a novel free-breathing (FB) artificial intelligence (AI) cine method with motion corrected (MOCO) in a clinical context. Compared to conventional multiple BHs cine, the proposed FB-MOCO AI cine method achieved comparable image quality with shortened scan times. No significant difference in ventricular volumetric and functional parameters were found, suggesting its potential applicability for clinical applications.Introduction
Conventional balanced steady state free precession (bSSFP) cine sequence with breath-holding (BH) is considered the standard method in cardiac MR for ventricular volumes and functional assessment. However, it requires multiple BHs for a complete scan. Recently, the value of deep learning has been demonstrated in cardiac MR to reduce scan time and/or improve image quality. An artificial intelligence (AI) cine method has been previously proposed with two different imaging protocols: one requires BH and the other allows for free-breathing (FB) with motion corrected (MOCO). This study aims to assess the image quality, biventricular volumes, function and left ventricular (LV) mass of the proposed AI cine method with BH and FB-MOCO, respectively, in comparison with the standard bSSFP cine with BH.Methods
Study population:This clinical study was approved by the local Institution Review Board and each participant signed informed consent before examination. From August to September 2022, 21 healthy volunteers (age 25.7±1.5, nine male) and 17 patients (age 41.2±15.7, ten male) were prospectively recruited to undergo cardiac MR examination. The clinical indications of 17 patients included cardiomyopathy, hypertensive heart disease, and other cardiovascular diseases.
MR imaging protocol:
All cardiac MR scans were performed on a 3T scanner (uMR 790, United Imaging Healthcare, Shanghai, China) with a dedicated 24-channel cardiac coil. The standard BH cine protocol was first performed, followed by the proposed BH AI cine and FB-MOCO AI cine protocols in subsequence. AI cine was scanned using a bSSFP sequence with phase-encoding lines following a Latin Hypercube under-sampling pattern. All cine scans were applied in short-axial view with matched slice positions. The detailed imaging parameters for all protocols are summarized in Table1.
Image analysis:
All qualitative and quantitative image analysis were independently performed by two radiologists with 7 and 2 years of experience in cardiovascular imaging. The overall image quality of short-axis images was evaluated individually with a 5-point Ordinal Likert scale as: 1-nondiagnostic; 2-poor; 3-adequate; 4-good; 5-excellent1. For quantitative functional analysis, the short 3-D module of commercial software cvi42, v.5.3 (Circle Cardiovascular Imaging, Calgary, Canada) was used to automatically delineate the LV endocardial and epicardial contours and the right ventricle (RV) endocardial contours at end-diastole and end-systole. Manual corrections were performed when necessary. Then the volume and functional parameters of LV/RV including end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), ejection fraction (EF), cardiac output (CO), cardiac index (CI) and LV end-diastolic mass (LVEDM) were extracted.
Statistical analysis:
Statistical analysis was performed using SPSS (version 26.0, Chicago, IL). Continuous data was described as mean ± SD or median (P25, P75). Ordinal Likert scores and quantitative parameters from two radiologists were averaged prior to analysis. The qualitative scores and quantitative values between the three protocols were evaluated by paired Wilcoxon signed-rank test and paired t-tests. The agreement of the measured quantitative parameters obtained from standard BH cine, BH AI cine and FB-MOCO AI cine were assessed by ICC. The interobserver agreement of measured quantitative parameters and scoring data was assessed with ICC and weighted kappa, respectively. P<0.05 was considered as statistically significant.
Results
All 38 participants successfully underwent standard breath-hold cine and two AI cine protocols. The mean scan time of BH AI cine (14.5±2.1s) and FB-MOCO AI cine (14.4±2.0s) were significantly shorter than standard BH cine (81.7±12.8s, P˂0.001 for both). Overall image quality scores of BH AI cine (4.3±0.7) and FB-MOCO AI cine (4.3±0.6) were comparable to standard BH cine (4.4±0.8) with no statistically significant difference (P=0.515, 0.411, respectively). All measured RV volume and function parameters and some LV parameters of BH AI cine and FB-MOCO AI cine sequences presented no statistical difference compared to standard BH cine. However, some LV parameters of BH AI cine and FB-MOCO AI cine had a small but statistically significant difference compared to standard BH cine. There was also a small but statistically significant difference in biventricular EDV, ESV and LVEF between BH AI cine and FB-MOCO AI cine. LV mass, RVEF, and biventricular SV, CO and CI between two AI cine protocols presented no statistical difference (Table 2). Furthermore, the agreement among standard BH cine, BH AI cine and FB-MOCO AI cine in measured quantitative cardiac MR parameters assessed with ICC were all excellent (Table 3). The interobserver agreement for the measured quantitative parameters analysis with ICC were all good (Table 4). Interobserver agreement of image quality for standard BH cine, BH AI cine and FB-MOCO AI cine were also good for all (weighted kappa, 0.67, 0.66, 0.61, respectively).Discussion and Conclusion
This study demonstrates the feasibility of free-breathing, motion corrected AI cine, which offered comparable image quality, ventricular volumetric and functional indices with significantly shorter scan time compared to standard bSSFP cine. It shows the potential as an alternative for clinical use with simplified scanning process, especially with patients who may have difficulties to exercise multiple breath-holding or remain cooperative in the long examination times.Acknowledgements
No acknowledgement found.References
1. Zucker EJ, Sandino CM, Kino A, Lai P, Vasanawala SSet al. Free-breathing Accelerated Cardiac MRI Using Deep Learning: Validation in Children and Young Adults. Radiology. 2021;300(3):539-548.Figures
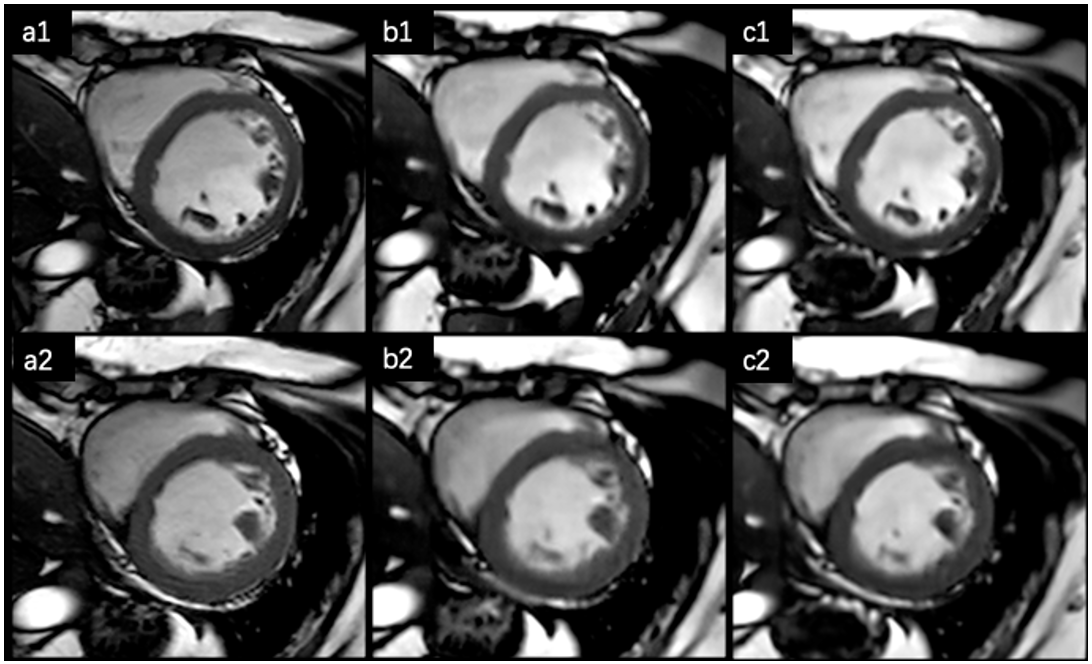
Figure1. Representative images of a 45 years old female patient diagnosed with dilated cardiomyopathy. The a-c images from standard BH cine, BH AI cine and FB-MOCO AI cine sequence, respectively, a1-c1 showed end-diastolic and a2-c2 showed end-systolic short-axis images of ventricle. Both observers rated image quality from all three sequences as excellent (score, 5), only the end-systolic image of standard BH cine (a2) showed minimal motion-related artifacts.
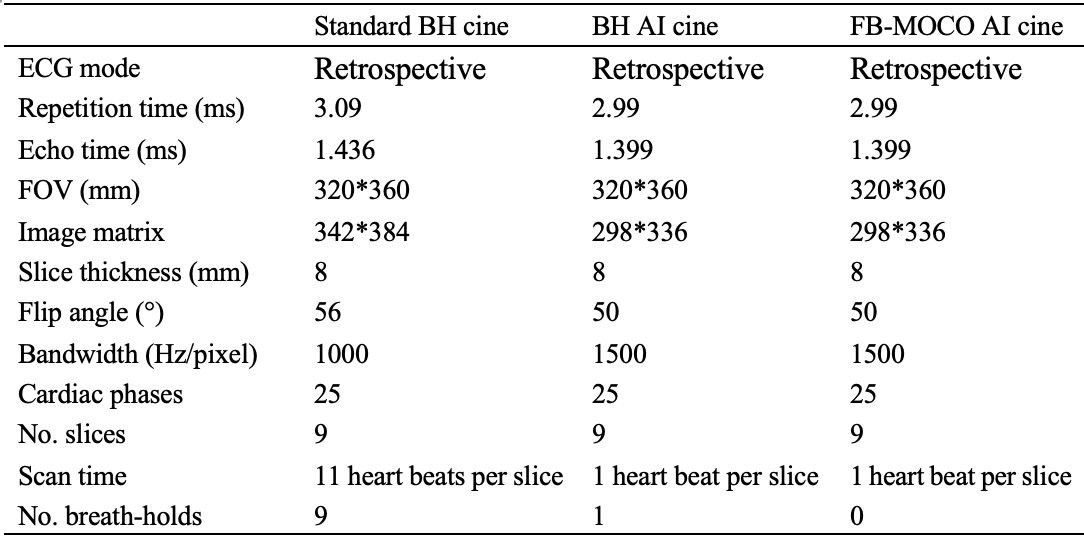
Table 1. Imaging parameters
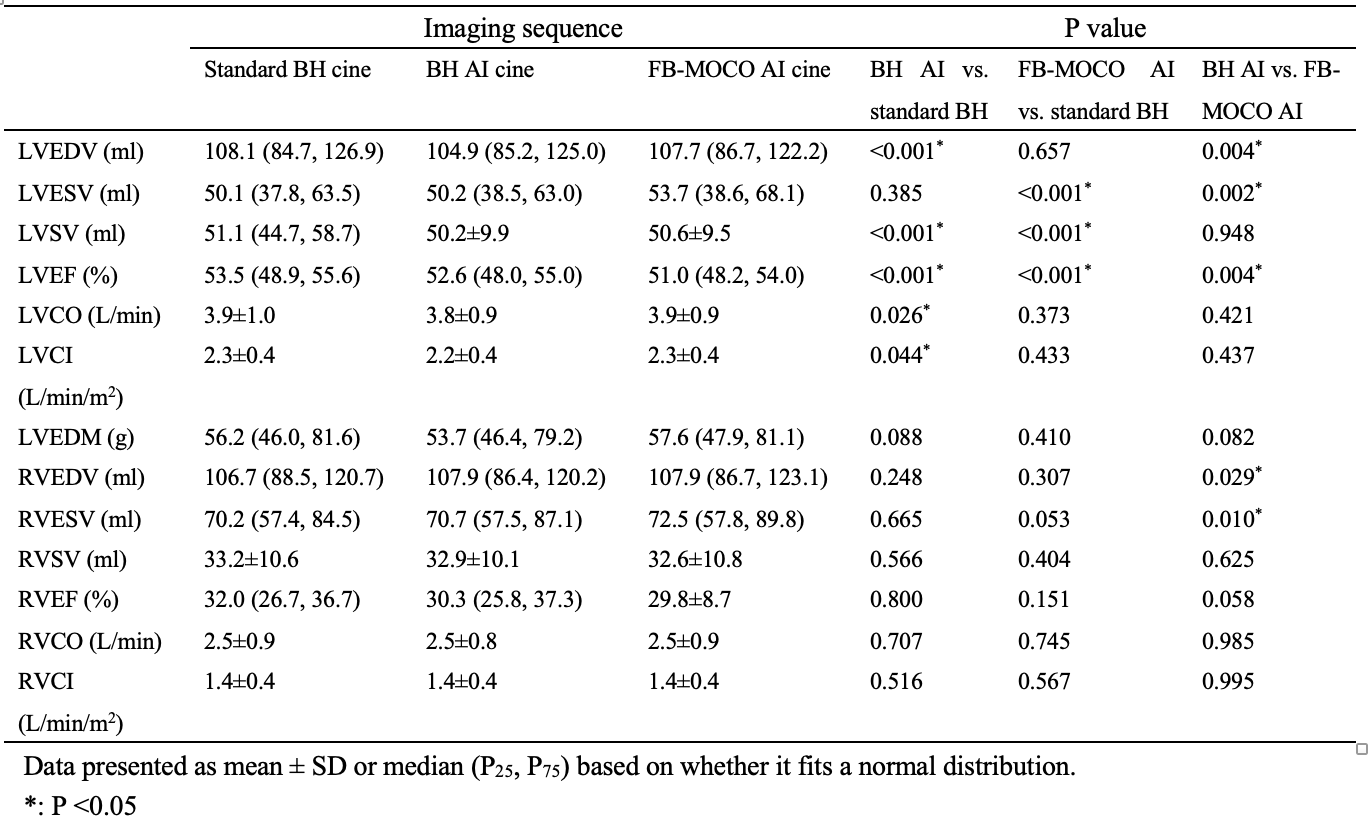
Table 2. Measured quantitative cardiac MR parameters
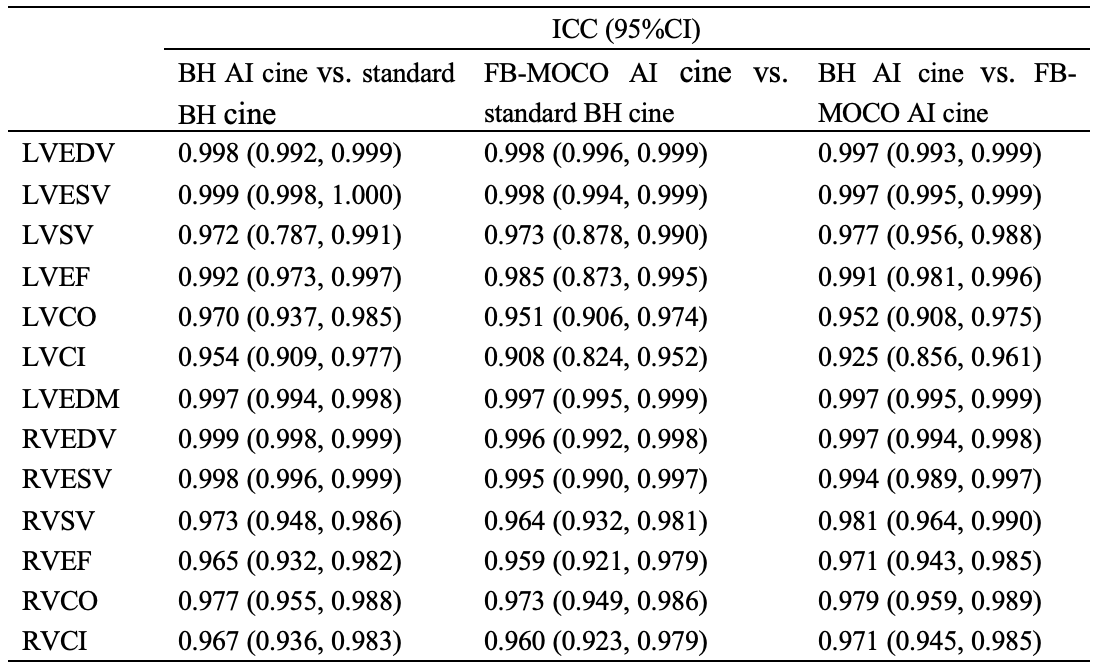
Table 3. Agreement among standard BH cine, BH AI cine and FB-MOCO AI cine in measured cardiac MR parameters with ICC
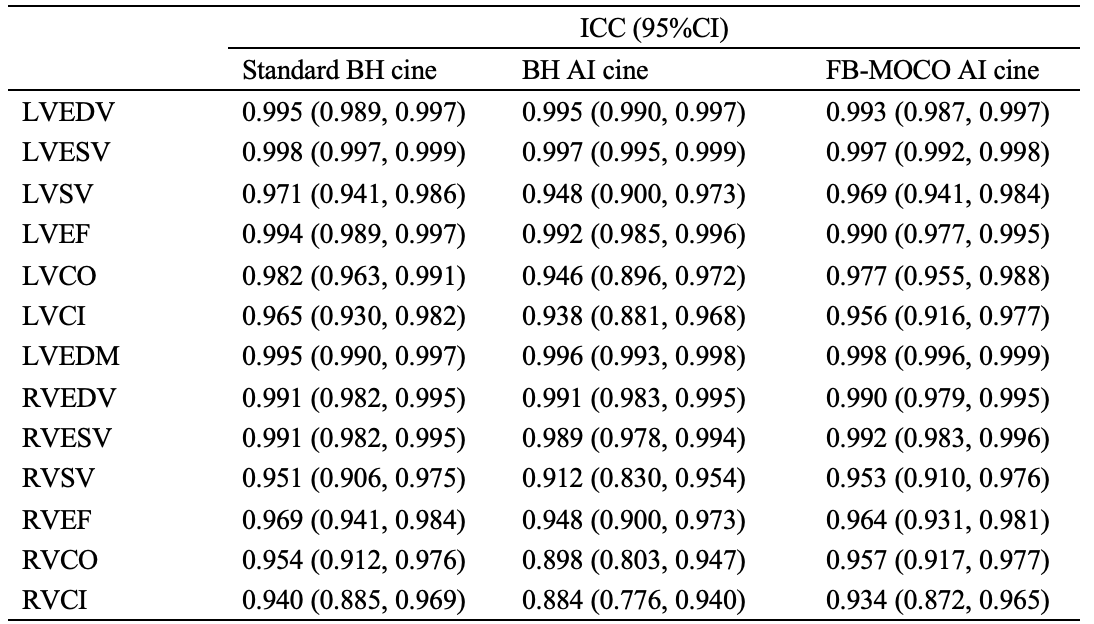
Table 4. Interobserver agreement of two radiologists for measured cardiac MR parameters with ICC
DOI: https://doi.org/10.58530/2023/5135