4936
Effect of acute ketamine on vigilance measured by multi-echo fMRI in treatment resistant major depression
Jennifer Evans1 and Carlos Zarate1
1NIH, Bethesda, MD, United States
1NIH, Bethesda, MD, United States
Synopsis
Keywords: Psychiatric Disorders, Drugs, major depression, ketamine
We investigate vigilance changes during intravenous ketamine administration in patients with treatment resistant major depression using an fMRI arousal template. There is a significant decrease in the average vigilance index after ketamine infusion as compared to placebo. The fMRI based vigilance index shows promise in detecting the rapid onset of ketamine administration effects.Introduction
Ketamine’s origins as an anesthetic with dissociative properties precede its discovery and development as a rapid acting antidepressant. Thus, to assess the signature of subanesthetic ketamine’s antidepressant action is important to also assess vigilance in these pharmacodynamic studies. Indeed, recent EEG (Chamadia, 2021) and EEG-fMRI (Zacharias, 2020) have investigated the induced functional connectivity and decreases in EEG vigilance after ketamine administration in healthy individuals. A newly developed template of alertness yields the ability to derive a vigilance index directly from fMRI data (Goodale, Elife, 2021). This template has been shown to correlate well with EEG and behavioral responses and track trial-to-trial variations in responses to sensory stimuli. Here we investigate vigilance changes during intravenous ketamine administration in patients with treatment resistant major depression using the fMRI arousal template.Methods
Twelve patients (mean age 35 years, [19-61])with treatment resistant major depression underwent a double-blind placebo cross-over trial where they received either a 40 minute infusion of either 0.5 mg/kg racemic ketamine or saline placebo while they were being scanned in a 3T Siemens Skyra scanner. There was one week between each infusion session. Heart rate was measured continuously with a pulse oximeter and respiration with a pneumatic belt and recorded with Biopac. Each session consisted of a 15 minute eyes closed resting state scan and a task acquired at: baseline, spanning the beginning of the infusion (starting after nominally 5 minutes) and during the continued infusion (from approximately 20-35 minutes) (see Fig 1.) – only the resting state scans is discussed here. Multi-echo fMRI data (3mm isotropic, TR: 2.08 s, TEs: 13,27,47 ms FA: , FA: 75 degrees) was preprocessed with afni_proc with slice-timing correction, motion alignment, registration to MNI space, and spatial smoothing to 4mm. Tedana (DuPre, 2021) was used for multi-echo denoising. After preprocessing and z-scoring, the fMRI vigilance timecourse for each scan was estimated by correlating a vigilance template (Goodale, 2020) with each volume of the scan on a TR-by-TR basis. The standard deviation of a continuous segment between 6-13 minutes was used to summarize the vigilance estimate for each scan.Results
Figure 2a illustrates vigilance timecourses for an example participant. There is an overall decrease in amplitude of the vigilance index during ketamine infusions as well as an increase in the frequency of oscillations as compared to placebo and the baseline scan. Figure 2b presents a summary of the estimate vigilance for each scan and infusion across all subjects (10) with a complete set of scans. There is a significant (p<0.001) decrease in the average vigilance index in the scan starting approximately 20 minutes after ketamine infusion which is does not occur after the placebo infusion. Comparable motion values were measured between paired ketamine and placebo scans suggesting that this result is not an effect of increased motion during drug administration.Conclusions
The fMRI based vigilance index shows promise in detecting the rapid onset of ketamine administration effects. Mediating factors such as ketamine response, motion and changes in heart rate and respiration need to be investigated.Acknowledgements
Funding for this work was provided by the Intramural Research Program at the National Institute of Mental Health, National Institutes of HealthReferences
DuPre et al., (2021) Journal of Open Source Software, 6(66),
Goodale, S, (2021) et al, eLife;10:e62376
Zacharias, N,(2020) et al., Hum Brain Mapp, Jan;41(1):107-119.
Chamadia, S 2021) et al., Clinical Neurophysiology,132(12):3010-3018
Figures
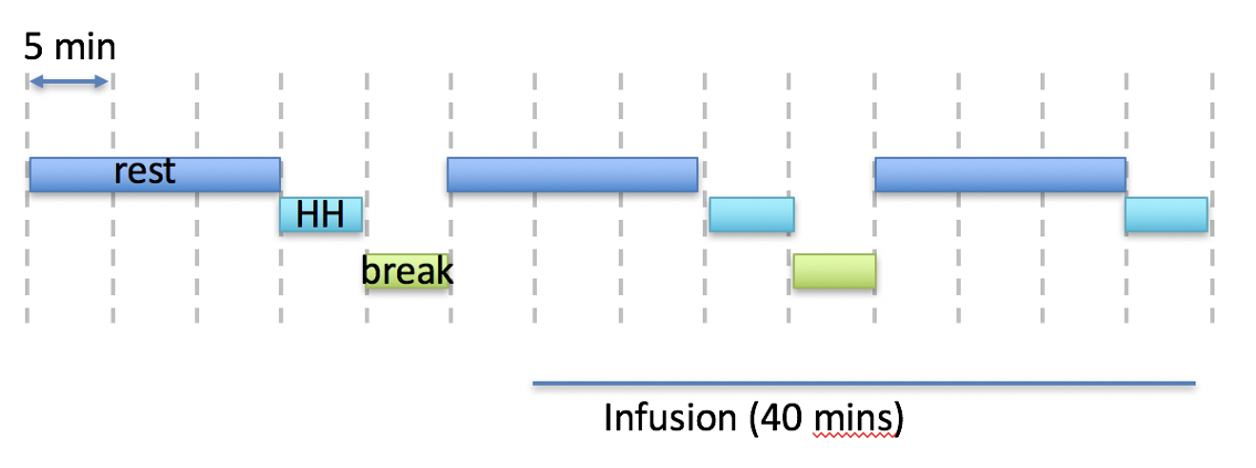
Nominal scan timing for each session indicating the eyes close resting state scans (rest in blue) and task (HH in green) with respect to the infusion. Each dashed line divider is 5 min.
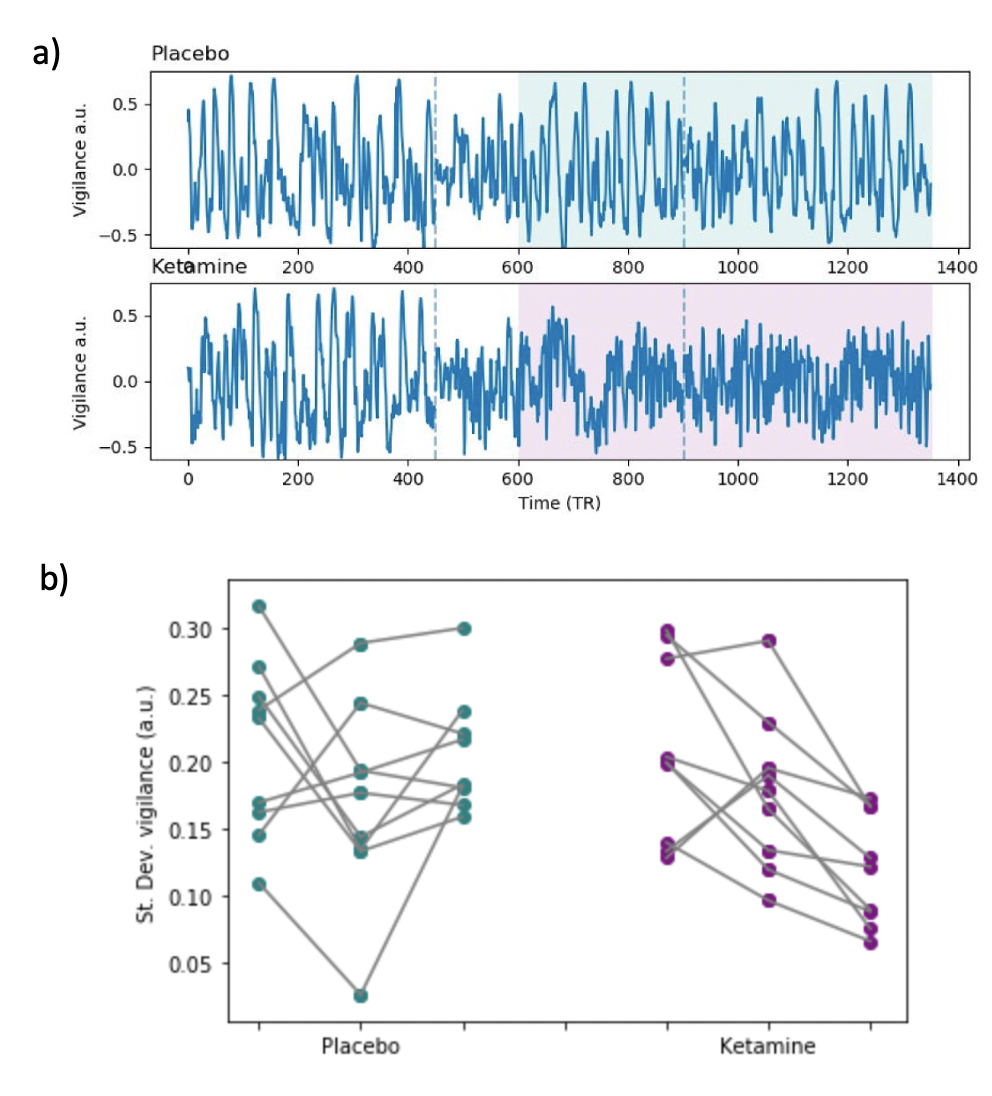
a) Example vigilance time series for placebo (top) and ketamine (bottom) infusion sessions. The three rest scans are shown concatenated and separated by vertical dotted lines. The timing of the infusion is indicated by the shaded area. b) Overall vigilance summary estimate for each participant across the 3 scans during either placebo (teal) or ketamine (purple) infusion.
DOI: https://doi.org/10.58530/2023/4936