4923
Deep learning-based pipeline to improve sharpness in knee imaging at both 1.5T and 3T: a clinical evaluation1Canon Medical Systems Corporation, Otawara, Japan, 2Canon Medical Systems France, Paris, France, 3Canon Medical Systems USA, Tustin, CA, United States
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Machine Learning/Artificial Intelligence
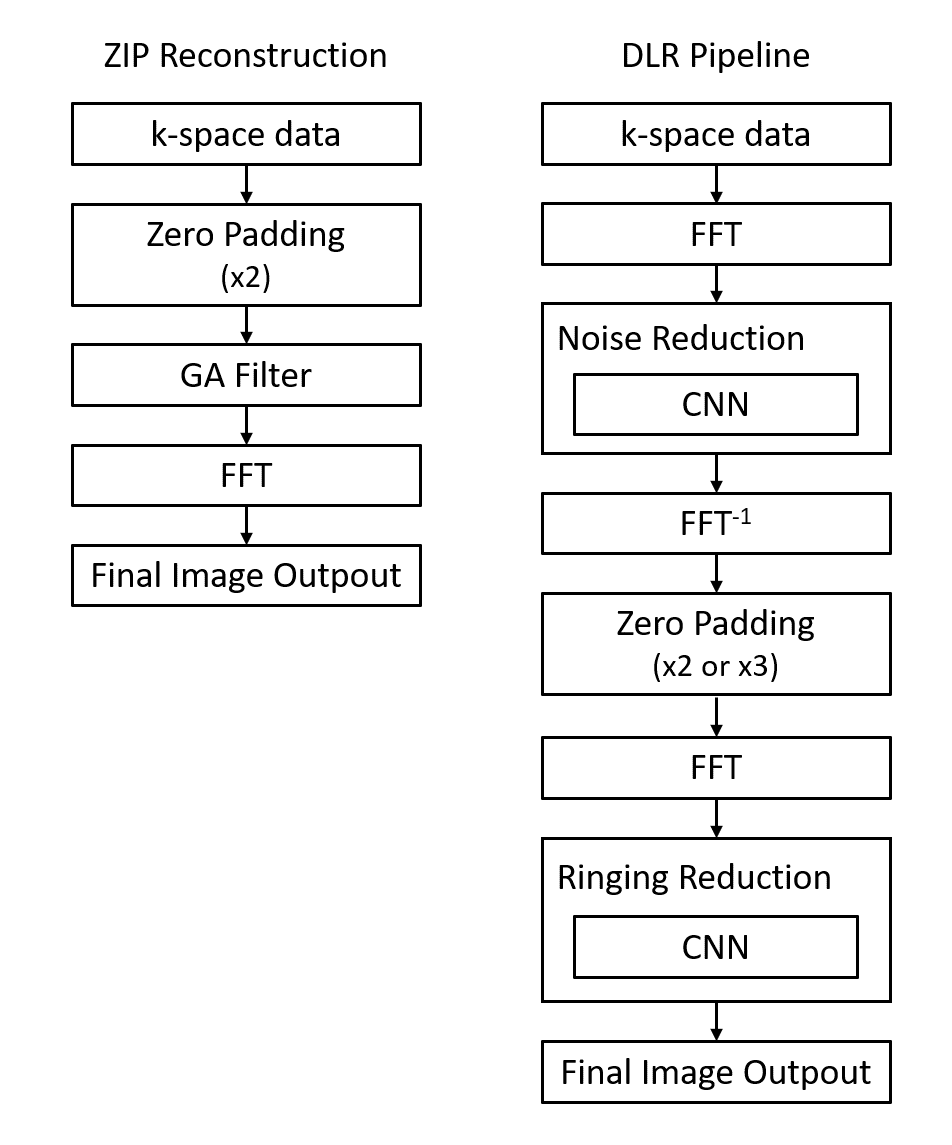
In MRI, edge sharpness is one of the main criteria to allow structure’s delineation and relevant clinical diagnosis. One way to improve the sharpness is to artificially increase the reconstructed matrix size with methods such as zero-padding interpolation (ZIP). In a previous study, we created a deep learning reconstruction (DLR) pipeline, combining ZIP with two CNN’s: the first one trained to reduce image noise, and the second one to reduce ringing artifacts. The goal of this work was to evaluate the clinical impact of this DLR pipeline on pathological knee images performed at 1.5T and 3T, compared to standard reconstructions.Introduction
In magnetic resonance imaging, edge sharpness is one of the main criteria to allow structure’s delineation and then relevant clinical diagnosis. One way to improve the sharpness is to increase the acquired matrix size but at a cost of a lower SNR or a longer scan time. Another option is to artificially increase the reconstructed matrix size with methods such as the widely used zero-padding interpolation (ZIP) [1], which expand the matrix size by filing the k-space extremities with zeros. For high upscaling factors, this process could lead to Gibbs ringing artifacts immediately adjacent to high-contrast interfaces [2], limiting the method to low factors. Several options could be additionally applied to reduce these artifacts. The most common one is to filter k-space data with a smoothly decreasing window (e.g Hamming or Tukey) prior to processing. More recently, convolution neural network (CNN) algorithms have been proposed to reduce them [3, 4]. In a previous study, we created a deep learning reconstruction (DLR) pipeline, combining ZIP with two CNN’s: the first one trained to reduce image noise, and the second one to reduce ringing artifacts. The goal of this work was to evaluate the clinical impact of this DLR pipeline allowing higher upscaling factor on pathological knee images performed at both 1.5T and 3T, compared to standard reconstructions and filters commonly used in routine.Method
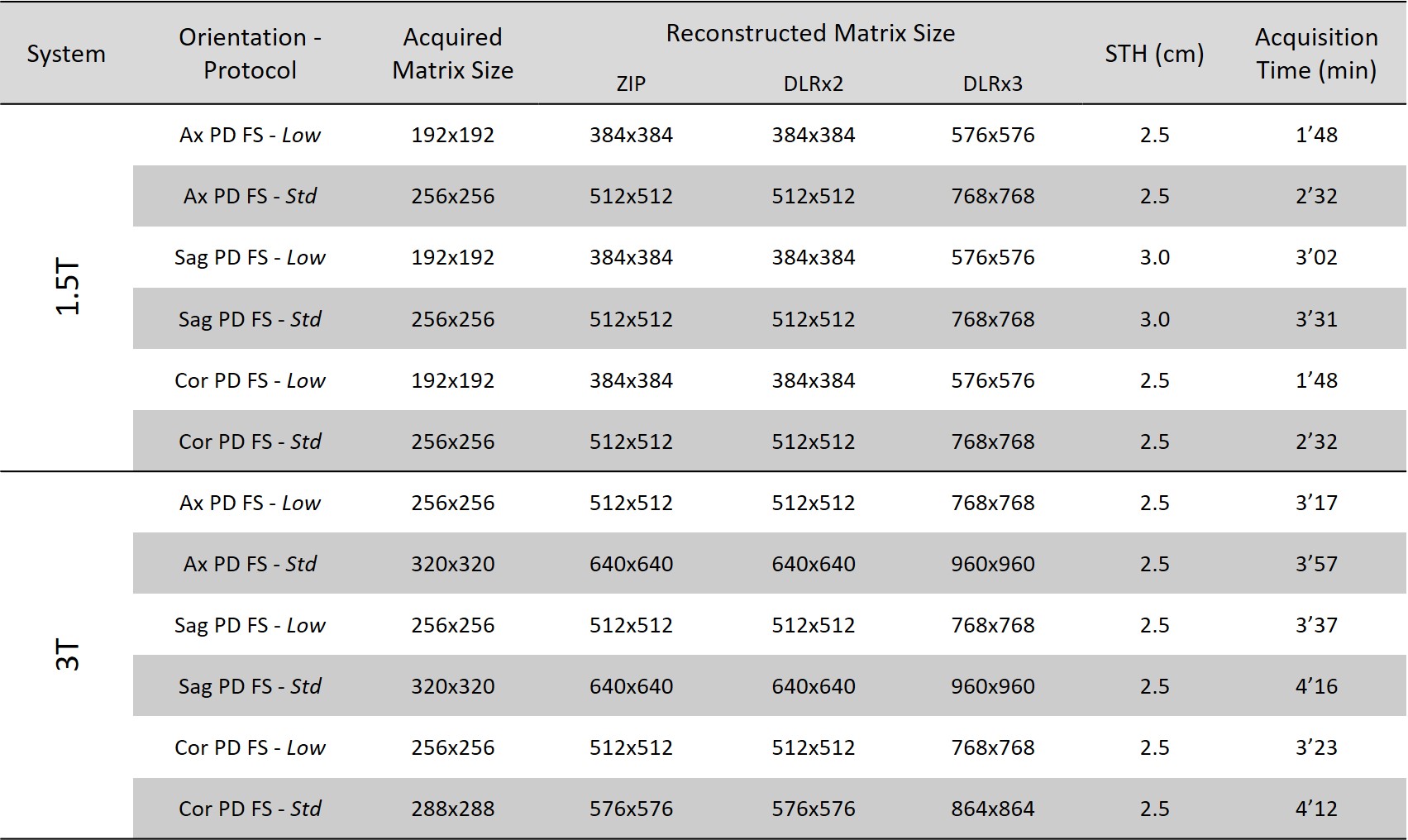
Imaging protocol and processing: Knee explorations were performed on 39 patients covering a breadth of clinical applications. They were scanned on 1.5T Vantage Orian XGO or Vantage Galan 3T XGO scanners (Canon Medical Systems Corporation, Tochigi, Japan) with dedicated knee coils. The study was approved by facilities’ institutional review board and informed consent was obtained from all subjects. Several 2D FSE scans with different phase direction have been performed at two resolutions: a standard one (Std), and a lower one (Low). All scans were reconstructed in two ways: with a ZIP method using an upscaling factor of 2 and an additional gain algorithm (GA) filter, and with the DLR pipeline using upscaling factors of 2 and 3 (Figure 1). Table 1 summarizes the main acquisition and reconstruction parameters.Data analysis: Datasets, in random order, were blindly evaluated by three board-certified radiologists, according to a modified Likert scale from 1 (“very poor”) to 5 (“excellent”). By definition, any value of 3 (“good”) or above indicates images could be considered as clinically acceptable. The scoring was segregated into several categories: imaging ringing, image sharpness, SNR, overall image quality, feature(s) conspicuity, and forced-ranking of the graded series per sequence. The reviewer scores were pooled by category and plotted as mean ± standard deviation. Three specific pairings have been selected to be compared (1) Low_DLRx2 vs Low_ZIP, (2) Low_DLRx3 vs Std_ZIP, and (3) Std_DLRx3 vs Std_ZIP. A pair-wise Wilcoxon signed rank test has been applied with a Bonferroni correction. Any p-value<0.017 would indicate a difference that is statistically significant
Results and discussion
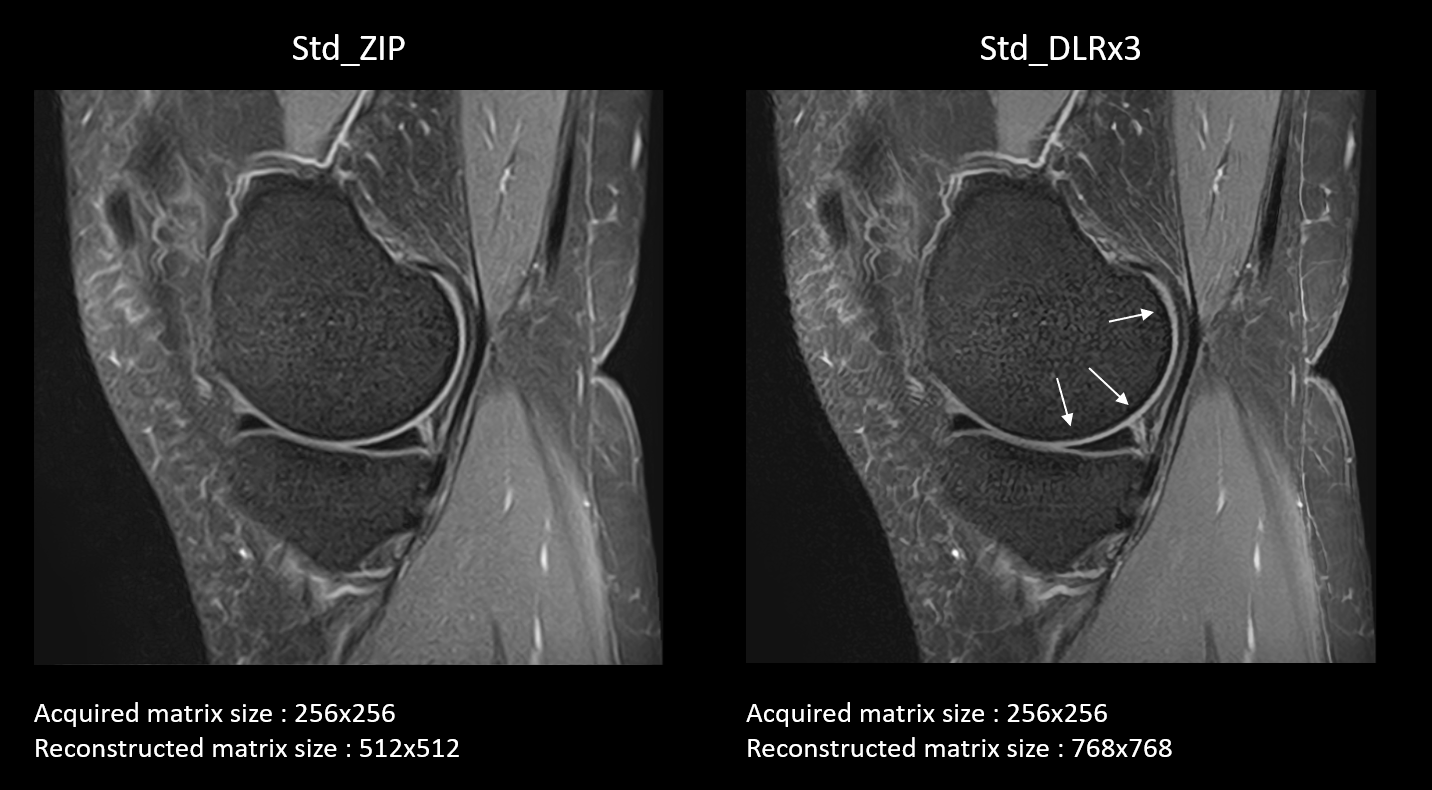
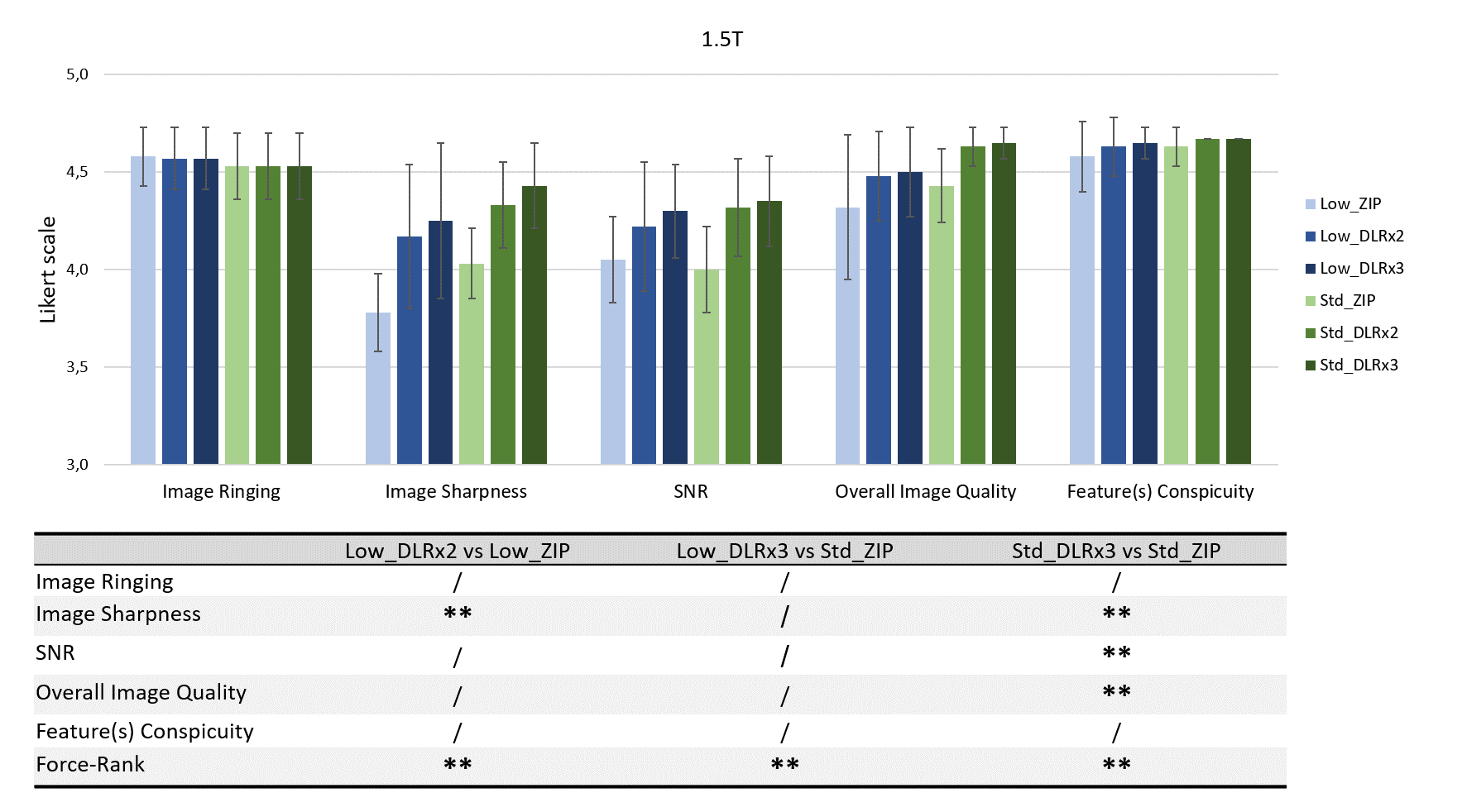
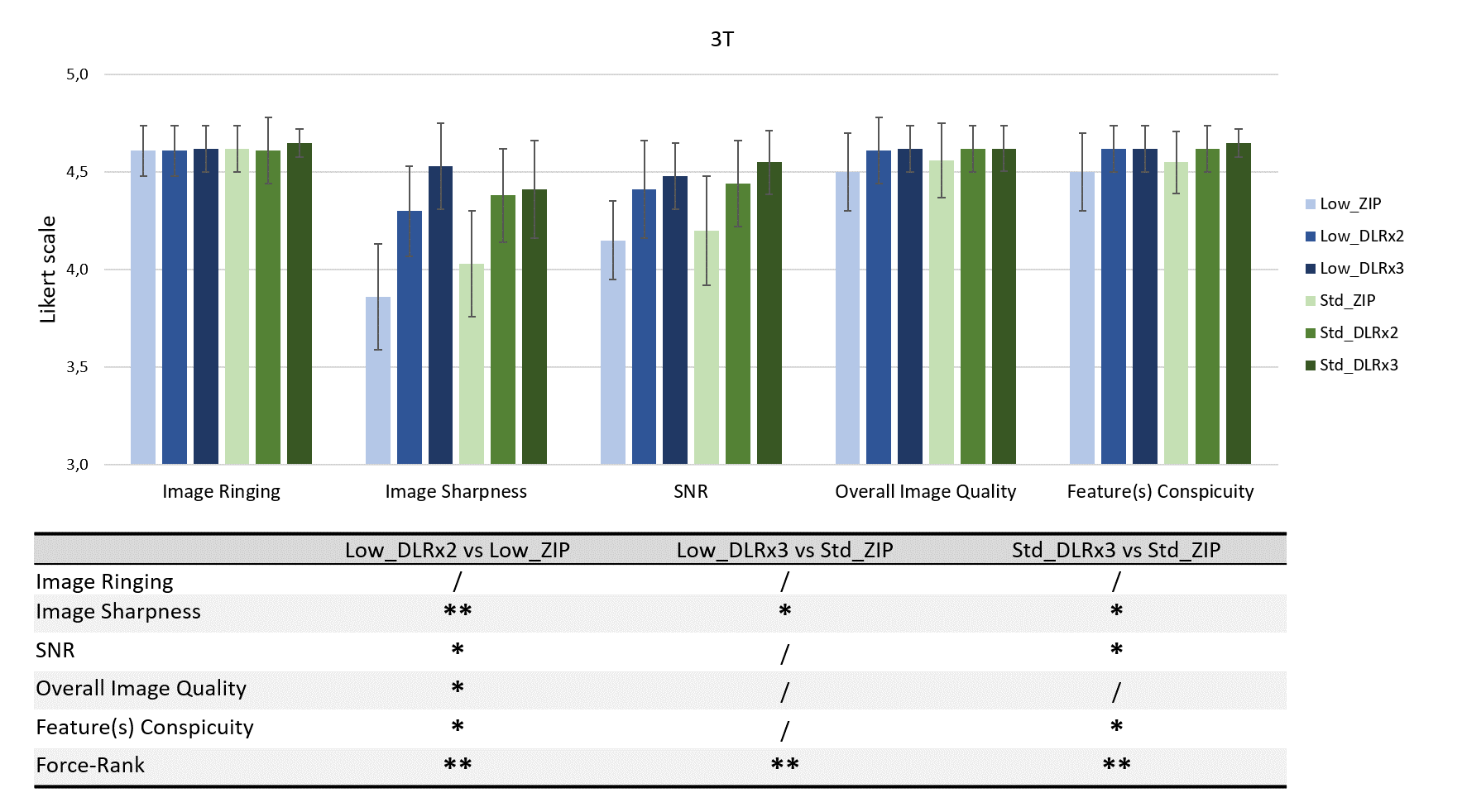
Typical images for the third pairing at 1.5T are shown in figure 2. Pooled scores and Wilcoxon analysis for 1.5T and 3T were plotted in figures 3 and 4, respectively. All images were ranked over score 3, meaning all were considered acceptable for clinical use. When comparing reconstructions for similar scans, performed with low (1st pairing: Low_DLRx2 vs Low_ZIP) or standard (3rd pairing: Std_DLRx3 vs Std_ZIP) acquisition matrix size, image sharpness and forced-ranking were significantly better for the DLR pipeline compared to the ZIP reconstruction, for both magnetic fields. For low matrix size acquisitions, more significant differences were found at 3T while for standard matrix size acquisitions, most scores were significantly different for both magnetic fields, highlighting the superiority of the DLR pipeline compare to the ZIP reconstruction. The second pairing (Low_DLRx3 vs Std_ZIP) was selected to evaluate if faster scans combined with the DLR pipeline could reach the same level of quality as ZIP. For this comparison, not many significant differences were found while forced-ranking was higher for DLR images. These results mean that fast scans with low acquisition matrix size and reconstructed with the DLR pipeline can reach the quality of standard scans and be preferred by radiologists. Finally, no difference in image ringing scores were identified in any of the 3 comparisons and for any fields. For this criterion, all images were scored between 4 and 5, meaning that very few Gibbs ringing artifacts were evident in the evaluated images. Additional study including ZIP reconstructions with upscaling factor of 3 would be needed to better evaluate the putative DLR pipeline superiority to reduce these artifacts further.Conclusion
The proposed DLR pipeline allowed higher upscaling factor without increasing Gibbs ringing artifact. For the two matrix sizes evaluated, image sharpness has been scored significantly higher for reconstructions performed with the DLR pipeline compare to those done with ZIP, at 1.5 and 3T. In addition, the three radiologists always ranked highest the DLR pipeline reconstructions compared to the conventional one. This DLR pipeline can be used in clinic and combined with standard scans to gain SNR and sharpness, or with fast scans to gain time without affecting the image quality and the clinical consistency.Acknowledgements
The authors would llike to thanks the Surgical Hospital at Southwoods (US) and the MIM group (Strasbourg, France) for their strong involvement with data collection.
References
1. Bernstein MA, Fain SB, Riederer SJ. Effect of windowing and zero-filled reconstruction of MRI data on spatial resolution and acquisition strategy. J Magn Reson Imaging. 2001 Sep;14(3):270–80.
2. Czervionke LF, Czervionke JM, Daniels DL, Haughton VM. Characteristic features of MR truncation artifacts. AJR Am J Roentgenol 1988; 151:1219-1228.
3. Zhao X, Zhang H, Zhou Y, Bian W, Zhang T, Zou X. Gibbs-ringing artifact suppression with knowledge transfer from natural images to MR images. Multimed Tools Appl. 2020 Dec 21;79(45–46):33711–33.
4. Wang Y, Song Y, Xie H, Li W, Hu B and Yang G. Reduction of Gibbs artifacts in magnetic resonance imaging based on Convolutional Neural Network. 10th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI), 2017
Figures