4862
DRA-CMR based layer-specific right ventricle strain predicts pulmonary arterial hypertension prognosis: results from a Chinese registry study1State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd, Beijing, China, 3MR Collaboration, Siemens Healthineers Ltd, Shanghai, China, 4Magnetic Resonance, Siemens Healthcare, Erlangen, Germany, 5Emergency Center, State Key Laboratory of Cardiovascular Disease, Key Laboratory of Pulmonary Vascular Medicine, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 6Center of Pulmonary Vascular Disease, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
Keywords: Heart, Heart, Strain, Right ventricle
This is the first study to demonstrate that right ventricle (RV) layer-specific strain rate measured by deformation registration algorithm based cardiovascular magnetic resonance had the long-term and 3-year mortality predictive values in pulmonary arterial hypertension (PAH) patients. Our findings indicated that RV layer-specific strain rate may be sensitive indicators of RV dysfunction in PAH.Introduction
Pulmonary arterial hypertension (PAH) could lead to right ventricle (RV) myocardial fiber orientation and result in RV deformation1,2. Deformation registration algorithm (DRA) based strain analysis software is a novel post-processing technique to quantify myocardial deformation by analyzing layer-specific strain and strain rate based on cardiovascular magnetic resonance (CMR)3. However, RV layer-specific strain measured by CMR and their prognostic values in PAH have not been explored. Thus, this study aimed to investigate the prognostic values of layer-specific strain in PAH using DRA-CMR.Method
As a sub-cohort from a real-world observation based Chinese national prospective multi-center observational registry study4, newly diagnosed PAH patients were prospectively recruited between January 2011 and December 2017. The designed primary endpoint was any causes of mortality, lung transplantation or atrial septostomy. Each patient was followed by telephone, outpatient or in hospital examinations in a 6-month interval. All enrolled patients received right heart catheterization (RHC) and CMR scanning within one week at the baseline. The hemodynamic criteria for PAH were mean pulmonary arterial pressure (mPAP) ≥ 25 mmHg, pulmonary capillary wedge pressure (PCWP) < 15 mmHg and pulmonary vascular resistance (PVR) > 3 Wood Units measured at rest by RHC. CMR was performed on a 1.5T scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Breath-hold short-axis cine images encompassing the whole left ventricle (LV) and RV from apex to base were acquired using balanced steady-state free-precession (bSSFP) sequence (repetition time/echo time, 3.2 ms/1.6 ms; temporal resolution, 34 ms; flip angle, 60 degrees; field of view, 280 x 340 mm2; matrix, 150 x 256; voxel size, 1.9mm x 1.3mm; slice thickness, 8 mm). Acquired CMR images were analyzed using a prototype software V2.1 (Trufi Strain, Siemens Healthcare, Princeton, USA). This software uses a deformation registration algorithm to calculate the myocardial strain on a pixel basis, which could be used to analyze the layer-specific strain and strain rate based on cine CMR (DRA-CMR). In this research, RV Peak Strain, Peak Systolic Strain Rate (SSR), Peak Early Diastolic Strain Rate (DSRE), Peak Late Diastolic Strain Rate (DSRL) in the radial, circumferential and longitudinal direction were studied on RV three layers [endocardial wall (ew), middle wall (mw) and epicardial wall (epiw)] and the whole RV myocardium. The representative radial strain and strain rate analysis results were shown in Figure.1.Results
82 newly-diagnosed PAH patients were enrolled and the median follow-up time was 2014 days (range from 26 to 3990 days). During the follow-up, no patient received lung transplantation or atrial septostomy and no patients were lost to follow up. 29 (35.37%) patients had all-caused death at the end of this study. Kaplan-Meyer curves showed RV layer-specific Peak Late Diastolic Circumferential Strain Rate (DCSRL), Peak Late Diastolic Radial Strain Rate (DRSRL) and Peak Systolic Longitudinal Strain Rate (SLSR) could predict the long-term mortality of PAH patients(Figure. 2). DCSRL and Peak Early Diastolic Longitudinal Strain Rate (DLSRE) were indictors of 3-year mortality. Combined layer-specific strain rate parameters could reclassify PAH patients who were in 2015 ESC/ERS low and intermediate risk groups into three distinct risk groups. Patients with endocardial wall (ew)-DRSRL <-67.97% + ewDCSRL ≥28.70% or middle wall (mw)-DRSRL <-76.03% + mwDCSRL ≥21.79% or myocardial region (m)-DRSRL <-79.84% + mDCSRL ≥22.36% presented the worst long-term prognosis.Discussion
RV has both systolic and diastolic functions. This study found that it seems only SLSR which reflects RV systolic functions could indicate prognosis. In contrast, baseline DRSRL, DCSRL and DLSRE, which all reflect RV diastolic function, were also predictors of PAH prognosis. Therefore, more attention should be paid to RV diastolic function5. Compared with traditional PAH risk stratification, combined layer-specific strain rates which reflected RV transverse wall motion abilities, could detect the early RV myocardial impairment which might not lead to apparent clinical RV dysfunction symptoms, but would result in bad long-term prognosis. Therefore, we speculated that layer-specific strain rate analysis can assess RV function more precisely.Conclusion
RV layer-specific strain rate quantified by DRA-CMR had the ability to predict long-term and 3-year mortality and were precise and sensitive indicators of RV dysfunction in PAH patients.Acknowledgements
This study was supported by grants from National Key Research and Development Program of China (No. 2016YFC1304400) and Youth Found of Fuwai Hospital (Grant number: 2022-FWQN06).References
1. Pettersen, E. et al. Contraction Pattern of the Systemic Right Ventricle. Shift From Longitudinal to Circumferential Shortening and Absent Global Ventricular Torsion. J. Am. Coll. Cardiol. 49, 2450–2456 (2007).
2. Kind, T. et al. Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J. Cardiovasc. Magn. Reson. 12, 1–11 (2010).
3. C. Guetter, H. Xue, C. Chefd’Hotel, J. Guehring, “Efficient symmetric and inverse-consistent deformable registration through interleaved optimization”, ISBI 2011
4. Quan, R. Characteristics , goal-oriented treatments and survival of pulmonary arterial hypertension in China : Insights from a national multicentre prospective registry. 1–12 (2022)
5. Trip, P. et al. Clinical relevance of
right ventricular diastolic stiffness in pulmonary hypertension. Eur. Respir.
J. 45, 1603–1612 (2015).
Figures
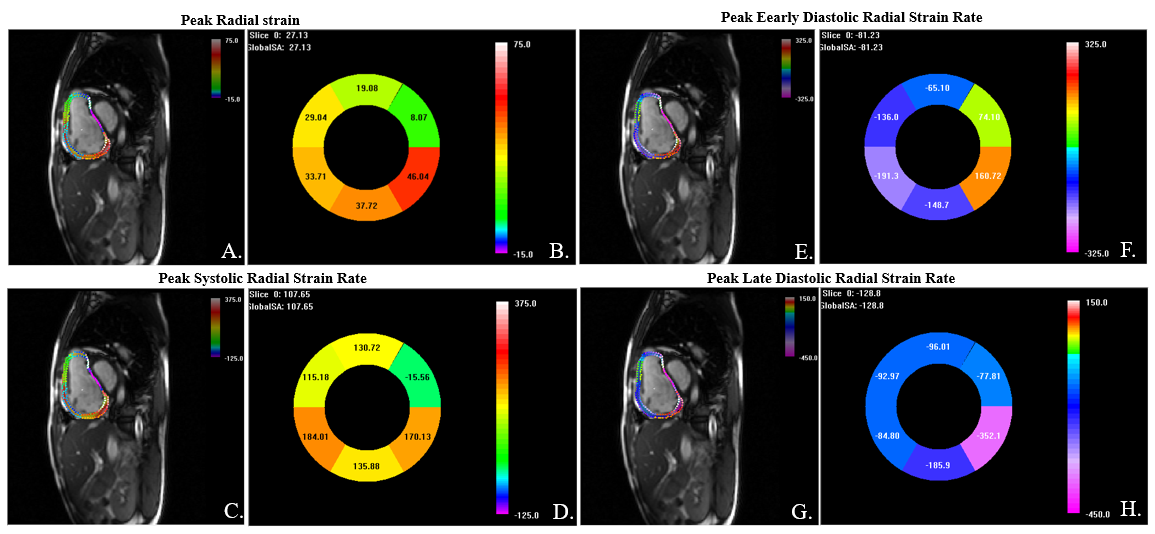
Figure 1. Right ventricle layer-specific radial strain and strain rate analysis by DRA-CMR.
The Trufi-strain software would track the endocardial and epicardial contours throughout a cardiac cycle automatically and divided the myocardium into three layers. Strain and strain rate values are shown in situ on three layers (A, C, E, G). Strain and strain rate values of six segments are shown in the “Bull’s eye” (B, F, D, H).
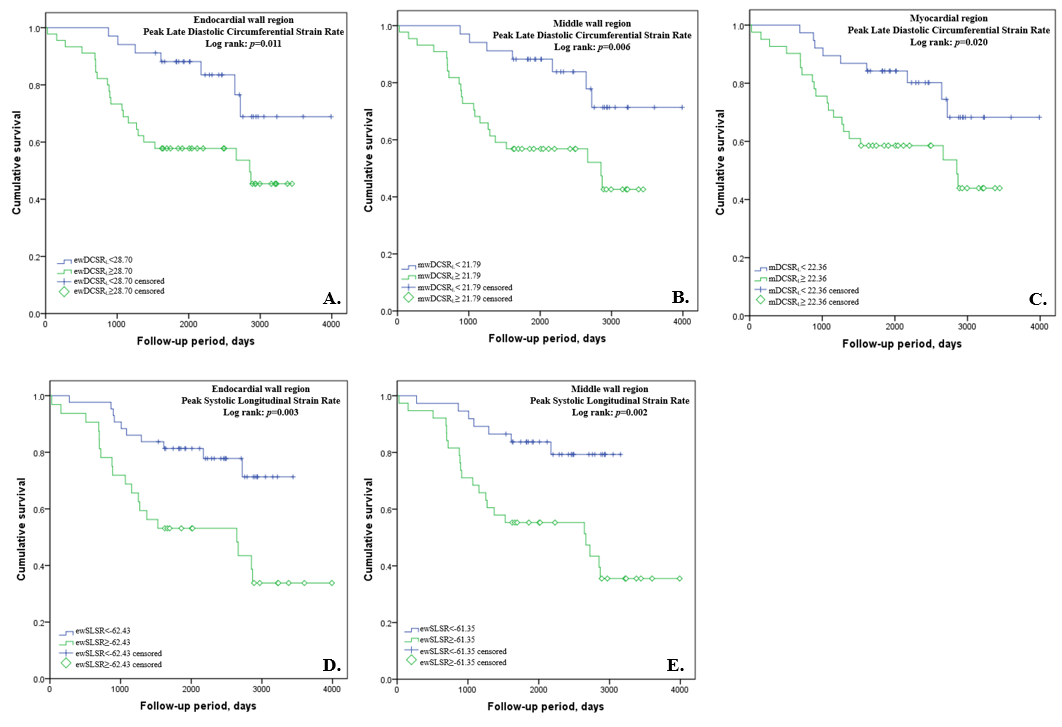
Figure 2. Kaplan-Meyer curves showed right ventricle layer-specific DCSRL and SLSR could predict the long-term mortality of PAH patients.
PAH patients with ewDCSRL ≥28.70% (A), mwDCSRL ≥21.79% (B) or mDCSRL ≥22.36% (C) had worse long-term prognosis. PAH patients with ewSLSR≥-62.43% (D) or mwSLSR≥-61.35% (E) also had worse long-term prognosis. Endocardial wall(ew), middle wall (mw), myocardial region (m), Peak Late Diastolic Circumferential Strain Rate (DCSRL), Peak Late Diastolic Radial Strain Rate (DRSRL) and Peak Systolic Longitudinal Strain Rate (SLSR).