5131
Novel Reconstruction Method to Improve the Sharpness of Free Breathing Cardiac MR Late Gadolinium Enhancement Images on a Commercial 0.55T System1The Ohio State University, Columbus, OH, United States, 2Siemens Healthineers, Columbus, OH, United States
Synopsis
Keywords: Myocardium, Low-Field MRI, Late Gadolinium Enhancement
Low-field cardiac MR imaging has intrinsically low SNR that degrades the image quality, especially for LGE imaging. Using multiple acquisitions and motion-corrected averaging is a well-established method to improve SNR. However, the ineffectiveness of MOCO at low field leads to blurring. We proposed a novel method that integrates motion correction into compressed sensing and reconstructs a single motion-corrected image. Quantitative sharpness measurements demonstrate that the proposed method improves boundary sharpness, independent of differences in SNR.Introduction
Low-field scanners with limited gradient performance potentially offer a cost-effective alternative to high-field MRI for cardiac imaging. However, the intrinsically low signal-to-noise ratio (SNR) at low field can degrade image quality, especially in late gadolinium enhancement (LGE) 1, 2. Reconstruction methods, e.g., compressed sensing (CS), can improve individual image SNR. The well-established motion correction (MOCO) + averaging method2,3 can also improve SNR when multiple acquisitions are available. Higher acceleration is needed to overcome limited gradient performance (26mT/m, 45 mT/m/ms); however, at low field this leads to low SNR single-shot source images that can reduce the accuracy of motion correction. Averaging of incorrectly registered source images introduces blurring and degrades image quality. In this study, we propose a novel MOCO compressed sensing (CS) method (MOCO + CS) to improve LGE image sharpness by incorporating MOCO into the CS image reconstruction algorithm.Methods
Multiple single-shot LGE images were acquired 10 to 20 minutes following injection of 0.15 mmol/kg gadolinium contrast agent (Gadobutrol, Bayer Healthcare, LLC, Whippany, NJ) in 10 healthy volunteers on a commercial 0.55T MR scanner (Free.Max, Siemens Healthcare, Erlangen, Germany). The k-space data from these scans were used to develop and test the effectiveness of the proposed MOCO + CS method.24 sets of k-space raw data from LGE image series were retrospectively included, comprising 18 short-axis, 3 four-chamber long-axis, and 3 two-chamber image series. A pseudo-random down-sampling pattern4 with an effective acceleration rate = 6 was used for data acquisition.
All k-space data sets were reconstructed using both the MOCO + averaging method that employs a CS reconstruction of the source images prior to MOCO, and the proposed MOCO + CS method. MOCO + CS incorporated the estimated motion displacement field into the CS cost function, i.e.:
$$argmin_x || DFSRx - k_0 ||^2_2 + \rho_x|| TV_xx ||_1$$
where x is the motion-corrected averaged image; k0 is the acquired k-space raw data; R is the forward MOCO operator; S is the sensitivity map; F is the Fourier transform operator; D is the downsampling operator; TVx is the spatial total variation operator; ρx is an adjustable parameter. For the implementation of R, the “demon” MOCO algorithm was employed5.
Boundary (edge) sharpness was evaluated in each pixel at the boundary between the LV myocardium and blood pool using the sigmoid function fitting method along the normal direction6. A paired t-test was used to evaluate the significance of the boundary sharpness differences. To account for the impact of SNR on the measured sharpness, Gaussian noise was added to the MOCO + averaging images to generate a new image series that matched the SNR of the MOCO + CS method.
Results
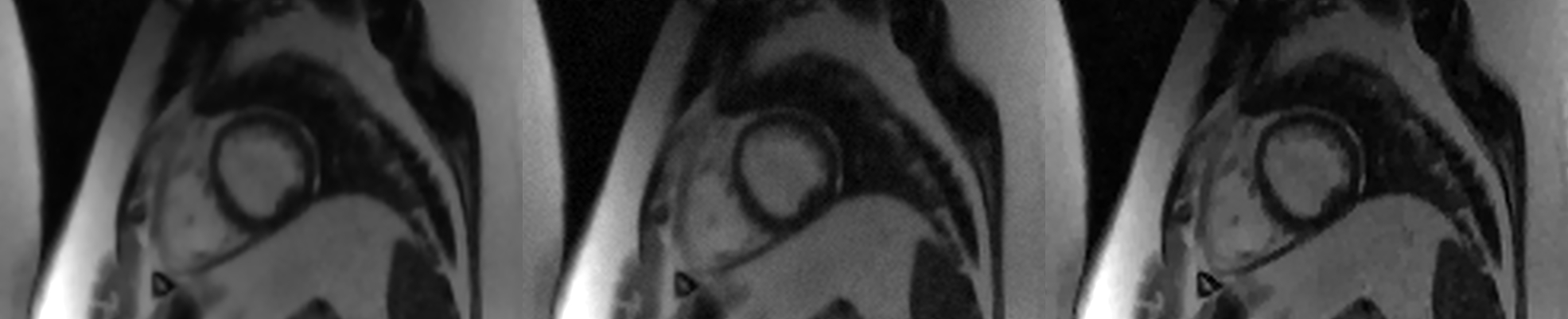
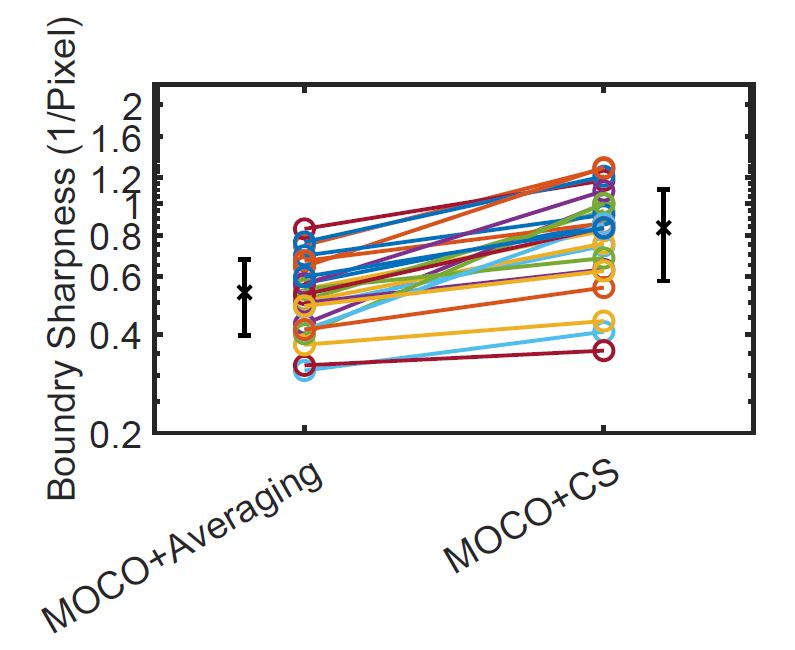
Figure 1 shows a typical image reconstructed by both methods, and an SNR matched image. The image reconstructed using the proposed MOCO + CS method has visibly improved sharpness. The image sharpness of MOCO + averaging method, SNR-matched MOCO + averaging method, and the MOCO + CS method are 0.54+/-0.14 pixel-1, 0.64+/-0.18 pixel-1 and 0.84+/-0.26 pixel-1 (p-value < 0.001), respectively (Figure 2, the SNR-matched result is not shown).Conclusion
This study demonstrates the proposed MOCO + CS method improves the sharpness of free-breathing LGE images acquired using a 0.55T commercial scanner. The sharpness increase was shown to be independent of SNR differences. We believe the loss of sharpness in the traditional MOCO + averaging method is due to the challenges of applying MOCO to low-SNR source images resulting in residual misregistration, which in turn causes blurring of the averaged image result. The proposed method, in contrast, leverages all available raw data to reconstruct one image frame; therefore, it is less sensitive to inaccuracies in the motion correction displacement field. Further studies are warranted in a patient population with myocardial scar and fibrosis.Acknowledgements
No acknowledgement found.References
1. Simonetti, Orlando P., et al. "An improved MR imaging technique for the visualization of myocardial infarction." Radiology 218.1 (2001): 215-223.
2. Kellman, Peter, et al. "Motion‐corrected free‐breathing delayed enhancement imaging of myocardial infarction." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 53.1 (2005): 194-200.
3. Kellman, Peter, et al. "Dark blood late enhancement imaging." Journal of Cardiovascular Magnetic Resonance 18.1 (2017): 1-11.
4. Ahmad, Rizwan, et al. "Cartesian sampling for dynamic magnetic resonance imaging (MRI)." U.S. Patent No. 11,294,009. 5 Apr. 2022.
5. Dirk-Jan Kroon (2022). Multimodality non-rigid demon algorithm image registration (https://www.mathworks.com/matlabcentral/fileexchange/21451-multimodality-non-rigid-demon-algorithm-image-registration), MATLAB Central File Exchange. Retrieved July 25, 2022.
6. Ahmad, Rizwan, Yu Ding, and Orlando P. Simonetti. "Edge sharpness assessment by parametric modeling: application to magnetic resonance imaging." Concepts in Magnetic Resonance Part A 44.3 (2015): 138-149.
Figures