4829
Ultrafast and versatile non-contract-enhanced MRA for visualization of whole-body dynamic blood flow using flow-sensitive CINE imaging
Isao Shiina1, Michinobu Nagao2, Masami Yoneyama3, Yasutomo Katsumata3, Jihun Kwon3, Yasuhiro Goto1, Yutaka Hamatani1, Kazuo Kodaira1, Takumi Ogawa1, Mana Kato1, and Shuji Sakai2
1Department of Radiological Services, Tokyo Women's Medical University, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
1Department of Radiological Services, Tokyo Women's Medical University, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Keywords: Vessels, Blood vessels
Flow-sensitive CINE imaging is non-contrast-enhanced MRA technique based on the Turbo Field Echo Planar Imaging (TFEPI). Because TFEPI is sensitive to blood flow, the MRA acquired with flow-sensitive CINE imaging includes dynamic flow information. In this study, we applied flow-sensitive CINE imaging to a variety of body parts such as trunk and lower extremity. Volunteer data demonstrated its usefulness to a variety of body parts. The combination of anatomical vascular pattern and the dynamic flow information may enable comprehensive assessment of whole-body arteries.Main findings
This study demonstrated the feasibility of whole-body dynamic flow visualization using flow-sensitive CINE imaging. This technique could provide robust dynamic flow information visually within a shorter scan time compared with conventional methods.Introduction
Non-contrast-enhanced MR angiography (MRA) is used for the entire body to visualize the arterial vascular pattern. balanced Trigger Angiography Non-Contrast Enhanced (b-TRANCE) and Fresh Blood Imaging (FBI) methods are commonly used in trunk1, and 2D-Time-of-Flight (TOF) and Trigger angiography non contrast enhanced (TRANCE) methods are commonly used in the lower extremity. However, the aforementioned scan techniques all require ECG synchronization and respiratory control, which complicate the examination and prolong the scan time. These are relevant especially for patients with arrhythmia because the use of ECG synchronization can lead to insufficient synchronization. Also, the use of respiratory control prolongs the scan time for patients with difficulty in respiratory control and eventually leads to pronounced motion artifacts and poor image quality. Flow-sensitive CINE imaging is another non-contrast-enhanced MRA technique, which is based on the Turbo Field Echo Planar Imaging (TFEPI) technique2,3,4. Because TFEPI is sensitive to blood flow, the MRA acquired with this technique includes dynamic flow information. Flow-sensitive CINE imaging is inherently robust to arrhythmia because the scan is synchronized to pulse using a peripheral pulse unit (PPU) and the entire cardiac cycle is used for data acquisition. Besides, the ultrafast shot duration (4 sec per slice) of flow-sensitive CINE imaging minimizes the influence of motion and makes it applicable to any part of the body. Previously, flow-sensitive CINE imaging was applied to cardiac and demonstrated that it can visualize the backflow of blood as well as the valve motion.2 In this study, we applied this technique to a variety of body parts other than the cardiac. The purpose of this study was to investigate the feasibility of flow-sensitive CINE imaging for blood vessels in the trunk and lower extremity MRA.Methods
A total of six volunteers (five men, one woman, age range 30 to 45) were examined on a 3.0T MRI (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. Pulse sequence scheme of the TFEPI sequence is shown in Figure 1. Unlike balanced CINE, three directional gradient is not applied in TFEPI CINE to make it sensitive to flow. The flow-sensitive CINE imaging was applied to subcarinal, trunk, and lower extremity area and its usefulness was investigated. It has to be noted that this method does not require the setting of velocity encoding (VENC), which makes it easy to use. Flow-sensitive CINE imaging was acquired with free breath retrospective PPU gating. The following parameters were common to all exams: FOV=250 mm, pixel size=2.0x2.0 mm, slice thickness=8 mm, CS-SENSE reduction factor =2.3, EPI factor=5, TFE factor=3, flip angle=30, number of heart phase= 100, TR=7.9 ms, TE=4.1 ms, number of signals averaged (NSA)=1, and acquisition time was 4 sec per slice.Results and Discussion
Figure 2 shows the flow-sensitive CINE imaging for subcarinal MRA. Five slices were acquired and the total scan time was 20 sec. MRA in subcarinal region typically suffers from artifacts due to susceptibility difference, but flow-sensitive CINE imaging clearly demonstrated the dynamic blood flow as well as the vascular pattern. Figure 3 shows the renal blood vessel MRA acquired by flow-sensitive CINE imaging. Ultrafast scan of 12 sec minimized the influence of motion and the origin of the renal vessels was clearly delineated without breathing control. Figure 4 shows the trunk MRA acquired by flow-sensitive CINE imaging. The scan consists of three stacks and the total acquisition time was 300 sec. Continuous artery image from neck to pelvis clearly visualizes the vascular pattern across the large area. The combination of anatomical vascular pattern and the dynamic flow information may enable comprehensive assessment of arteries. Figure 5 shows the lower extremity MRA acquired by flow-sensitive CINE imaging. The scan consists of four stacks and the total acquisition time was 480 sec. Although the scan was conducted under free-breathing, the image was not influenced by the breathing motion or arrhythmia and the blood vessels were clearly delineated with additional dynamic flow information.Conclusion
This study demonstrated the feasibility of whole-body flow visualization using flow-sensitive CINE imaging. This technique could provide robust dynamic flow information visually within a shorter scan time compared with conventional methods.Acknowledgements
No acknowlegement found.References
1.Miyazaki M,Isoda H,Non-contrast-enhanced MR angiography of the abdomen.Eur J Radiol.80:9-23,2011
2. Shiina Y,et al.Semi-quantification of pulmonary regurgitation in congenital heart disease using 2D flow magnetic resonance imaging at 3.0T with modified Look-Locker sequence. International Journal of Cardiology Congenital Heart Disease 4 (2021)
3.Goto Y,et al. Novel ASL-based flow imaging for cardiovascular hemodynamics and valvular function visualization:comparision with a feasibility study Proc.ISMRM:2017.1576
4.Shiina I, et al. High-resolution flow-sensitive CINE imaging visualizing valve,chamber,and regurgitant flow Proc. ISMRM:2022.3910
Figures
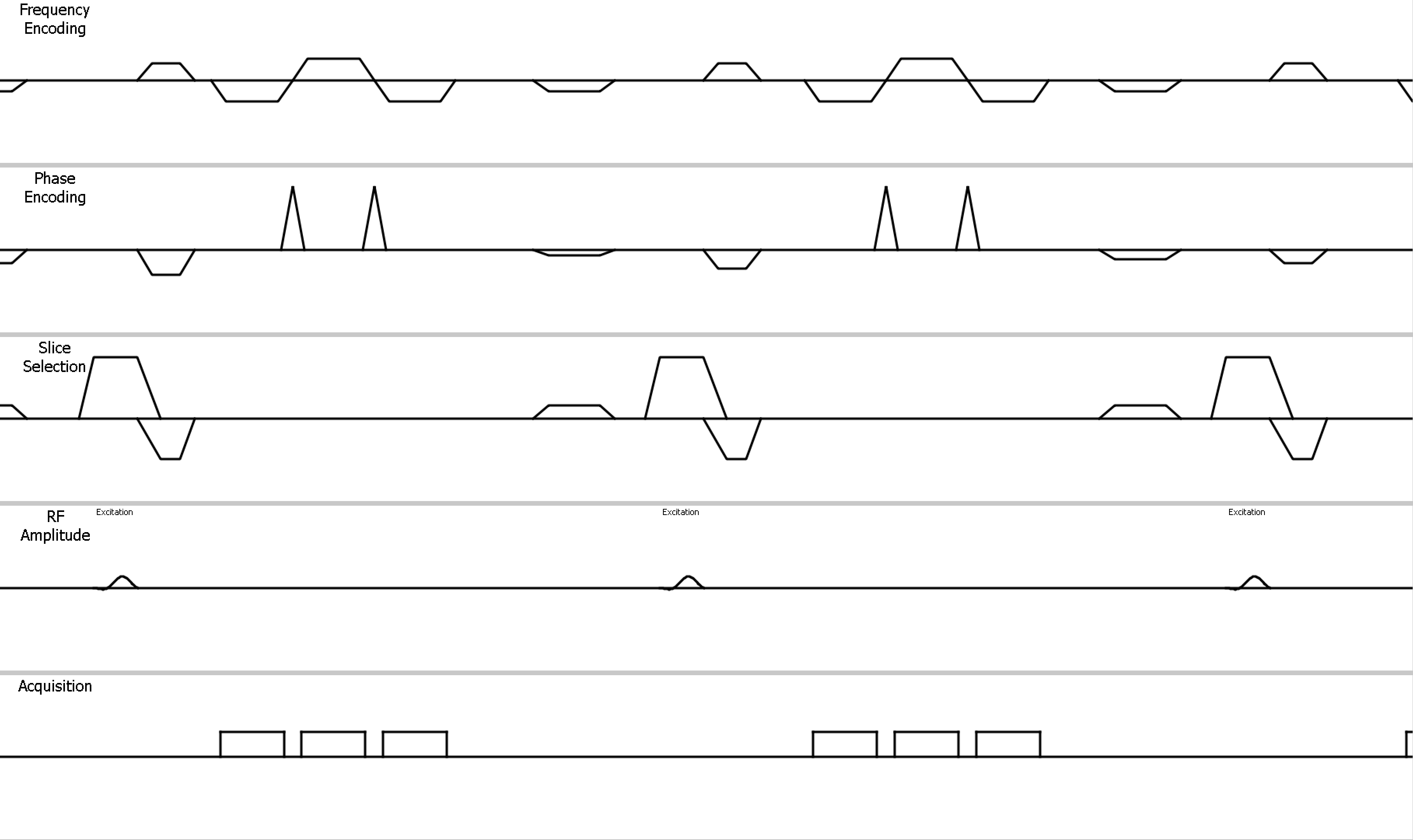
Fig 1.Pulse
sequence scheme of the TFEPI sequence.

Fig 2.Subclavian MRA with Flow-sensitive CINE Imaging.
The total scan time was 20 sec.

Fig 3.Renal Vascular MRA with Flow-sensitive CINE Imaging.
The total scan time was 12 sec.

Fig 4.Trunk MRA with Flow-sensitive CINE Imaging. The
scan consists of three stacks and the total acquisition time was 300 sec.
Fig 5.Lower extremity MRA with Flow-sensitive
CINE Imaging. The scan consists of four stacks and the total acquisition time
was 480 sec.
DOI: https://doi.org/10.58530/2023/4829