4866
Left ventricular layer-specific strain predicts pulmonary arterial hypertension long-term prognosis1State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd, Beijing, China, 3Magnetic Resonance, Siemens Healthcare, Erlangen, Germany, 4Emergency Center, State Key Laboratory of Cardiovascular Disease, Key Laboratory of Pulmonary Vascular Medicine, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 5Center of Pulmonary Vascular Disease, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
Keywords: Heart, Data Processing, Strain
Studies have reported left ventricular (LV) dysfunction was associated with more severe disease and poorer prognosis in pulmonary arterial hypertension (PAH). However, there are only few studies that evaluated LV strain abnormalities using cardiovascular magnetic resonance (CMR) in PAH patients. This is the first study to describe the distribution pattern and prognostic values of LV layer-specific strain/strain rate in PAH patients using a deformation registration algorithm (DRA) based on CMR. It’s found that CMR derived LV layer-specific strain could predict long-term prognosis in PAH patients.Introduction
Though right ventricular function is considered as a determining factor of prognosis in pulmonary arterial hypertension (PAH) patients, left ventricular (LV) function can also be affected by PAH. Studies have reported LV dysfunction was associated with more severe disease and poorer prognosis in pulmonary hypertension 1,2. However, there are only few studies that evaluated LV multi-layer strain abnormalities using cardiovascular magnetic resonance (CMR) in PAH patients. Thus, this study investigated the layer-specific LV strain pattern and its prognosis value in PAH patients using a deformation registration algorithm (DRA) based on CMR.Method
82 newly-diagnosed PAH patients were enrolled from a real-world observation based Chinese national prospective multi-center observational registry study between January 2011 and December 2017. The median follow-up time was 2014 days (range from 26 to 3990 days). All enrolled patients received right heart catheterization (RHC) and CMR scanning within one week at the baseline. CMR was performed on a 1.5T scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Breath-hold short-axis cine images encompassing the whole left ventricle (LV) and RV from apex to base were acquired using balanced steady-state free-precession (bSSFP) sequence (repetition time/echo time, 3.2 ms/1.6 ms; temporal resolution, 34 ms; flip angle, 60 degrees; field of view, 280 x 340 mm2; matrix, 150 x 256; voxel size, 1.9mm x 1.3mm; slice thickness, 8 mm). Acquired CMR images were analyzed using a prototype software V2.1 (Trufi Strain, Siemens Healthcare, Princeton, USA). This software uses a deformation registration algorithm to calculate the myocardial strain on a pixel basis, which could be used to analyze the layer-specific strain and strain rate based on cine CMR (DRA-CMR). In this research, LV Peak Strain, Peak Systolic Strain Rate (SSR), Peak Early Diastolic Strain Rate (DSRE), Peak Late Diastolic Strain Rate (DSRL) in the radial, circumferential and longitudinal direction were studied on LV three layers [endocardial wall (ew), middle wall (mw) and epicardial wall (epiw)] and the whole LV myocardium.Results
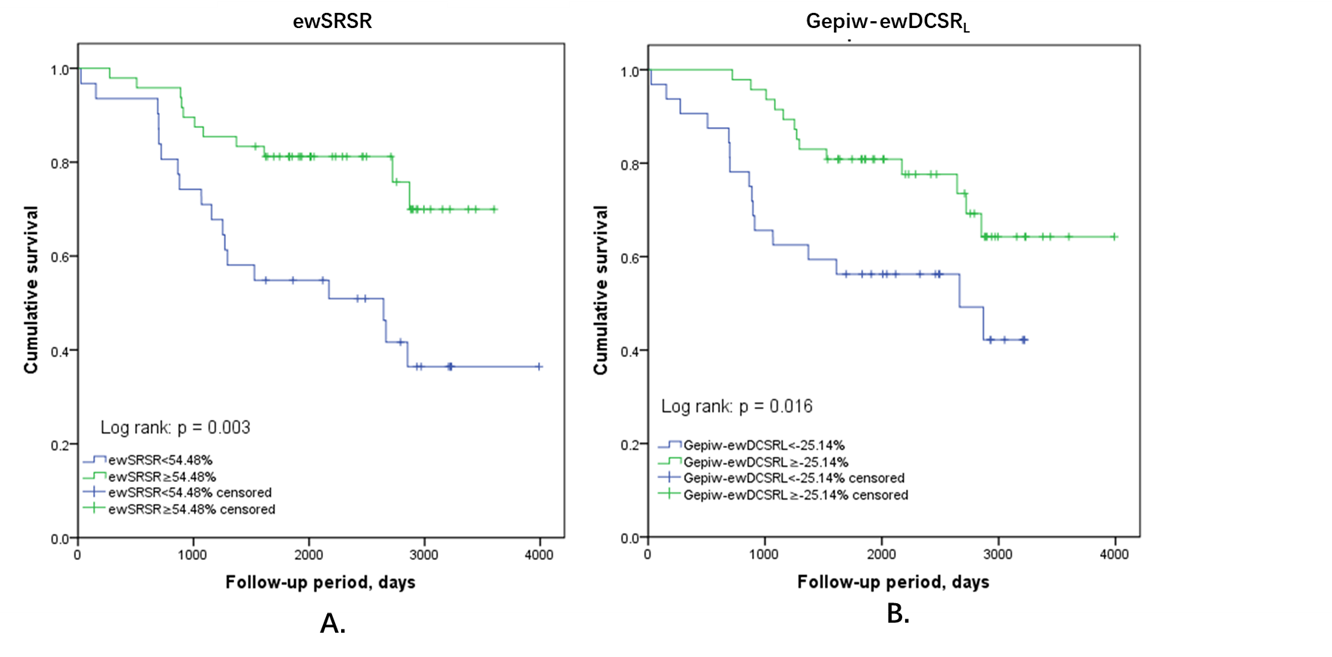
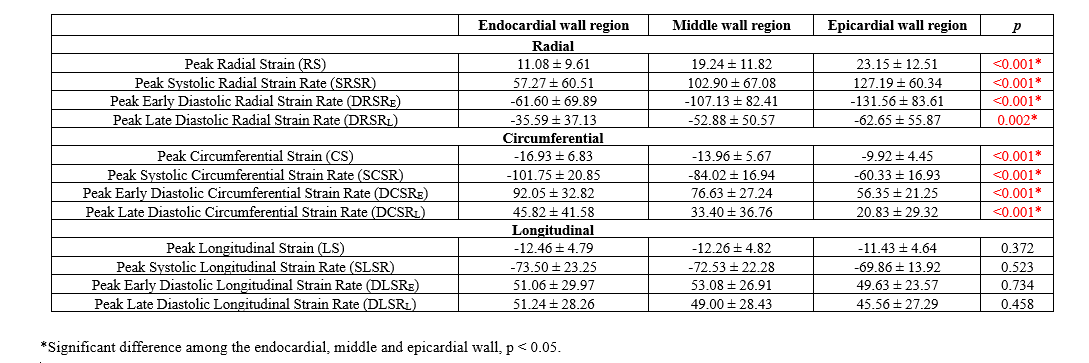
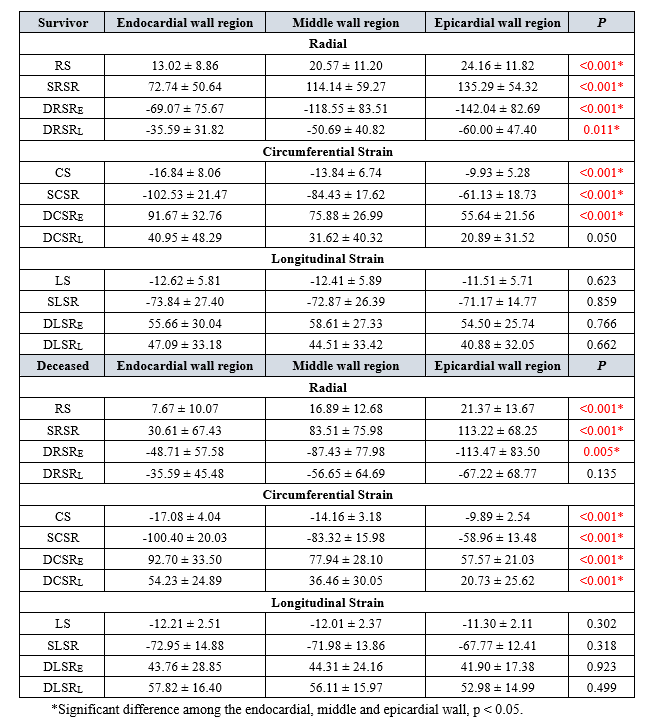
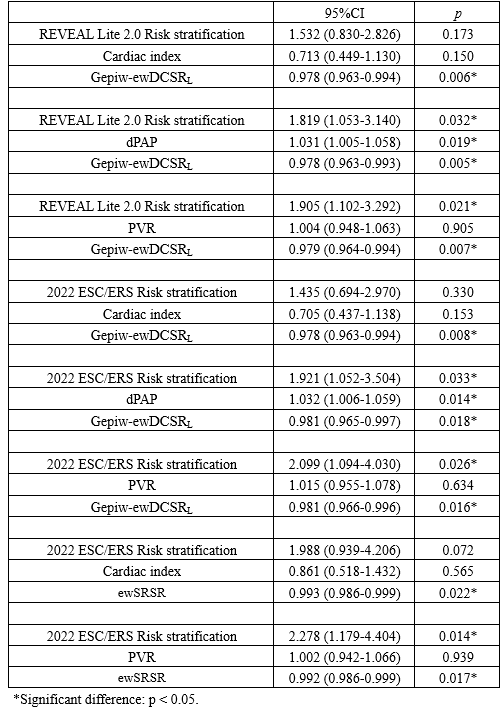
In the radial direction, obvious increasing transmural gradients from endocardial to epicardial wall were found in Peak Radial Strain (RS), Peak Systolic Radial Strain Rate (SRSR), Peak Early Diastolic Radial Strain Rate (DRSRE) and Peak Late Diastolic Radial Strain Rate (DRSRL) within LV (Table 1). In the circumferential direction, decreasing transmural gradients from endocardial to epicardial wall were found in Peak Circumferential Strain, Peak Systolic Circumferential Strain Rate, Peak Early Diastolic Circumferential Strain Rate and Peak Late Diastolic Circumferential Strain Rate (DCSRL) within LV. However, in the longitudinal direction, no obviously homogeneous transmural gradients were found among three layers. Comparisons between survival and deceased patients showed the increasing transmural gradient from endocardial to epicardial wall in DRSRL was not heterogenous in deceased patients (Table 2). Univariate Cox regression analysis found LV endocardial wall (ew)-RS, ewSRSR, middle wall- Peak Early Diastolic Longitudinal Strain Rate (DLSRE), epicardial wall-DLSRE and transmural gradient (Gepiw-ew) of DCSRL were risk factors of long-term mortality. Multivariate Cox regression analysis found Gepiw-ewDCSRL and ewSRSR could were still risk factors of long-term mortality after adjusted by functional and haemodynamics parameters (Table 3). Kaplan-Meyer curve displayed PAH patients with ewSRSR<54.48% (log-rank: p=0.003) or Gepiw-ewDCSRL<-25.14% (log-rank: p=0.016) had worse long-term prognosis (Figure 1).Discussion
Strain is a quantitative measure of myocardial deformation. Liu`s study reported in normal people, only circumferential strain had obvious transmural gradient within LV3. However, our study found PAH patients had homogeneous transmural gradients both in LV radial and circumferential strain. In addition, deceased PAH patients had altered DRSRL distribution pattern than survivors at the baseline. LV layer-specific ewSRSR and Gepiw-ewDCSRL both of which reflect LV systolic function, could indicate long-term PAH prognosis. Therefore, LV layer-specific strain rate at baseline might reflect the severe level of myocardial damage.Conclusion
CMR derived LV layer-specific ewSRSR and Gepiw-ewDCSRL could predict long-term prognosis in PAH patients.Acknowledgements
This study was supported by grants from National Key Research and Development Program of China (No. 2016YFC1304400) and Youth Found of Fuwai Hospital (Grant number: 2022-FWQN06).References
1. Brauchlin AE, Soccal PM, Rochat T, Spiliopoulos A, Nicod LP, Trindade PT. Severe left ventricular dysfunction secondary to primary pulmonary hypertension: bridging therapy with bosentan before lung transplantation. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation. 2005; 24(6):777–780.
2. Pielsticker EJ, Martinez FJ, Rubenfire M. Lung and heart-lung transplant practice patterns in pulmonary hypertension centers. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation. 2001; 20(12):1297–1304.
3. Liu H, Yang D, Wan K, et al. Distribution pattern of left-ventricular myocardial strain analyzed by a cine MRI based deformation registration algorithm in healthy Chinese volunteers. Sci Rep 2017;7:45314.
Figures