5123
Data-driven clustering for ECG-free cine MRI with robustness against irregular cardiac motion1Physics and Biology in Medicine Graduate Program, University of California,Los Angeles, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 3Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 4Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 5Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 6Department of Radiation Oncology, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Keywords: Arrhythmia, Machine Learning/Artificial Intelligence
Both ECG-gating and self-gated approaches are used for cardiac motion binning in segmented cardiac cine MRI. Typical self-gated methods reduce ECG-dependency by assuming periodic cardiac motion, but may be less reliable in the presence of irregular cardiac motion. We propose a novel clustering algorithm that incorporates regularization in both temporal and cluster dimension to provide robustness against irregular cardiac motion in complex arrhythmias such as atrial fibrillation and premature ventricular contraction. Compared with images from k-means clustering, initial validation using the modified algorithm shows higher image quality scores with comparable single-to-noise ratio (SNR) and image sharpness.Introduction
Segmented 2D cardiac cine imaging [1] is widely used to evaluate cardiac morphology and function. Self-gating [2-5] is an alternative approach to ECG gating but typically assumes periodic cardiac motion, which may be susceptible to cardiac motion irregularities. We have previously shown [6] that a segmented k-space, Cartesian golden-step balanced steady-state free precession (bSSFP) sequence with motion navigators can be used with k-means clustering to reduce the dependency on regular cardiac motion assumptions. To tailor our cine MRI approach for complex arrhythmias such as atrial fibrillation and premature ventricular contraction (PVC), we propose a novel clustering algorithm to further enhance robustness against irregular cardiac motion.Methods
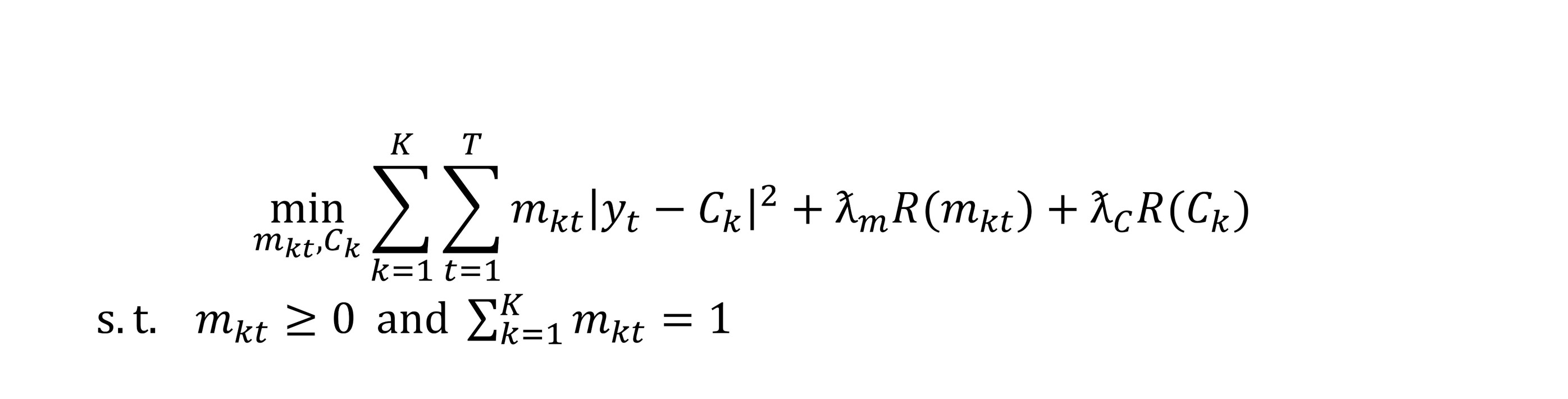
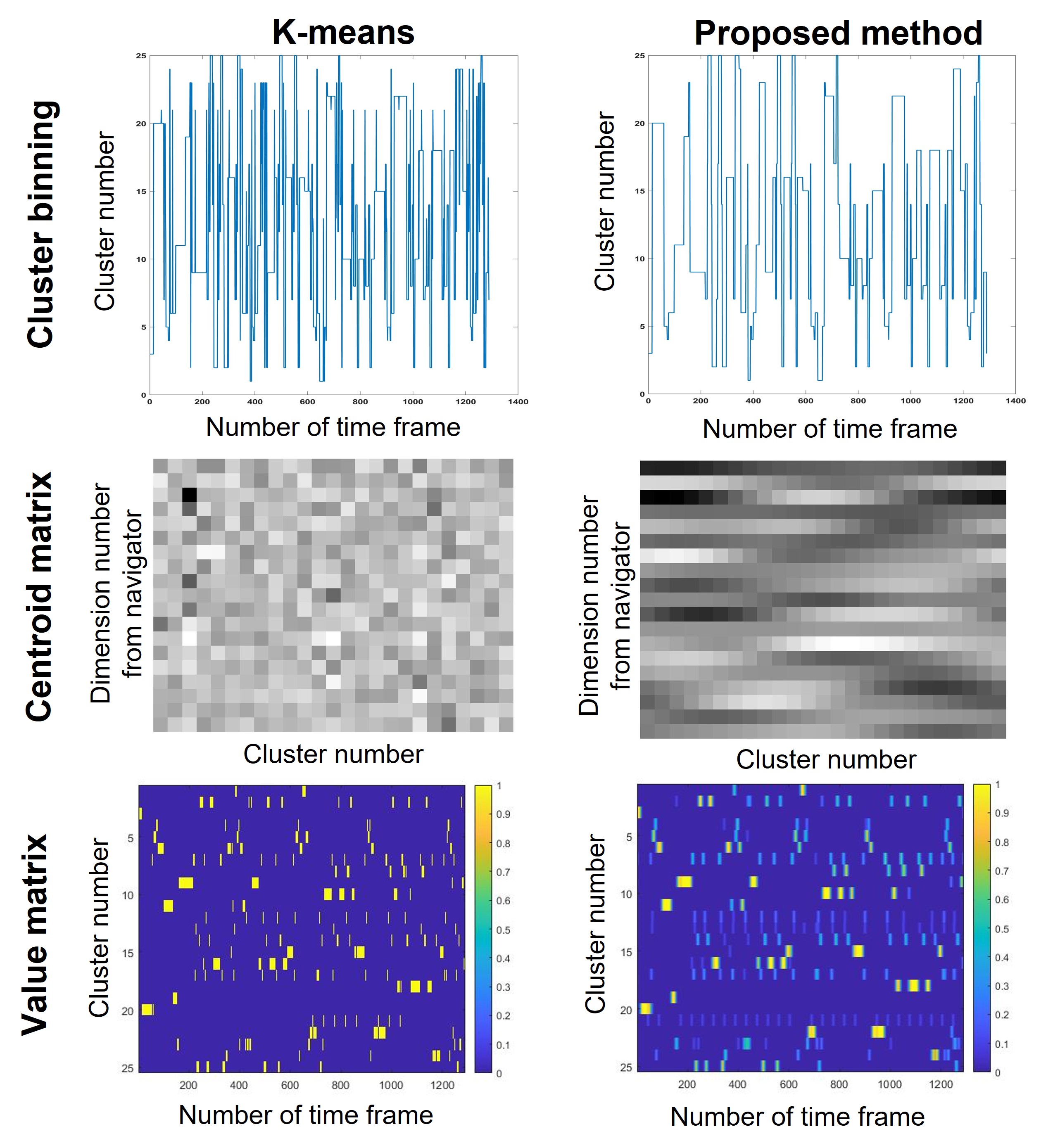
In prior work [6], motion navigators were used to acquire the motion signal, and k-means clustering was applied to bin the navigator data for subsequent image reconstruction. To adapt to nonstationary irregular and sometimes chaotic cardiac motion in complex arrhythmias, we further customized the optimization setting to along the temporal and cluster dimensions (Figure 1). Specifically, a “probability-like” matrix was used for determining navigator association with cardiac phase bins. Weight values in the matrix ranged from 0 to 1 and the sum along the cluster dimension was 1. To encourage temporal continuity and smooth association, centroid difference in adjacent clusters and variation along time were penalized. Compared to the output of the k-means, the additional adaptive strategies were designed to provide an output matrix with greater flexibility for subsequent image reconstruction. To ensure a fair comparison with the prior k-means method, we first chose bin numbers that correspond to the largest matrix values along the cluster dimension to generate a similar output as the k-means method (Figure 2). Images are then reconstructed using the binned outputs from each method.To test the proposed algorithm, six patients with arrhythmia (n=5 atrial fibrillation and n=1 PVC, 6 male) were scanned on a clinical 3.0T scanner (Skyra, Siemens) using our free-running, segmented, golden step, Cartesian bSSFP sequence (FA=55, matrix size=208*172, spatial resolution=1.8mm x 1.8mm x 8mm, TE/TR = 1.7ms /3.4ms, segments=20). A left ventricular short-axis stack was acquired during breath-holding. To compare the performance of the proposed clustering algorithm and the previous k-means method, we calculated the single-to-noise ratio (SNR) and image sharpness of the base, mid and apical 2D cine images from the two algorithms. The image sharpness is measured by drawing a linear profile across the interventricular septum and calculating the average slope of the signal magnitude. A composite 4-point Likert scale image quality score was used to evaluate the cine images (1=non-diagnostic, 2=diagnostic, 3=good image quality with few artifacts that do not obscure the cardiac borders, 4=excellent image quality). Paired t-tests were used to compare the SNR and image sharpness; whereas the Wilcoxon signed-rank test was used to compare image quality scores.
Results and Discussion
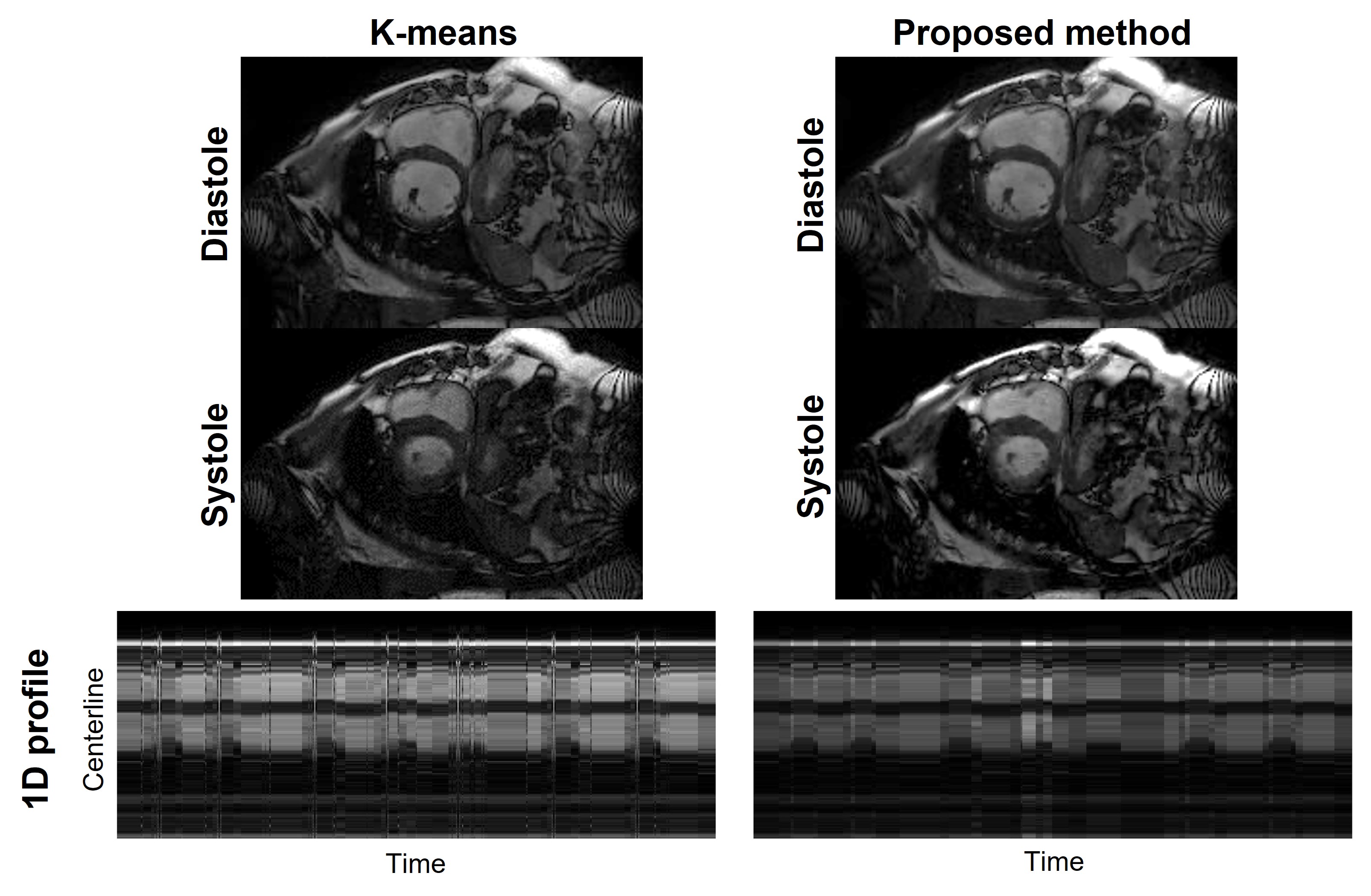
The average age of the patients was 69.2±11.5 years. The SNR values for the k-means and the proposed clustering approaches were 8.27±0.99 vs 8.31±1.27 (p=0.24), respectively. Image sharpness of the k-means and proposed clustering were 0.21±0.05 vs 0.23±0.08 (p=0.59), respectively. For the image quality scores, 71% of images of the k-means clustering received scores = 3; none received the highest score of 4. Seventy-six percent of images from the proposed clustering received scores >=3 and 30% of the images receive score 4. A higher percentage of reconstructed images using the proposed method received higher image scores (p<0.05). Figure 2 shows the data binning results, cluster centroid matrixes and cluster value matrixes of the k-means clustering and the proposed clustering algorithm from one patient with atrial fibrillation. The data binning results from the proposed method have better continuity along time dimension compared with k-means method. Similarly, the proposed method has better continuity along the cluster dimension of the cluster centroid matrices. These observations indicate good performance of the two additional regularization terms. In the cluster value matrices, the proposed method assigns high values to more time frames compared with the k-means method but maintains the features of irregular cardiac motion. Diastolic and systolic images in a patient with atrial fibrillation are shown in Figure 3. Although the image quality appears comparable for both methods, the 1D profile suggests better continuity along the time dimension using the proposed method. These findings suggest that the proposed method may have better performance than the k-means method for adaptive handling of irregular cardiac motion such as complex arrhythmias.Conclusion
Compared with the k-means clustering approach, the addition of two regularization terms in the temporal and cluster dimensions can enhance the handling of irregular cardiac motion often seen in complex arrhythmias. In the five atrial fibrillation and one PVC patients, images using the proposed method for binning achieved higher image quality scores than those from the k-means binning approach. In addition, the two methods have similar SNRs and image sharpness. Confirmation of these findings in a larger set of patients with various types of arrhythmias will be needed.Acknowledgements
No acknowledgement found.References
1. Atkinson, Dennis J., and R. R. Edelman. "Cineangiography of the heart in a single breath hold with a segmented turboFLASH sequence." Radiology 178.2 (1991): 357-360.
2. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD‐GRASP: golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. Magnetic resonance in medicine. 2016;75(2):775-88.
3. Han F, Zhou Z, Han E, Gao Y, Nguyen KL, Finn JP, et al. Self‐gated 4D multiphase, steady‐state imaging with contrast enhancement (MUSIC) using rotating cartesian K‐space (ROCK): validation in children with congenital heart disease. Magnetic resonance in medicine. 2017;78(2):472-83.
4. Pang J, Sharif B, Fan Z, Bi X, Arsanjani R, Berman DS, et al. ECG and navigator‐free four‐dimensional whole‐heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magnetic resonance in medicine. 2014;72(5):1208-17.
5. Roy CW, Di Sopra L, Whitehead KK, Piccini D, Yerly J, Heerfordt J, et al. Free-running cardiac and respiratory motion-resolved 5D whole-heart coronary cardiovascular magnetic resonance angiography in pediatric cardiac patients using ferumoxytol. Journal of Cardiovascular Magnetic Resonance. 2022;24(1):1-12.
6. Ming Z, Pogosyan A, Colbert CM, Wu HH, Ruan D, Hu P, et al. ECG-free 2D cardiac cine MRI with data-driven clustering. Proceedings of the 31st International Society for Magnetic Resonance in Medicine (ISMRM), 4096.
Figures