4907
Automatic localization of metal artifacts regions on MRI scout images1GE Healthcare, Bangalore, India, 2GE Healthcare, Niskayuna, NY, United States
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Artifacts, Metal implants
In MRI, presence of metal can cause blooming artifacts on MRI images. Automatically detecting the presence of metal and localizing it on the scout images itself can help streamline the MRI imaging workflow decisions downstream. In this work, we demonstrate a DL framework for hot spotting of metal/metal affected regions based on 2D three-plane MRI scout images of spine. The results indicate that the solution not only detects metal regions well on spine images (on which it was trained), but also is generalizable enough to work on other anatomies such as knee which was not part of the training data.Introduction
With MRI, presence of metal implants in patients can impact image quality. Hence the knowledge of presence of metal regions and its extent can help the technologist for scan planning, aid AI-based intelligent plane prescription workflow [1] and manual/automatic protocol selection [2]. Since scout images are the first set of images acquired for imaging setup, an algorithm which can accomplish metal detection on scout images is desirable in clinical practice. In this work, we describe a DL-based method for detection of metal regions directly using the 2D three-plane scout images to minimize any disruption in existing imaging workflow. We focused on the spine anatomy assuming that metal “hot-spotting” would help the choosing the appropriate method of multi-slice, multi-angle axial imaging [3]. We also describe ways to mitigate the rarity of cases having metal regions by leveraging high resolution T2 images and the corresponding masks in multiple ways to augment the training pool.Methods
Subjects: Spine & Knee MRI data for training and testing came from multiple clinical sites and approved by respective IRBs. A total of 1500 spine exams were considered. From these, total of 78 MRI exams which contained metal regions were included for further development. These were split into 58 in train set, 6 in validation and 12 in the test set. Additionally, two knee MRI exams with metal implants were also used to test the robustness of the model across anatomies. All the subjects were approved by the respective IRBs.MRI Data: All the data for the study came from 15 clinical sites with mix of 1.5T and 3T MRI systems (GEHC) with wide variety of imaging coils and covered multiple spine stations (Cervical, thoracic and lumbar) and overlap. We choose single shot, fast spin echo (SSFSE) scout images (only sagittal stack used) and Sagittal T2W images for the present study.
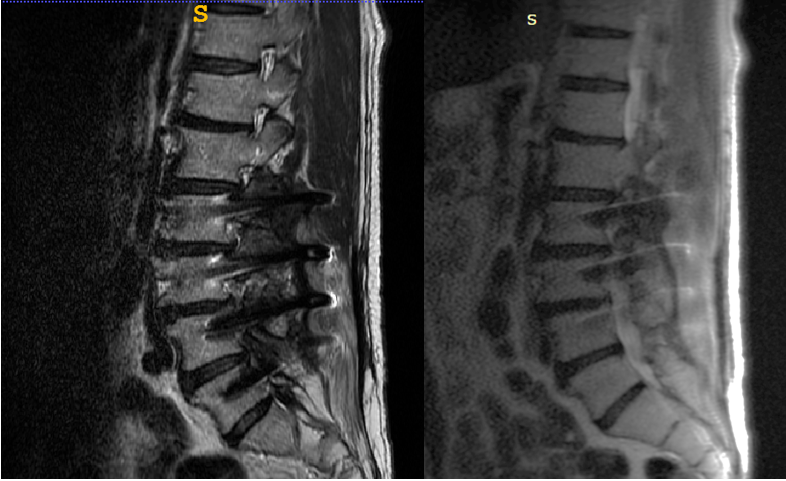
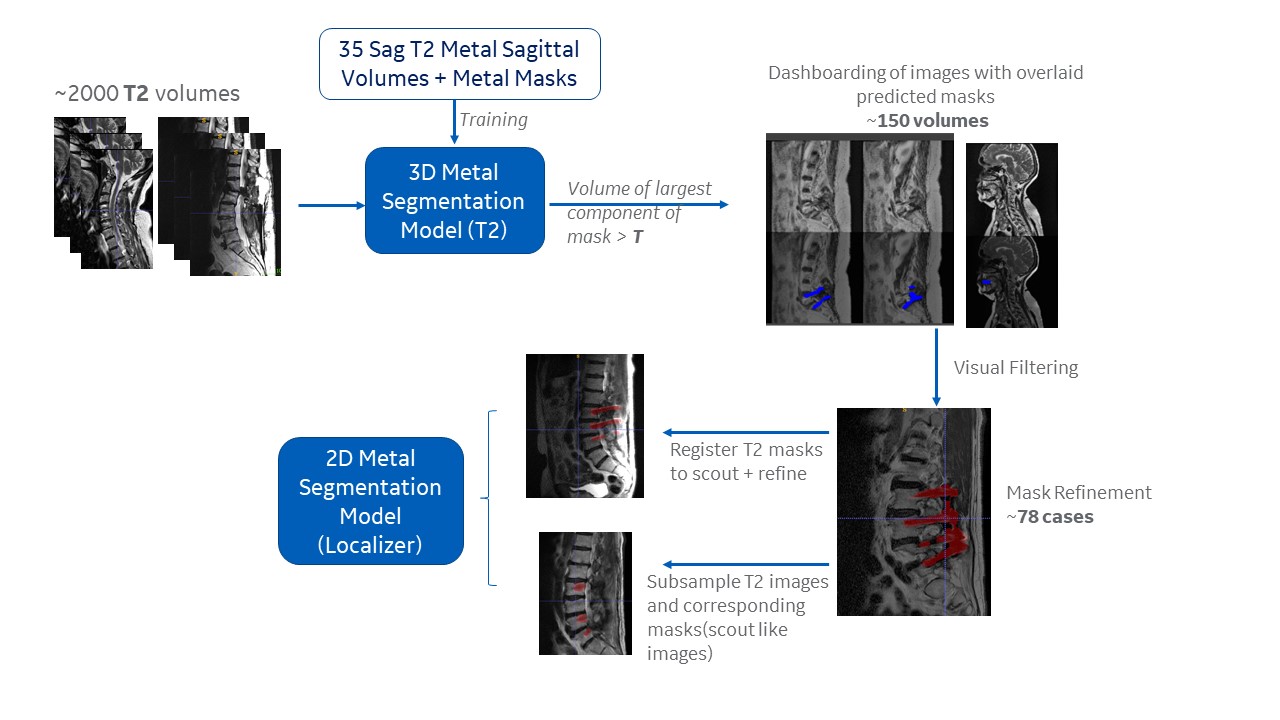
Metal Detection on Scout images: In addition to low prevalence of metal cases in our subject population, scout scans have thicker slices and consequently metal regions are visualized with lesser clarity as compared to the high-resolution images (Fig.1). Consequently, we took a multi-step approach for metal hot-spotting algorithm development (Fig 2):
a. From a small pool of manually identified metal impacted data, develop a deep learning model for metal detection on higher resolution Sagittal T2W data.
b. Use the initially trained model to search metal cases in larger pool of T2W Sagittal data and refine the metal regions as needed.
c. Finally, transfer the mask to scout images and create a train pool on expanded data using data augmentation.
From the initial small pool of data (400 cases), metal cases (~35) are manually identified and ground truth segmentation masks for metal regions were generated for high resolution T2W images. A 3D segmentation UNet model is trained using the selected T2 images and the corresponding ground truth masks. The model is then run on a larger pool of data (~1500) on the corresponding T2 images within them. As a first step, all cases where the metal region mask volume exceeds a particular threshold are selected as potential positives, this resulted in identifying around 150 cases. In the second filtering stage, a manual inspection of all potential positive cases, is performed and the false positives weeded out manually, resulting in a total of 78 metal cases. For all the final selected cases, a rigid registration was performed between T2W and 3-plane scout images using functionality provided in Elastix toolkit [4]. Accordingly, the metal segmentation masks were transferred from T2W data to corresponding scout images and a further manual refinement of the masks – resulting in scout image and its mask (set A). To expand the data pool, the T2W images and the corresponding masks as also appropriately resampled to simulate scout images – resulting in another set of images and its masks (set B). The data in Set A and B are combined to get the final set of images. The dataset then undergoes five-fold intensity based and geometric augmentation.
Deep Learning: A 2D UNet [5] is trained slice-wise with scout image as input and metal region mask as output using Dice loss, epochs = 100, ADAM optimizer and batch size = 5. The model with best validation loss was chosen for testing
Results and Discussion
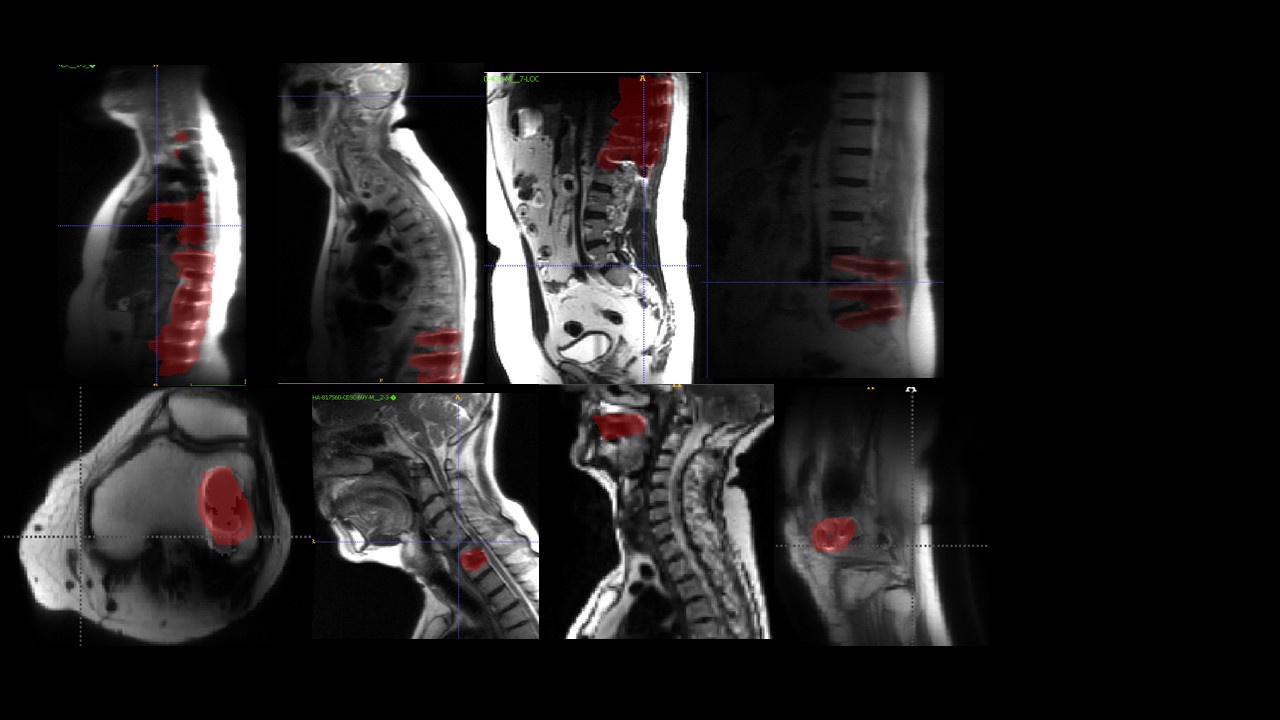
The scout metal hot-spotting model gives an average dice of 51% and can identify metal regions on all test cases (samples shown in Fig. 3). It is to be noted that the purpose of the metal identification is localization and not accurate pixelwise segmentation. We observe that the trained model can localize all the metal regions in the test cases. The salient features of the approach include ability to detect metal throughout the FOV (mostly spine cases, but still able to pick up dental implants in cervical spine exams). See Fig 3 where metal hot-spotting could be performed even on knee MRI cases; even though knee data were not included in the training pool. Since the metal blooming artifact manifest in a similar manner, the method is generalizable across anatomies.Acknowledgements
No acknowledgement found.References
[1] Intelligent Knee MRI slice placement by adapting a generalized deep learning framework, ISMRM 2020
[2] MRI After Arthroplasty: Comparison of MAVRIC and Conventional Fast Spin-Echo Techniques, Catherine L. Hayter, Matthew F. Koff, Parina Shah, Kevin M. Koch, Theodore T. Miller, and Hollis G. Potter, American Journal of Roentgenology 2011 197:3, W405-W411
[3] Multi Angle Oblique, https://www.mr-tip.com/serv1.php?type=db1&dbs=Multi+Angle+Oblique
[4] Klein, S., Staring, M., Murphy, K., Viergever, M.A. and Pluim, J.P., 2009. Elastix: a toolbox for intensity-based medical image registration. IEEE transactions on medical imaging, 29(1), pp.196-205.
[5] Ronneberger, O., Fischer, P. and Brox, T., 2015, October. U-net: Convolutional networks for biomedical image segmentation. In International Conference on Medical image computing and computer-assisted intervention (pp. 234-241). Springer, Cham.
Figures