4836
Predictive value of myocardial strain on myocardial infarction size in ST-segment elevation myocardial infarction with preserved LVEF1Department of Cardiology, Central Hospital Affiliated to Shandong First Medical University, Jinan, China, 2Research Center of Translational Medicine, Central Hospital Affiliated to Shandong First Medical University, Jinan, China, 3Department of Radiology, Central Hospital Affiliated to Shandong First Medical University, Jinan, China, 4Philips Healthcare, Beijing, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular, Acute ST-segment elevation myocardial infarction
With the development of the emergency system, we can see more and more acute ST-segment elevation myocardial infarction patients with preserved left ventricular ejection fraction.the predictive value of myocardial strain as determined by cardiac magnetic resonance (CMR) for myocardial infarct size could not been clarified by previous investigations in STEMI patients with preserved LVEF. The present study reveals incremental value of global circumferential strain (GCS), determined by CMR, for the prediction of infarction size after STEMI, above and beyond LVEF as well as global longitudinal strains. The findings of this study suggest that GCS may represents a potential marker of infarct size and may be used to better guide drug therapy. It may be beneficial to use GCS to determine the infarct size and prognosis of post-MI patients who do not qualify for contrast imaging.Introduction
CMR examination is considered the in vivo reference standard for measuring infarct size in STEMI patients. It is recommended that late gadolinium enhancement (LGE) be used for infraction size (IS) quantification. However, data regarding the correlation between strain and LGE of FT-CMR in STEMI patients are scarce and sometimes controversial. The predictive value of strain by FT-CMR for the infarct size of STEMI patients with preserved LVEF remains unclear. We aimed to investigate the correlation between myocardial strain and myocardial infarction size in patients of acute STEMI with preserved LVEF.Materials and Methods
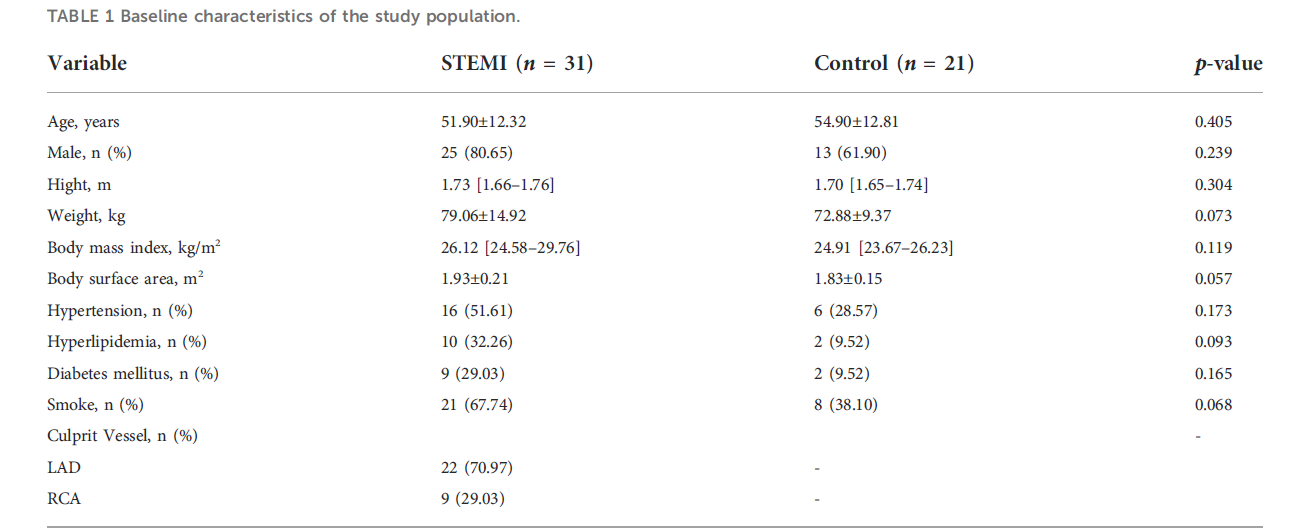
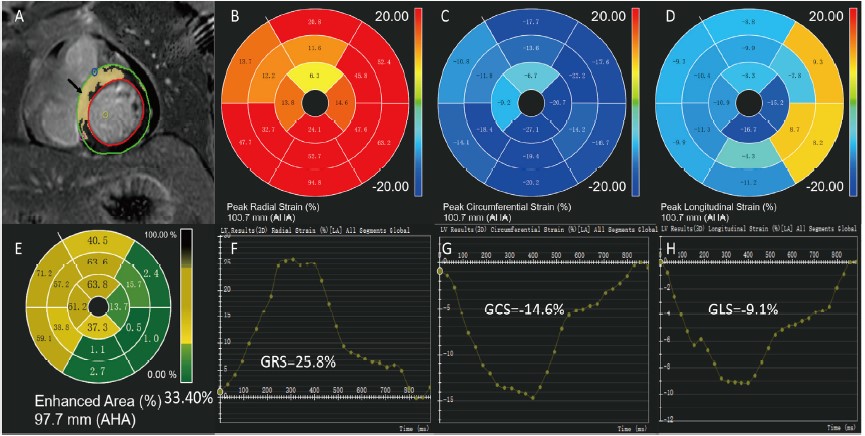
A retrospective study was conducted to assess 31 patients with acute ST-segment elevation myocardial infarction (STEMI)after primary percutaneous coronary intervention (PCI) who received cardiac magnetic resonance (CMR) imaging during hospitalization at the Central Hospital of Shandong First Medical University from 2019 to 2022 and whose echocardiography indicated preserved LVEF. The control group consisted of 21 healthy adults who underwent CMR during the same period. Cardiac MRI was performed on 3.0 T MRI systems (Elition, Philips Healthcare, Best, the Netherlands) using a 32-channel phased-array abdomen coil. The protocol consisted of cine imaging and late gadolinium enhancement (LGE) imaging for analysis. Infarct size was determined from the LGE images. All the analyses were conducted by two investigators with more than five years of experience each using the commercial software CVI42. We compared the CMR characteristics, global and segmental strain between the two groups. Furthermore, the correlation between the global strain and the segmental strain of the left ventricle and LGE were evaluated. Continuous variables were presented as mean ± standard deviation (SD) or median values with interquartile range (IQR), depending on the normality variables. Correlation between variables was performed using Spearman’s rank or Pearson correlation test. A multiple linear regression model was constructed to assess correlates of global circumferential strain (GCS), global longitudinal strain (GLS), LVEF, and LGE size. The optimal cut-off values to identify the LGE size of STEMI patients, whether higher than 25% or not, were derived from receiver operating characteristics (ROC) analysis by the Youden Index. All statistical analyses were conducted using R version 4.1.0 (The R Foundation, Austria).Results
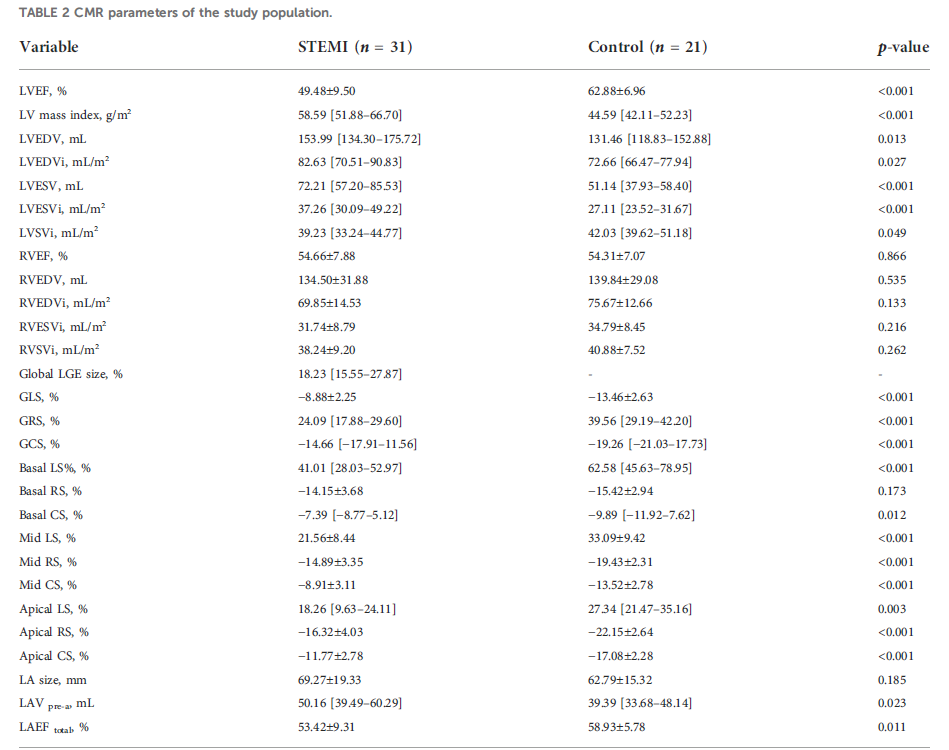
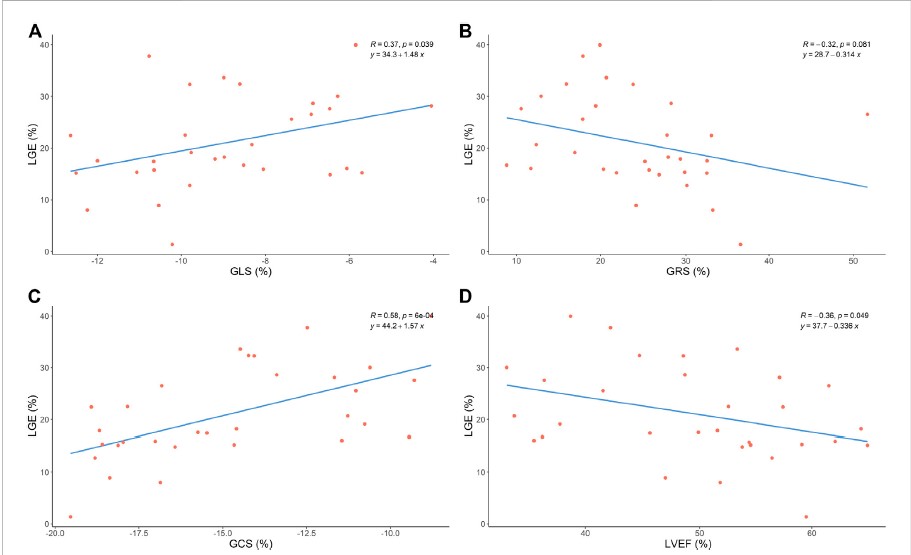
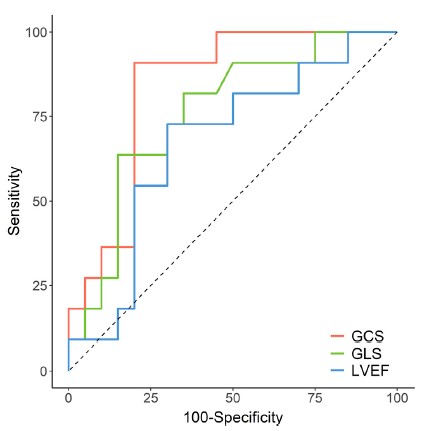
Compared with healthy controls, the left ventricular ejection fraction (LVEF) of STEMI patients with preserved LVEF was significantly decreased (p < 0.05). Moreover, the global radial strain (GRS) (24.09% [IQR:17.88 - 29.60%] vs. 39.56% [IQR:29.19 - 42.20%], p < 0.05), global circumferential strain (GCS) ( -14.66%[IQR: -17.91 -- 11.56%]vs. -19.26%[IQR: -21.03 --17.73%], p < 0.05), and global longitudinal strains (GLS) (-8.88 ± 2.25% vs. -13.46 ± 2.63%, p < 0.05) were damaged in patients. Furthermore, GCS and GLS were associated with LGE size (%left ventricle) (GCS: r = 0.58, p < 0.05; GLS: r = 0.37, p < 0.05). In the multivariate model, we found that LGE size was significantly associated with GCS (β coefficient = 2.110, p = 0.016) but was not associated with GLS (β coefficient = -0.102, p = 0.900) and LVEF (β coefficient = 0.227, p = 0.354). The receiver operating characteristic (ROC) results showed that GCS emerged as the strongest LGE size (LGE > 25%) prognosticator among strain parameters (AUC: 0.836 [95% CI, 0.692 – 0.981], sensitivity: 91%, specificity: 80%) and was significantly better (p = 0.001) than GLS (AUC: 0.761 [95% CI, 0.583 – 0.939], sensitivity: 64%, specificity: 85%) and LVEF (AUC: 0.673 [95% CI, 0.469 – 0.877], sensitivity: 73%, specificity: 70%).Discussion
In the present study, we investigated the characteristics of conventional CMR parameters and the correlation between the strain and LGE assessment by CMR-FT in STEMI patients with preserved LVEF. Our research has found that STEMI patients with preserved LVEF have impaired segmental strain, GLS, GCS, and GRS. Compared with healthy controls, STEMI patients had enlarged LVEDV, LVEDVi, LVESV, LVESVi, and LAVpre-a. Additionally, LVSVi and total LA EF tended to decline in patients. However, we did not find any significant differences in RVEF, RVEDV, RVEDVi, RVESV, RVESVi, or RVSVi between the two groups. GCS, GLS, and LVEF were associated with LGE size. Furthermore, GCS had superior diagnostic accuracy to GLS and LVEF in identifying myocardial infarction size in the STEMI patients with preserved LVEF. This work demonstrates that it may be possible to detect infarction size when GCS is impaired. Some patients develop renal impairment after acute MI, which makes them ineligible for gadolinium-contrast imaging. It is also possible to use strain imaging when gadolinium-contrast medium cannot be tolerated to assess infarct size.Conclusion
Global and segmental strain were impaired in STEMI patients with preserved LVEF treated by contemporary primary percutaneous coronary intervention. GCS and LGE were correlated, and GCS, as determined by CMR, emerged as a strong and independent predictor of infarction size. Moreover, GCS had superior diagnostic accuracy to GLS and LVEF for predicting myocardial infarction size.Acknowledgements
No acknowledgement found.References
1. Thiele H, Kappl MJ, Conradi S, Niebauer J, Hambrecht R, Schuler G: Reproducibility of chronic and acute infarct size measurement by delayed enhancement-magnetic resonance imaging. J Am Coll Cardiol 2006, 47(8):1641-1645.
2. Mahrholdt H, Wagner A, Judd RM, Sechtem U, Kim RJ: Delayed enhancement cardiovascular magnetic resonance assessment of non-ischaemic cardiomyopathies. Eur Heart J 2005, 26(15):1461-1474.
3. Ibanez B, Aletras AH, Arai AE, Arheden H, Bax J, Berry C, Bucciarelli-Ducci C, Croisille P, Dall'Armellina E, Dharmakumar R et al: Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel. J Am Coll Cardiol 2019, 74(2):238-256.
4. Yu S, Zhou J, Yang K, Chen X, Zheng Y, Zhao K, Song J, Ji K, Zhou P, Yan H et al: Correlation of Myocardial Strain and Late Gadolinium Enhancement by Cardiac Magnetic Resonance After a First Anterior ST-Segment Elevation Myocardial Infarction. Front Cardiovasc Med 2021, 8:705487.
5. Khan JN, Singh A, Nazir SA, Kanagala P, Gershlick AH, McCann GP: Comparison of cardiovascular magnetic resonance feature tracking and tagging for the assessment of left ventricular systolic strain in acute myocardial infarction. Eur J Radiol 2015, 84(5):840-848.
Figures