4982
Dual-Band Adiabatic Pulses in cardiac MRI: Application in Black Blood Imaging at 3T
Ayda Arami1, Christal van de Steeg-Henzen2, Hildo J.Lamb3, and Sebastian Weingärtner1
1TU Delft, Delft, Netherlands, 2HollandPTC, Delft, Netherlands, 3LUMC, Leiden, Netherlands
1TU Delft, Delft, Netherlands, 2HollandPTC, Delft, Netherlands, 3LUMC, Leiden, Netherlands
Synopsis
Keywords: Myocardium, RF Pulse Design & Fields
Black-Blood imaging is an integral part of clinical cardiac MRI, due to it’s clear depiction of the cardiac morphology. Double inversion recovery, is most commonly used for black-blood contrast, by successively applying a non-selective inversion and a slice-selective reinversion. In this work, we investigate dual band adiabatic inversion pulses, as an alternative, to achieve nulling of the blood signal outside of the imaging slice. Thorough blood suppression and comparable noise performance to double inversion recovery were demonstrated in vivo while achieving an 11% reduction in SAR and a 10% reduction in pulse duration.Introduction
Black-blood (BB) imaging1 is widely used in clinical cardiac MRI for its excellent depiction of cardiac morphology and Double Inversion Recovery (DIR) is the method of choice for reliable black-blood contrast2. In DIR, a non-selective inversion is followed by a slice selective re-inversion centered around the imaging slice. Thus, inverted blood is flowing into the imaging slice, while the myocardial signal is restored. However, DIR requires long preparation pulses with high SAR, in particular when being used with adiabatic pulses. Furthermore, magnetization decay during the preparation can compromise the imaging SNR. In this work, we sought to evaluate the use of multi-band adiabatic inversion pulses as an alternative to DIR. Dual-band adiabatic (DBA) inversion is used to suppress blood signals outside the imaging slice. The proposed pulse is evaluated in simulations and used in phantom and in-vivo imaging at 3T.Methods
A dual-band adiabatic inversion pulse is created by combining frequency-shifted adiabatic full passage pulses, with one of the bands being time reverse3,4. Hyperbolic secant pulses with ꞵ=5 and duration=25ms were used for each band (Fig. 1). For a given gradient strength single-band bandwidth and the band spacing were chosen to achieve a 28mm pass-band and 56mm stop-bands (Fig.1). Bloch simulations of the adiabatic dual-band pulses were used to evaluate the slice profile and resilience against B1+ inhomogeneities for different gradient strengths and T2 times (Fig. 2). The slice profile of the DBA inversion was measured on a 3T scanner (Ingenia, Philips) with a breath-hold cardiac triggered turbo spin echo sequence (Fig. 3), including the following parameters: resolution=1.8x1.8x8mm3, inversion delay=420ms, TE/TR=10/1053ms, FOV=300x300mm2 , Echo Train Length=20. The proposed preparation was compared with conventional adiabatic DIR, using two successive hyperbolic scant pulses (total duration~27ms, bandwidth~760Hz). Phantom experiments were used to validate the slice profile. Ten repetitions were acquired to measure the SNR in the passband of the two preparations. In vivo images were obtained in three healthy subjects (1 female, 27.33±5.5y) and three repetitions each to illustrate the use of the pulse for black blood imaging and quantify the noise variability in the pass-band.Results
Fig. 1 illustrates the pulse shape and the simulated slice profile of different DBA pulses obtained with constant stop/pass-band widths but varying gradient strength. Low gradient strength leads to less sharp transitions, while high gradient strength reduces the inversion efficiency in the stop-bands. Thus, a gradient strength of 1000uT/m was used as a trade-off for phantom and in-vivo imaging. DBA inversion shows good resilience against B1+ inhomogeneities up to 3.5µT(45%) with less than 5% drop in inversion efficiency of the stop-bands and negligible T2 effects (Fi.g 2). Phantom images confirm sharply delineated stop-bands, for both the conventional and the DBA pulses (Fig. 4). Black-blood images obtained with DIR and with DBA show thorough suppression of the blood in both ventricles. Good delineation of the cardiac morphology without visible artifacts related to B1+ or B0 inhomogeneities is achieved. Comparable noise variability in the myocardium is obtained with both pulses leading to an average normalized SNR of 5% for DIR and 2.88% for DBA. The B1+rms was 1.04 and 1.17 µT for DIR and DBA preparation modules, respectively.Discussion
In this study, we explored the use of the DBA inversion pulse for black-blood imaging in cardiac MRI. Our results show good delineation between pass- and stop-bands in simulations and phantom imaging, and thorough blood suppression in vivo. A prescribed stop/pass-band width can be achieved at various gradient strengths, by modifying the bandwidth and the band spacing of the combined single-band pulses. This allows for a trade-off of band profile sharpness against inversion efficiency in the stop bands. Phantom results with a gradient strength of 500 µT/m lead to blurry transitions. Additionally, off-resonances can lead to distortion of the band transition and, thus, artifacts in vivo. Consequently, 1000 µT/m was found to be an ideal sweet spot at 3T, but higher gradient strength (i.e. higher stop-band bandwidth and band spacing in Hz) may be required at higher field strengths to further mitigate of-resonance artifacts. In a black-blood imaging sequence, DBA pules showed comparable pass-band SNR in phantom and blood signal suppression in-vivo. The proposed pulse was achieved with an 11% reduction in SAR and 10% in pulse duration, compared with the conventional application of selective/non-selective inversion pulses. This gain in SAR can allow for higher spin-echo flip-angles and may enable further improved image quality, in particular at high field strengths.Acknowledgements
No acknowledgement found.References
[1]Edelman, R. R., Chien, D., & Kim, D. (1991). Fast selective black blood MR imaging. Radiology, 181(3), 655-660.
[2]Saranathan, M., Worters, P. W., Rettmann, D. W., Winegar, B., & Becker, J. (2017). Physics for clinicians: Fluid‐attenuated inversion recovery (FLAIR) and double inversion recovery (DIR) Imaging. Journal of Magnetic Resonance Imaging, 46(6), 1590-1600.
[3]Kupce E, Freeman R. J Magn Reson Ser A (1995).Adiabatic Pulses for Wideband Inversion and Broadband Decoupling Journal of Magnetic Resonance, Series A, Volume 115, Issue 2, p. 273-276.[4]Ouwerkerk, R., Edden, R.A., & Morgan, R.H. (2006). Multi-Band Adiabatic Pulses.
Figures
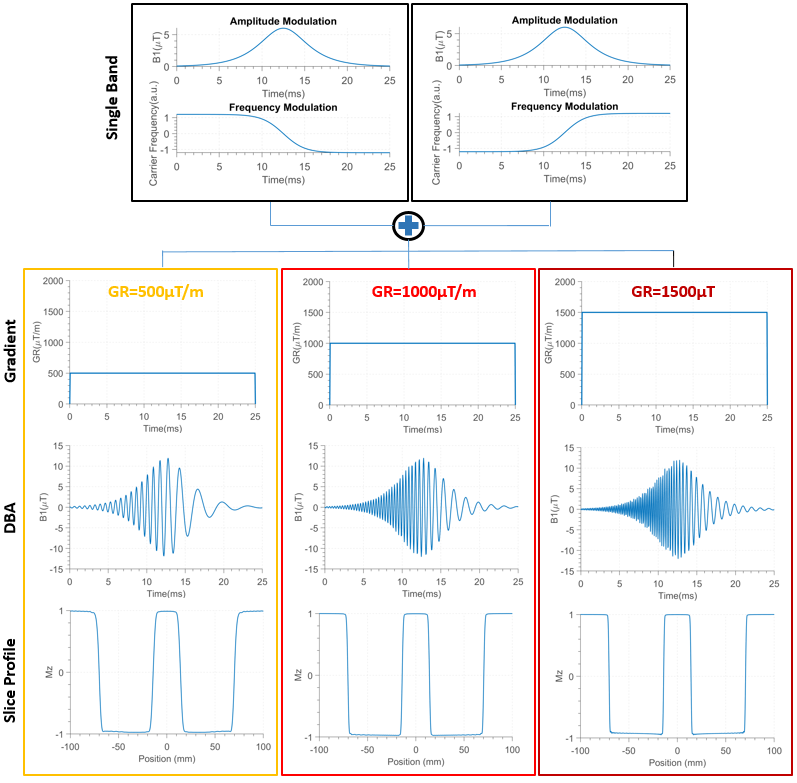
Fig1: Two hyperbolic secant adiabatic half passage pulses (top row), one of them time reversed, are combined to yield a DBA inversion pulse. Three DBA pulses (third row) are shown for different gradient strengths (second row) but constant pass/stop-band width.
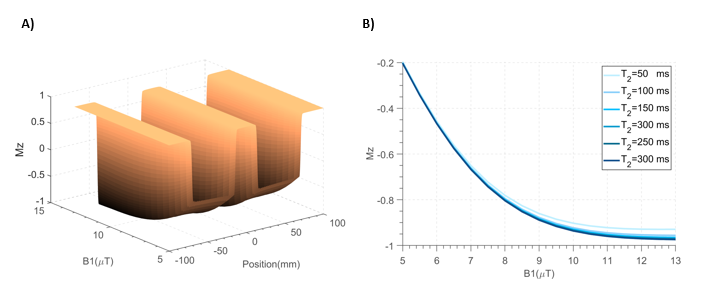
Fig2: A) Slice profile of the DBA inversion pulse as a function of the position and the B1+ amplitude, showing good resilience against B1 inhomogeneity. B) Inversion efficiency of the stop band for different B1+ amplitudes andT2 times, show negligible effect of the magnetization relaxation during the pulse.
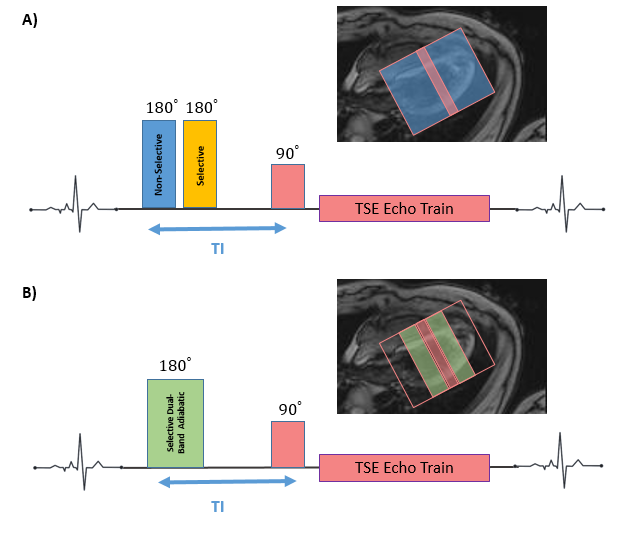
Fig3:Black-blood preparation scheme imaging sequence using A)double inversion recovery (DIR) or B) dual band adiabatic (DBA) Inversion, along with the slice geometry of the imaging slice, the inversion slans, and the stop bands of the DBA pulse
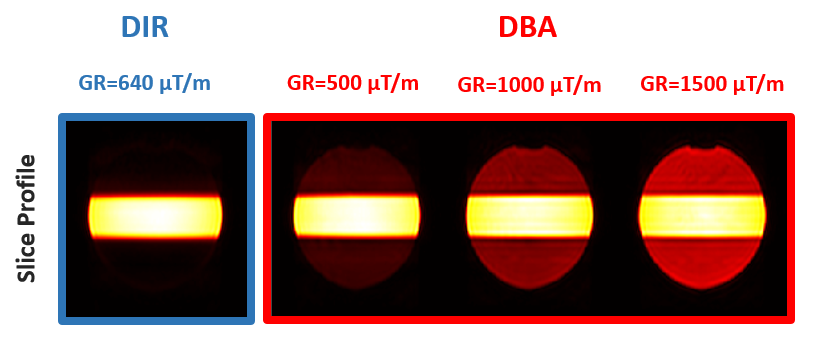
Fig4: Slice Profile of the DBA inversion pulse obtained in phantom experiments at different gradient strengths.
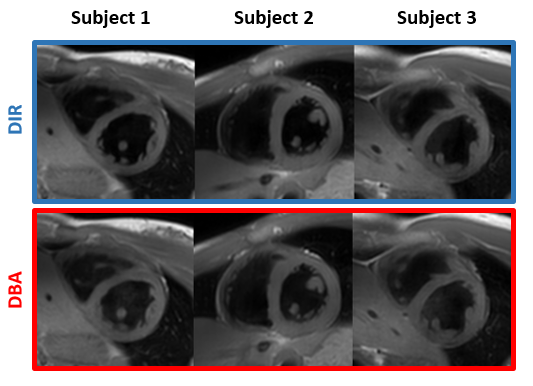
Fig5: Black-blood imaging obtained in three different volunteers using DIR or DBA inversion (DIR: thickness=26mm/DBA: thickness=28mm);
DOI: https://doi.org/10.58530/2023/4982