4825
Follow-up non-contrast-enhanced MRA using balanced turbo field-echo sequence for visceral artery aneurysm after endovascular therapy
Nobuyuki Kawai1, Yoshifumi Noda1, Tetsuro Kaga1, Kimihiro Kajita2, Hiroshi Kawada1, and Masayuki Matsuo1
1Radiology, Gifu University, Gifu, Japan, 2Radiology Services, Gifu University Hospital, Gifu, Japan
1Radiology, Gifu University, Gifu, Japan, 2Radiology Services, Gifu University Hospital, Gifu, Japan
Synopsis
Keywords: Vessels, Blood vessels
Contrast-enhanced MRA has been shown to be a safe and effective way to provide posttreatment visceral artery aneurysm (VAA) follow-up. However, this study cannot be performed for those who have contraindications to MR contrast agents. Balanced turbo field-echo (bTFE) sequence enables static and moving fluids to be shown as high intensity without the use of gadolinium. We assessed the feasibility of follow-up non-contrast-enhanced MRA using bTFE sequence for posttreatment VAA. Combined bTFE and unenhanced fat-suppressed T1-wighted (FS-T1W) images demonstrated excellent performance for the diagnosis of aneurysm reperfusion comparable to combined dynamic contrast-enhanced and unenhanced FS-T1W images.Introduction
Visceral artery aneurysms (VAA) are a rare but clinically important vascular condition. Because of the increased use of intra-abdominal imaging, including magnetic resonance (MR) imaging and computed tomography (CT), occult VAAs are being diagnosed with increased frequency1. These imaging studies allow detailed therapy planning for endovascular therapy, which is generally considered to be the preferred initial approach to most anatomically suitable VAAs. However, there is some concern of aneurysm reperfusion during follow-up. In addition, whereas radiopaque agent is necessary for endovascular therapy, this creates a significant metallic artifact on follow-up imaging2,3. As CT angiography is the most used follow-up study modality, certain reports have found that it cannot accurately determine aneurysm reperfusion because of the degree of metallic artifact4.Recently, contrast-enhanced MR angiography (MRA) has been shown to be a safe and effective way to provide posttreatment follow-up5. However, this study cannot be performed for those who have contraindications to MR contrast agents. Although there are limited to several reports on non-contrast-enhanced MRA for posttreatment VAAs, Some authors demonstrated the feasibility of non-contrast-enhanced MRA using balanced turbo field-echo (bTFE) sequence for endoleak detection after endovascular therapy6,7. On bTFE images, static and moving fluids, namely the flowing blood in arteries and veins, show inherent high intensity without the use of gadolinium. The purpose of this study was to evaluate the feasibility of follow-up non-contrast-enhanced MRA using bTFE sequence for posttreatment VAA.
Materials and Methods
This retrospective HIPAA-compliant study was approved by our IRB, and written informed consent was waived. Between January 2017 and June 2022, a total of 43 patients (27 men and 16 women; mean age, 65 years; range, 37‒87 years; mean BMI, 22.9 kg/m2) underwent follow-up contrast-enhanced dynamic MRA for VAA after endovascular therapy using a 1.5-Tesla (T) clinical scanner with a 20-channel (n = 26; Ingenia Prodiva CX; Philips Healthcare, Best, The Netherlands), a 3-T with a 16-channel (n = 16; Intera Achieva Quasar Dual), or a 3-T with 32-channel torso coil (n = 1; Ingenia CX). The mean time interval between endovascular therapy and follow-up MRA was 104 days (range, 31‒433 days). Our standard MRA protocol for VAA after endovascular therapy consisted of the following sequences: axial in-phase and opposed-phase T1-weighted gradient-echo sequence; axial breath-hold three-dimensional fat-suppressed T1-weighted (unenhanced FS-T1W) fast field-echo sequence; axial respiratory-triggered two-dimensional fat-suppressed T2-weighted turbo spin-echo sequence; axial and coronal respiratory-triggered two-dimensional single-shot bTFE sequence (Table 1). After obtaining precontrast images, 0.1 mL/kg of gadobutrol (n = 41) or 0.2 mL/kg of meglumine gadoterate (n = 2) was administered at a rate of 2 mL/s followed by a 30 mL saline flush at the same rate. Subsequently, dual-phase arterial and portal venous phase were obtained at 5 s and 45 s after arrival of the contrast agent at abdominal aorta detected by fluoroscopic bolus tracking system; and delayed phase was subsequently obtained at 180 s after administration of the contrast agent. All injections were performed using a commercially available power injector. And then, we created subtraction images of dynamic study. An experienced radiologist evaluated the image set and recorded the location, size, and embolization material of posttreatment VAA. Additionally, signal intensity (SI) of each posttreatment VAA against proximal artery on dynamic contrast-enhanced (DCE), bTFE, and unenhanced FS-T1W images were recorded in a 3-point scale (1 = completely low-, 2 = low with partially iso-, 3 = low with partially high-signal intensity). We defined as reperfusion using the score of DCE images only, bTFE images only, combined DCE and unenhanced FS-T1W images, and combined bTFE and unenhanced FS-T1W images, respectively. Subtraction images and all available follow-up studies were used to provide collect diagnosis of reperfusion. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and areas under the curve (AUCs) for the diagnosis of reperfusion were compared among the four image sets.Results
We evaluated 43 posttreatment VAAs (Table 2). Sensitivity, specificity, PPV, NPV, and AUCs for the diagnosis of reperfusion among the four image sets were summarized in Table 3. Specificity and PPV in combined DCE and unenhanced FS-T1W images (1.00 and 1.00, respectively) and combined bTFE and unenhanced FS-T1W images (0.94 and 0.78) were very high compared with DCE images only (0.60 and 0.36) and bTFE images only (0.57 and 0.35) (Fig. 1‒2). AUCs in bTFE images only was significantly lower than that in combined DCE and unenhanced FS-T1W images (0.79 vs. 0.94, respectively; P = 0.04). However, no statistically significant difference was found in AUCs between combined DCE and unenhanced FS-T1W images and combined bTFE and unenhanced FS-T1W images (0.94 vs. 0.91, respectively; P = 0.15).Discussion
Combined bTFE and unenhanced FS-T1W images demonstrated excellent performance for the diagnosis of reperfusion comparable to combined DCE and unenhanced FS-T1W images. Our results demonstrated that the feasibility of follow-up non-contrast-enhanced MRA using bTFE sequence for posttreatment VAA. Non-contrast-enhanced MRA is best suited to children and women of childbearing potential or those who have contraindications to CT or MR contrast agents (i.e., pregnancy, renal insufficiency, or gadolinium-based contrast agent allergy).Conclusion
MRA using combined bTFE and unenhanced FS-T1W images achieved comparable diagnostic ability of reperfusion for posttreatment VAA without contrast agent compared to combined DCE and unenhanced FS-T1W images.Acknowledgements
The authors of this abstract declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
- Chaer RA, Abularrage CJ, Coleman DM, et al. The Society for Vascular Surgery clinical practice guidelines on the management of visceral aneurysms. Journal of vascular surgery 2020;72:3s-39s.
- Tulsyan N, Kashyap VS, Greenberg RK, et al. The endovascular management of visceral artery aneurysms and pseudoaneurysms. Journal of vascular surgery 2007;45:276-83; discussion 83.
- Pulli R, Dorigo W, Troisi N, Pratesi G, Innocenti AA, Pratesi C. Surgical treatment of visceral artery aneurysms: A 25-year experience. Journal of vascular surgery 2008;48:334-42.
- Yamamoto S, Hirota S, Maeda H, et al. Transcatheter coil embolization of splenic artery aneurysm. Cardiovascular and interventional radiology 2008;31:527-34.
- Koganemaru M, Abe T, Uchiyama D, et al. Detection of neck recanalization with follow-up contrast-enhanced MR angiography after renal artery aneurysm coil embolization. Journal of vascular and interventional radiology : JVIR 2010;21:298-300.
- Mori K, Saida T, Sato F, et al. Endoleak detection after endovascular aneurysm repair using unenhanced MRI with flow suppression technique: Feasibility study in comparison with contrast-enhanced CT. European radiology 2017;27:336-44.
- Kawada H, Goshima S, Sakurai K, et al. Utility of Noncontrast Magnetic Resonance Angiography for Aneurysm Follow-Up and Detection of Endoleaks after Endovascular Aortic Repair. Korean journal of radiology 2021;22:513-24.
Figures
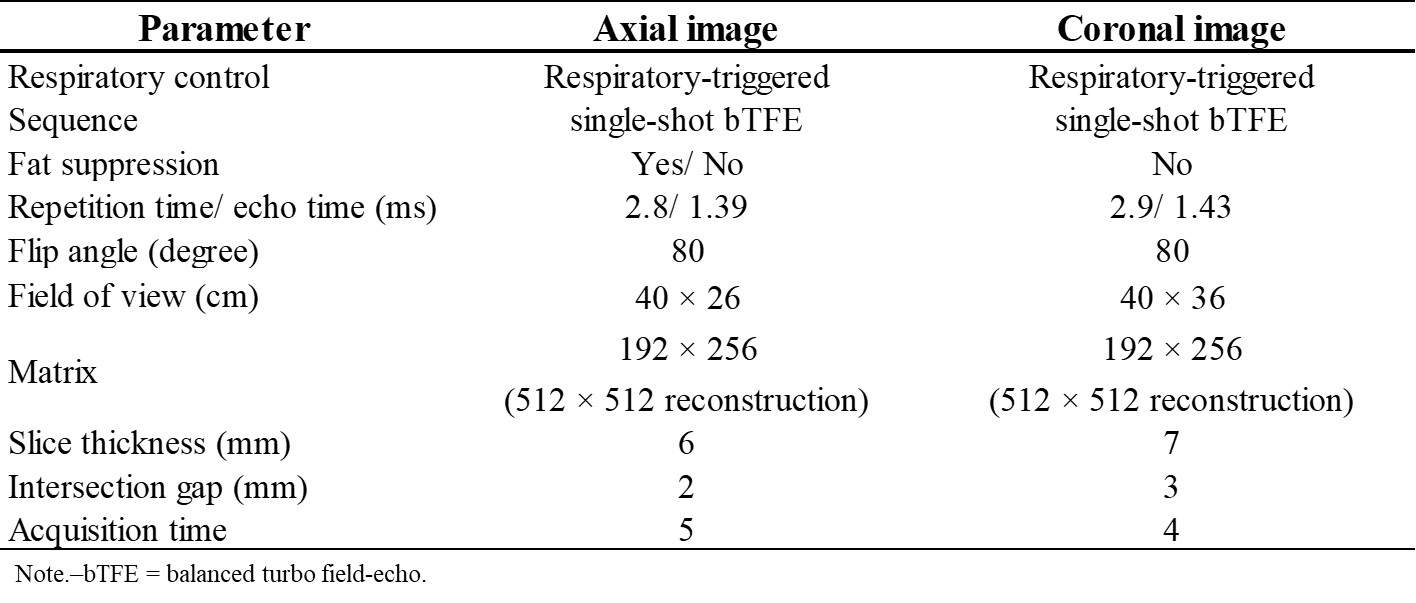
Scan parameters of balanced turbo field-echo sequence.
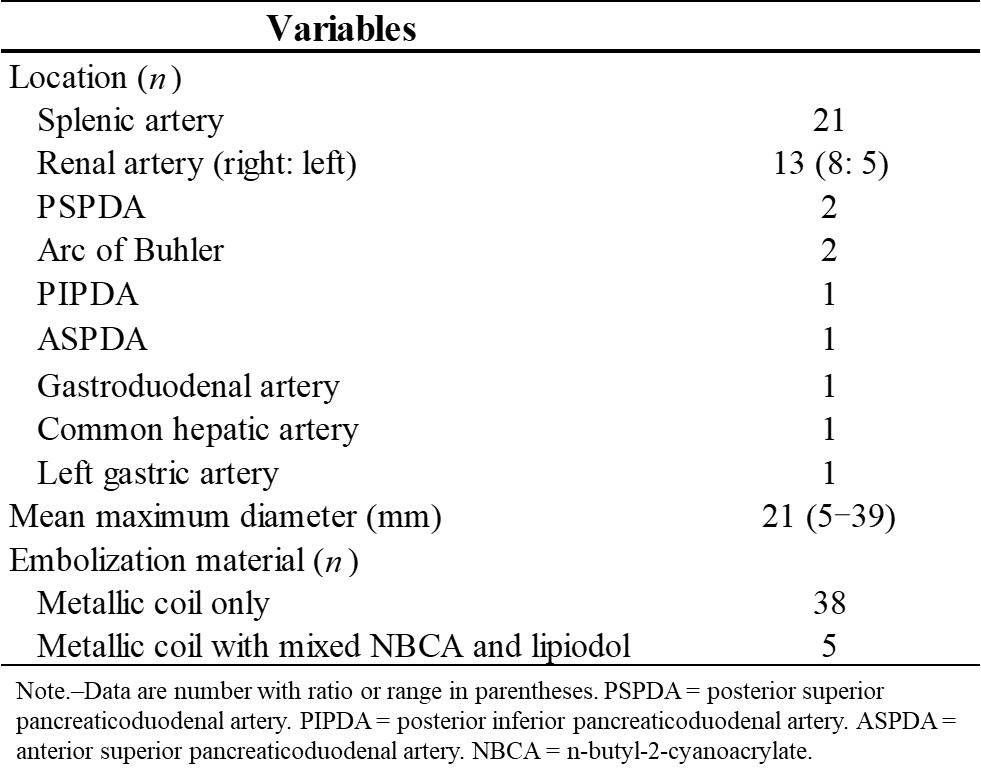
Location, size, and embolization material of posttreatment visceral artery
aneurysm.

Sensitivity, specificity, PPV, NPV, and AUCs for the diagnosis of reperfusion
of posttreatment visceral artery aneurysm among the four image sets.
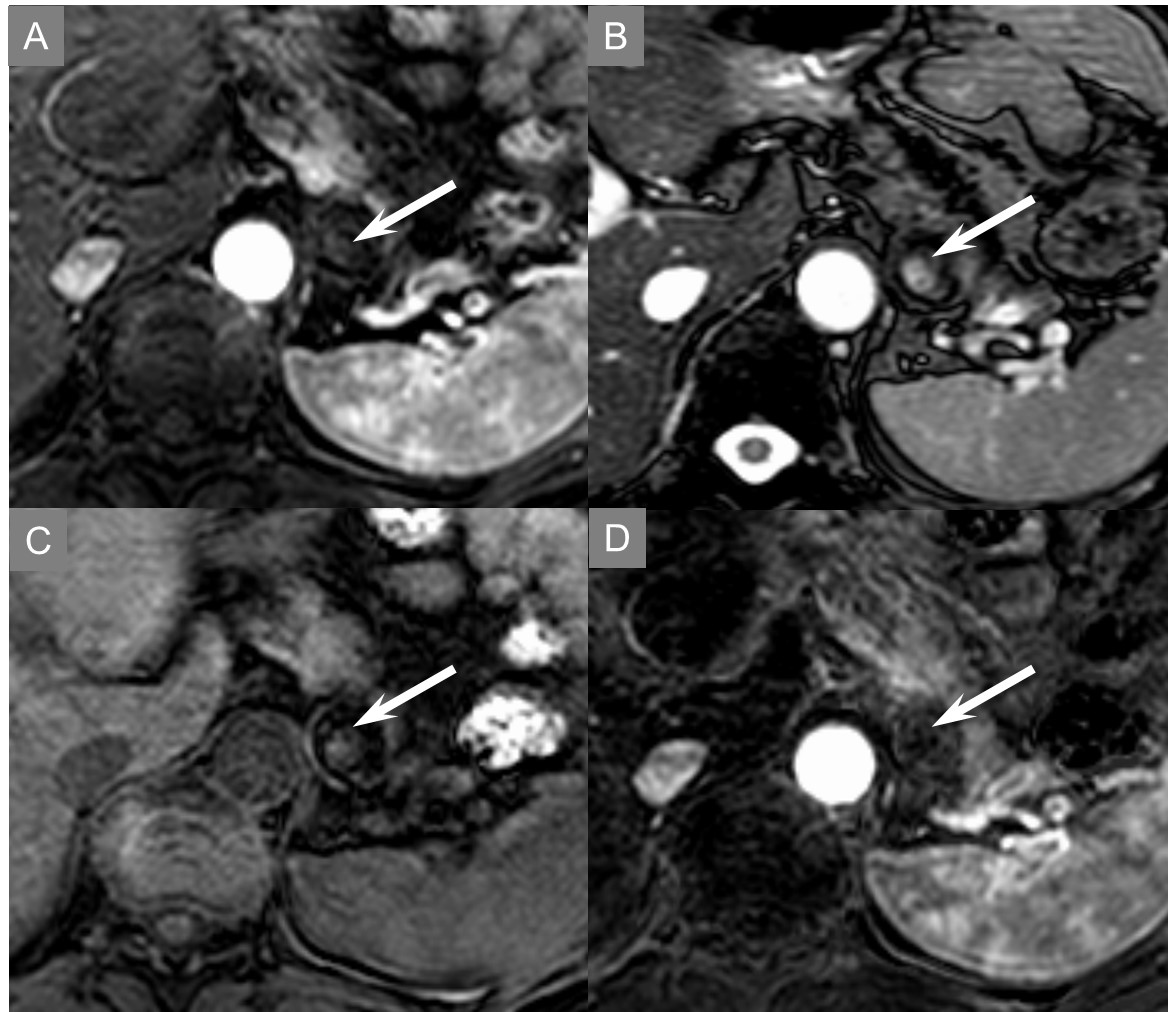
A 53-year-old female with splenic artery aneurysm after metallic coil
embolization. Both arterial phase (A) and bTFE (B) image showed low with
partially iso-signal intensity against proximal artery in posttreatment splenic
artery aneurysm (score 2), however, unenhanced FS-T1W (C) image showed low with
partially high-signal intensity (score 3). Subtraction image (D) showed completely
low signal intensity. This abnormality means fresh clot in posttreatment splenic
artery aneurysm.
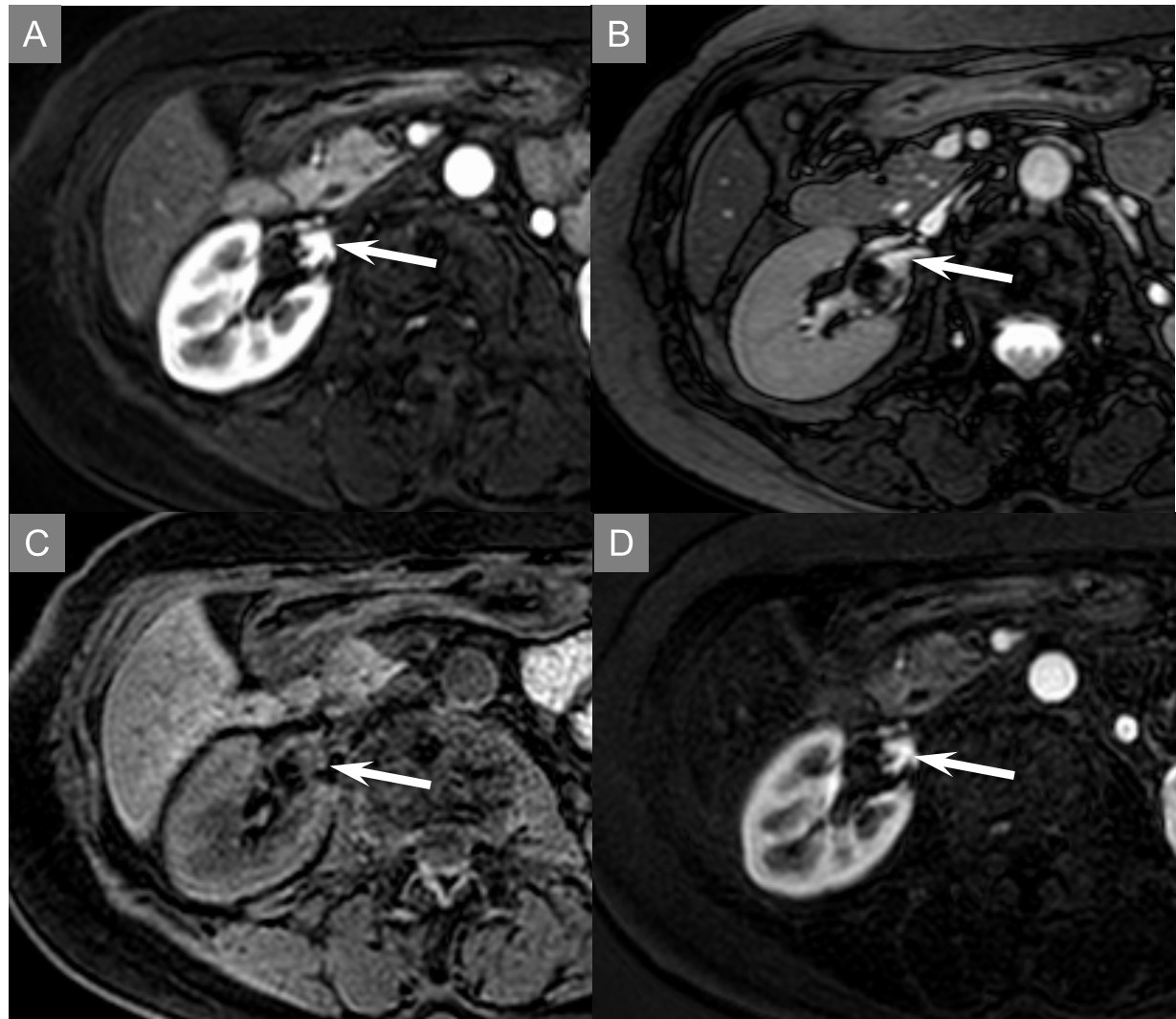
A 70-year-old female with right renal artery aneurysm after metallic coil
embolization. Arterial phase (A), bTFE (B), and unenhanced FS-T1W (C) image showed
low with partially iso-signal intensity against proximal artery in posttreatment
splenic artery aneurysm (score 2). Subtraction image (D) also showed the same
signal intensity. This abnormality means reperfusion in posttreatment right
renal artery aneurysm.
DOI: https://doi.org/10.58530/2023/4825