4851
Left Atrial Circumferential Strain for Evaluation of Mitral Regurgitation: A Feasibility and Reproducibility Study1Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Radiology, Stanford University, Stanford, CA, United States, 3Digital Technology and Innovation, Siemens Healthineers, Erlangen, Germany, 4Cardiothoracic Radiology, University Hospital of Basel, Basel, Switzerland
Synopsis
Keywords: Myocardium, Valves, strain
Short-axis CMR left atrial (LA) circumferential strain has not yet been investigated as a cardiac biomarker. This study assessed feasibility and reproducibility of LA circumferential strain in a healthy cohort, examined changes in strain within mitral regurgitation (MR) patients, and assessed correlations between reproducible strain measures and MR severity and cardiac function. Reservoir strain globally and at superior and mid LA regions was found to be reproducible, was significantly different between healthy volunteers and MR patients, and was correlated with cardiac function. CMR LA circumferential strain is reproducible with potential utility in evaluating impaired LA mechanics in MR patients.
Background
Mitral regurgitation (MR) is the most prevalent valvular disease. Monitoring MR severity is critical for guiding management1. Left atrial (LA) strain is a measure of LA deformation and has been shown to be a useful biomarker of impaired cardiac mechanics2. Strain can be quantified retrospectively from cine steady-state free-precession (SSFP) cardiac MRI (CMR) through feature-tracking (FT). To assess complex cardiac deformations, strain is quantified over three principal directions: radial, longitudinal, and circumferential. Clinical CMR exams typically include long-axis cine SSFP (LAX) images, which cover both left ventricle (LV) and LA, enabling FT LA longitudinal and radial strain calculation. However, circumferential strain requires short-axis views (SAX) to measure circumferential deformation. Since routine short-axis cine SSFP exams are for LV evaluation, they do not typically cover the LA. Thus, feasibility and clinical utility of CMR circumferential LA strain remains unknown. The aims of this study were to assess 1) feasibility and test-retest reproducibility of global and regional LA FT circumferential strain from cine SAX SSFP; 2) test utility of identified reproducible circumferential LA strain parameters in quantifying differences between MR patients and healthy volunteers; 3) correlation of reproducible LA circumferential strain parameters with MR severity and cardiac function in MR patients.Methods
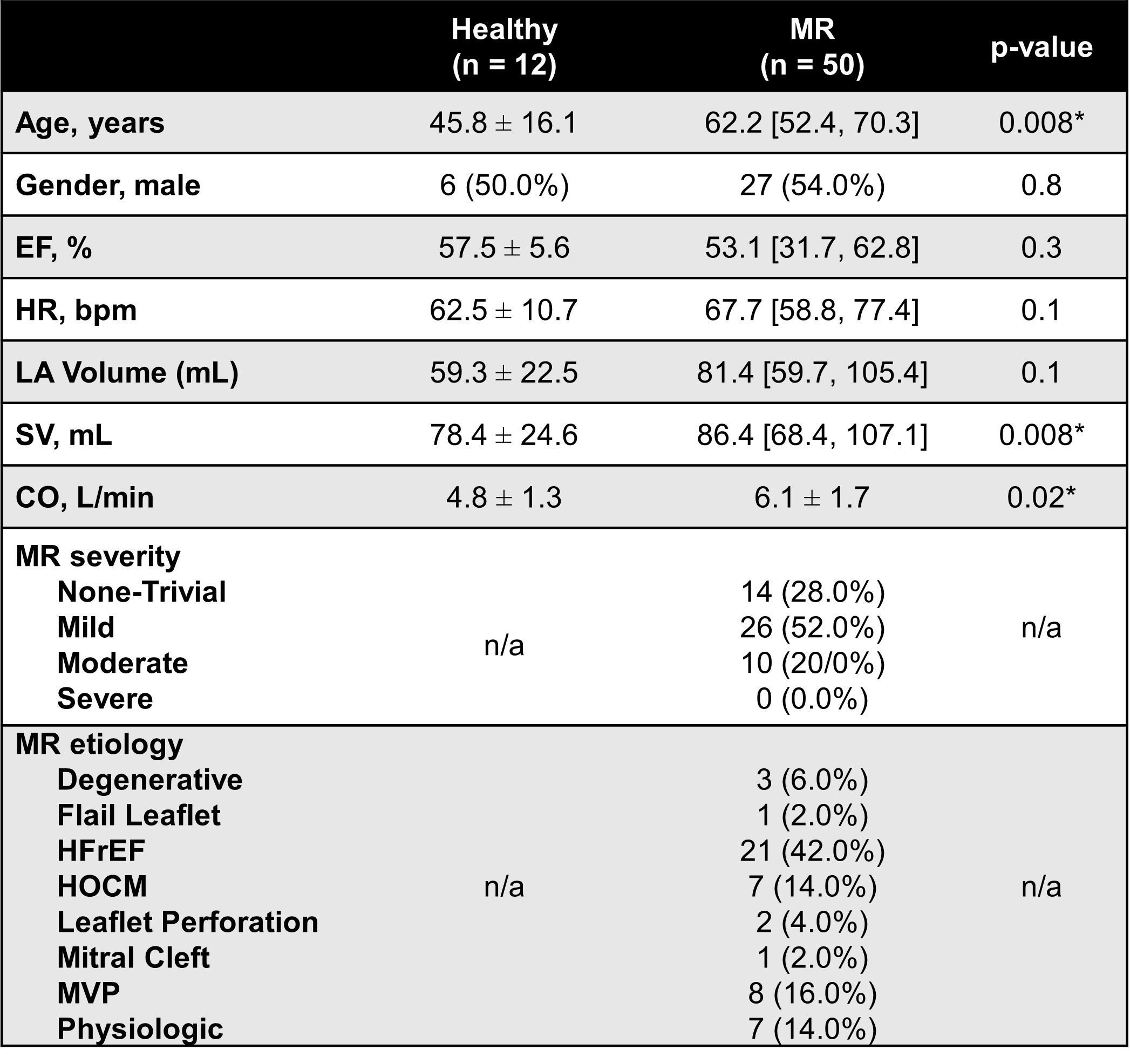
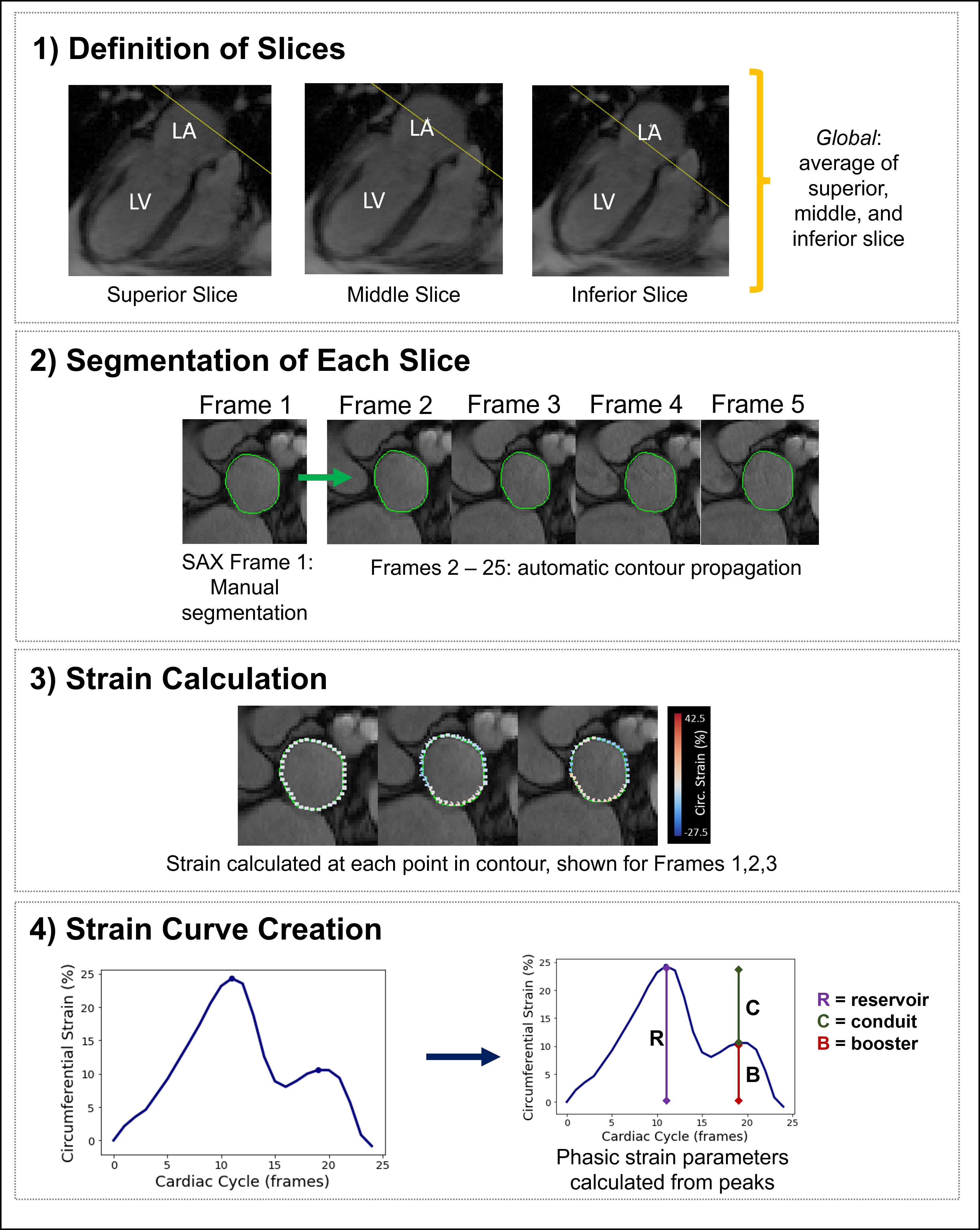
Fifty-one MR patients (27 male, age: 62.2 [52.4, 70.3]) who were prospectively recruited based on echocardiographic evidence of MR within 3 months from CMR and 12 healthy volunteers (6 male, age: 45.8±16.1 years) were retrospectively analyzed [Fig. 1]. Each participant underwent a cine SAX SSFP scan with 3 cross-sectional LA slices: superior, mid, and inferior [Fig. 2]. One MR patient was excluded due to insufficient number of slices. For test-retest reproducibility, the LA cine SAX SSFP scan was repeated 2 weeks later for the 12 healthy volunteers. Circumferential strain was computed from CMR as the strain component tangential to the LA contour using a FT prototype (TrufiStrain, Siemens) [Fig. 2]. Regional strain was computed for each LA slice separately (superior, mid, and inferior) by averaging strain over each slice. This was repeated for each time point to create a strain-time curve to calculate reservoir, conduit, and booster strain per slice3 [Fig. 2]. Global circumferential strain parameters were computed by averaging over all 3 slices. Test-retest reproducibility was assessed using the intraclass correlation coefficient (ICC). A parameter was defined reproducible if ICC> 0.754. The identified reproducible circumferential strain measures were 1) compared between MR patients and healthy volunteers; 2) tested their association in MR patients with regurgitant fraction, LA volume, and LV cardiac function: stroke volume (SV) and ejection fraction (EF).Results
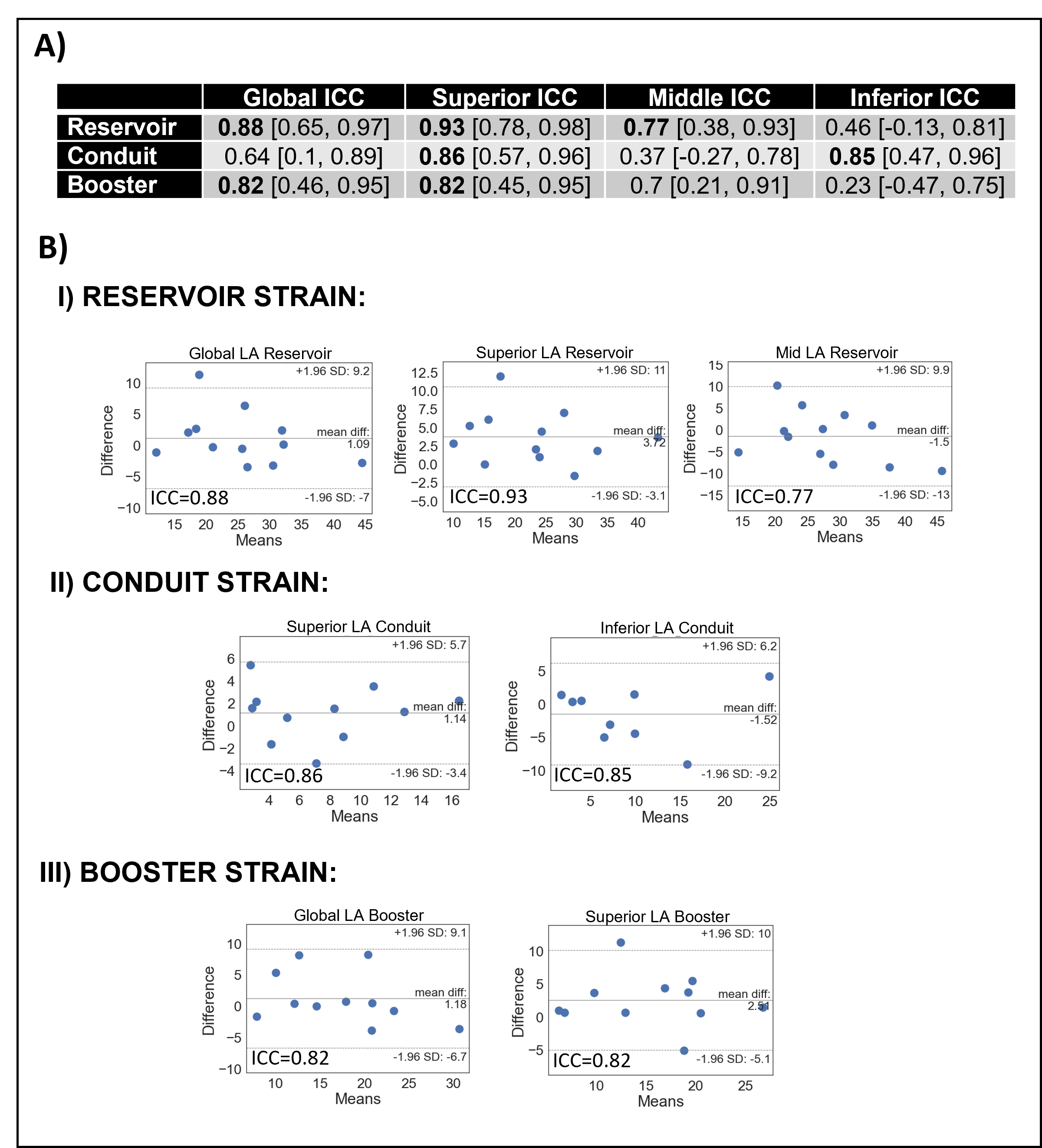
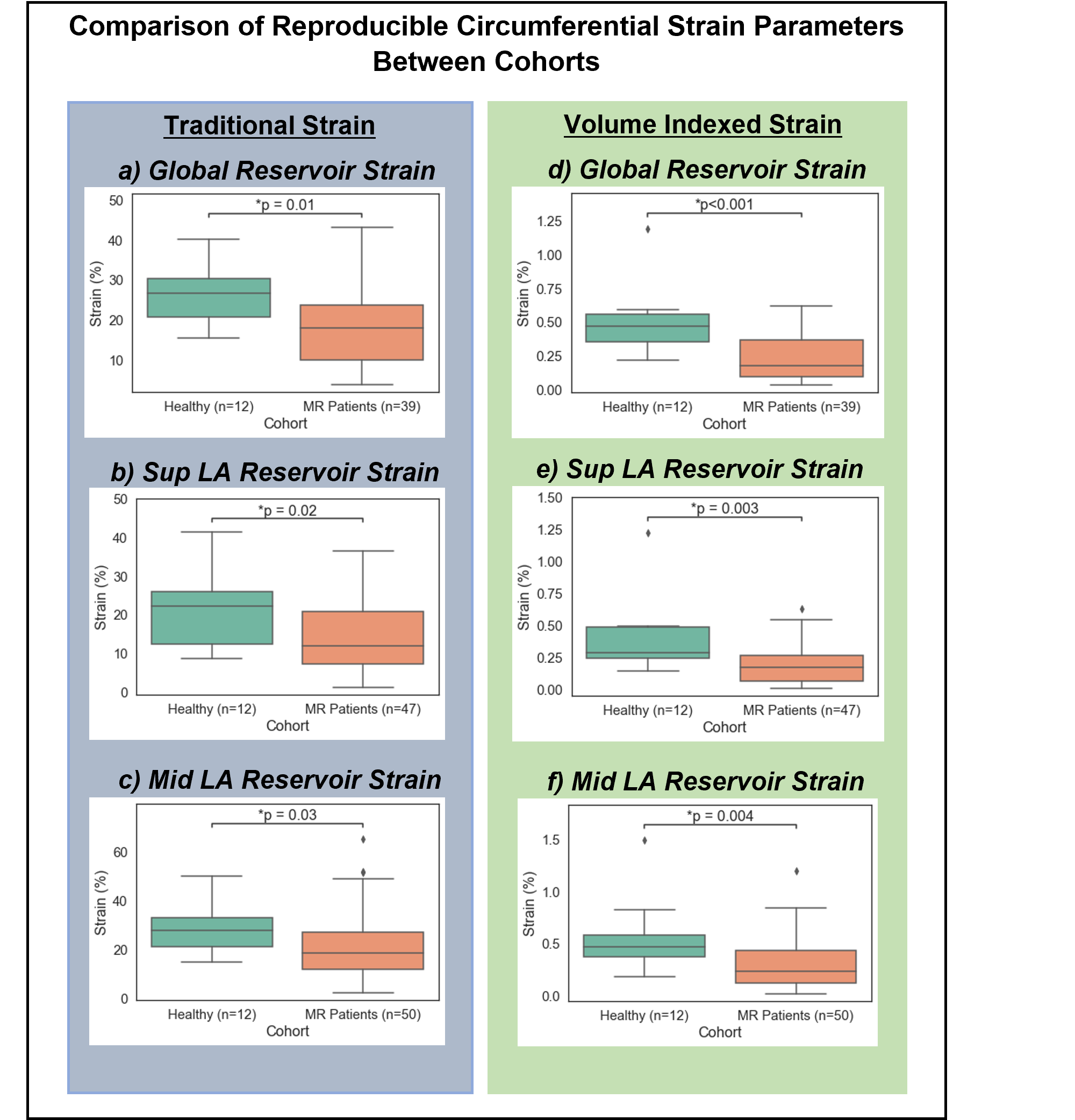
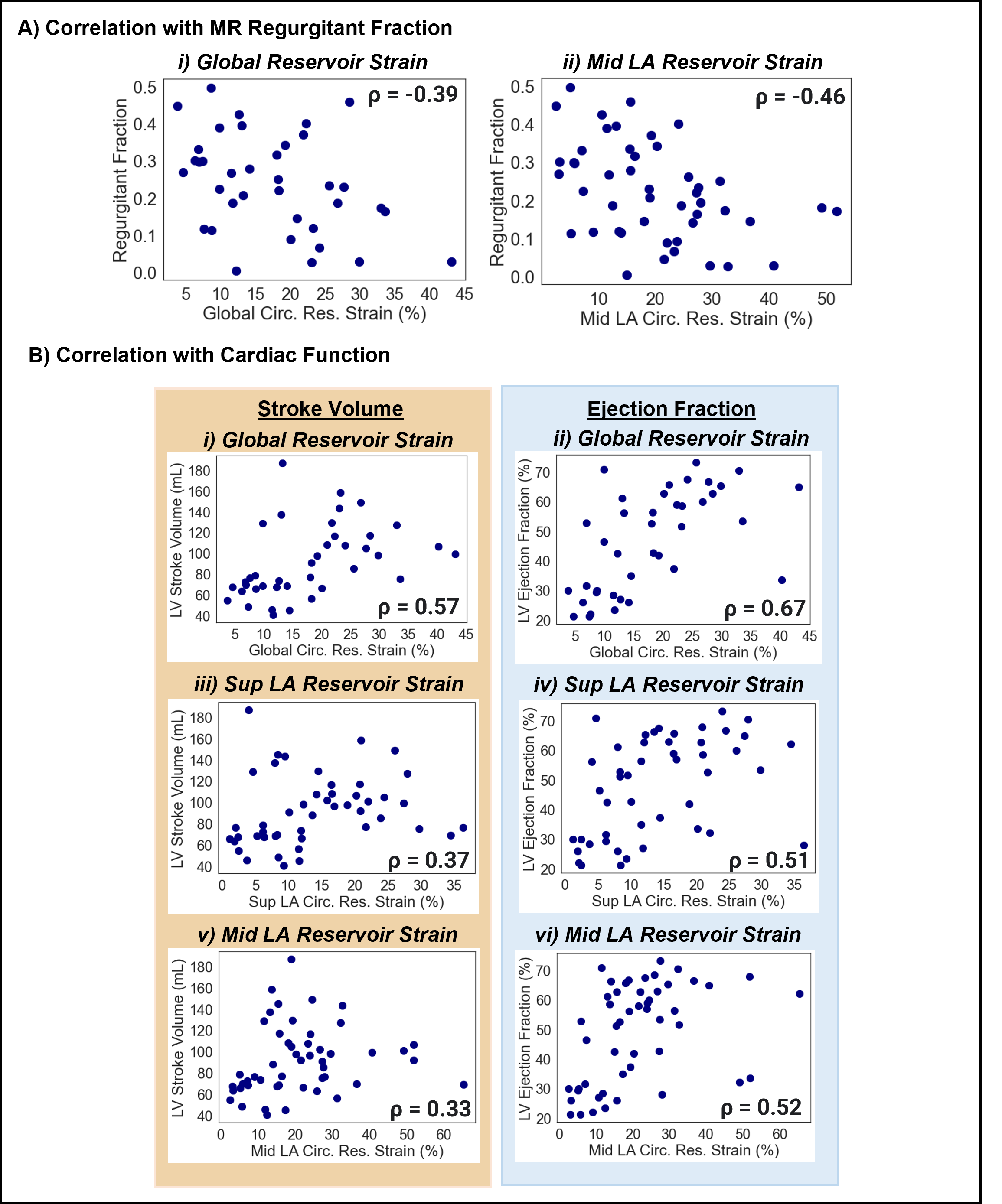
Test-retest reproducibility showed that most ‘global’ circumferential strain parameters were reproducible with circumferential reservoir strain ICC = 0.88 and circumferential booster strain ICC = 0.82 [Fig. 3A]. All three superior LA circumferential strain parameters were reproducible: ICC = 0.82 to 0.93 [Fig. 3BI-III]. Within the mid LA region, only circumferential reservoir strain was reproducible with ICC = 0.77 [Fig. 3BI]. In the inferior LA region, only circumferential conduit strain was reproducible with ICC = 0.85 [Fig. 3BII]. MR patients showed significantly lower values of circumferential strain than healthy volunteers at the reservoir phase when calculated globally (p=0.01), at the superior LA region (p=0.02), and at the mid LA region (p=.03) [Fig. 4A]. Similar results were found for volume-indexed circumferential strain parameters [Fig. 4B]. Global circumferential reservoir strain was inversely correlated with regurgitant fraction (ρ= -0.39) and directly correlated with SV (ρ = 0.57) and EF (ρ = 0.67) [Fig. 5A-B]. Superior LA circumferential reservoir strain was inversely correlated with LA volume (ρ = -0.39) and directly correlated with SV (ρ = 0.37) and EF (ρ = 0.51) [Fig. 5B]. Mid LA reservoir strain was inversely correlated with regurgitant fraction (ρ = -0.46) and LA volume (ρ = -0.31), and directly correlated with SV (ρ = 0.33) and EF (ρ = 0.52) [Fig. 5A-B].Discussion
To our knowledge, this is the first study to assess feasibility, reproducibility, and utility of LA circumferential strain by FT from CMR cine SAX SSFP. Realizing the importance of reproducibility, we first identified reproducible LA circumferential strain measures, by a conservative ICC>0.75, then only tested the reproducible measures. Global LA circumferential reservoir and booster strain are reproducible. Regionally, the superior LA region had the highest reproducibility potentially due to lesser bulk movement versus the inferior region that is prone to out-of-plane motion given proximity to mitral valve. The results show that adding only two SAX slices –using the same LV cine SSFP SAX protocol– at the superior and mid LA region allow reproducible measures of circumferential strain changes in MR patients. Global and regional circumferential reservoir strain are associated with MR severity as well as cardiac function parameters (EF, SV). Therefore, highlighting potential clinical utility.Conclusion
This study demonstrates the feasibility and reproducibility of quantifying global and regional circumferential LA strain by FT from cine CMR SAX SSFP and its potential utility in evaluating impaired LA mechanics in MR patients. Hence, it may facilitate clinical adoption given that it builds on the existing LV SAX pipeline. Future studies are needed to assess potential added value of CMR LA circumferential strain in prognosis of MR patients.Acknowledgements
AHA Student Scholarship in Cardiovascular DiseaseReferences
1. Enriquez-Sarano, Maurice, et al. “Mitral Regurgitation.” The Lancet., vol. 373, no. 9672, 2009, pp. 1382–94, https://doi.org/10.1016/S0140-6736(09)60692-9.
2. Cau, Riccardo et al. “The emerging role of atrial strain assessed by cardiac MRI in different cardiovascular settings: an up-to-date review.” European radiology vol. 32,7 (2022): 4384-4394. doi:10.1007/s00330-022-08598-6
3. Gan, Gary C. H., Aaisha Ferkh, Anita Boyd, and Liza Thomas. “Left Atrial Function: Evaluation by Strain Analysis.” Cardiovascular Diagnosis and Therapy 8, no. 1 (2018): 29–46. https://doi.org/10.21037/cdt.2017.06.08.
4. Koo,
Terry K., and Mae Y. Li. “A Guideline of Selecting and Reporting Intraclass
Correlation Coefficients for
Reliability Research.” Journal of Chiropractic
Medicine, vol. 15, no. 2, 2016, pp. 155–63,
https://doi.org/10.1016/j.jcm.2016.02.012.
Figures