4815
A simultaneous dual slice acquisition with spiral trajectory for morphological and functional lung assessment
Anne Slawig1,2, Andreas Max Weng2, and Herbert Köstler2
1University Clinic and Outpatient Clinic for Radiology, University Hospital Halle (Saale), Halle (Saale), Germany, 2Department of Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany
1University Clinic and Outpatient Clinic for Radiology, University Hospital Halle (Saale), Halle (Saale), Germany, 2Department of Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany
Synopsis
Keywords: Lung, Data Analysis, ventilation, functional lung imaging, senceful
SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) is a well-established method to determine functional lung parameters and was already successfully combined with 3D-UTE for robust ventilation quantification. Nevertheless, the evaluation of not only ventilation, but also perfusion, requires a 2D excitation, as it is based on the inflow effect. Additionally, coverage of more than one slice within short measurement times is valuable. Here, it is shown that functional information can be obtained from two slices acquired simultaneously, thus doubling the anatomical coverage of a conventional 2D acquisition.Introduction
MR imaging of the lung is very challenging but of high interest for functional analysis, especially in pediatric patients or to monitor chronic lung diseases1–3. Many pathologies are characterized by ventilation or perfusion defects and can be distinguished from certain deficit patters in one or both parameters.One approach to determine these functional lung parameters is the SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) algorithm4 which has already proven itself in multiple clinical applications5,6. While it was already successfully combined with 3D-UTE for robust ventilation quantification7,8, the evaluation of perfusion requires a 2D RF-excitation, as it relies on the inflow effect. Nonetheless, coverage of the whole lung within short measurement times is valuable. Therefore, here, the feasibility of combining the SENCEFUL algorithm with a simultaneous dual slice acquisition is evaluated.
Methods
All experiments were performed on a 3T-MRI (Siemens MAGNETOM PrismaFit). Coronal 2D measurements of the lungs were performed in a healthy volunteer. Firstly, one simultaneous dual-slice measurement featuring a center-out spiral trajectory was performed with an echo time of 0.46ms. A gradient preemphasis was employed to prospectively offset effects of gradient system imperfection and mainly eddy currents in order to ensure good image quality9,10. Secondly, one single slice Cartesian scan using a quasi-random line ordering with an echo time of 0.69 ms was acquired for comparison. Total measurement time was chosen to be 2 min for each acquisition. Other imaging parameters were fixed for both measurements as well: TR=2.0ms, flip angle=8°, resolution=3.0x3.0mm2, slice thickness=10mm. By analyzing the DC-signal of the k-space, the temporal data was retrospectively gated into 30 respiratory phases and 21 cardiac phases. For spiral-out imaging, the first point in each readout is positioned at the center of k-space and was used for gating, while in Cartesian imaging the DC signal is acquired separately after each readout. A segmentation of the lung was performed by a region-growing algorithm and functional parameters were determined using the standard SENCEFUL algorithm4. Ventilation values were normalized to the end-expiration signal and overall lung volume change during one breathing cycle. Perfusion values were normalized to a ROI sampling pure blood in the descending aorta.Results
Results of the measurements in a healthy volunteer are shown in Figure 1. The morphological overview shows the expected signal behavior for Cartesian and spiral imaging with the respective echo times. The two simultaneously acquired slices, shown in Figure 1a, feature the proton-weighted contrast and high signal in the lung parenchyma, as typical for imaging with short echo times.The ventilation maps (Figure 1b) acquired by the simultaneous dual slice acquisition are comparable to the maps from a Cartesian single slice acquisition. Likewise, the perfusion maps are comparable through all measurements (Figure 1c). Large vessels in distal areas are clearly visible, while perfusion values decrease in the proximal regions. In general, maps from spiral acquisition seem to be blurred in comparison to the Cartesian acquisition. As the anterior slice acquired in the simultaneous dual slice acquisition is positioned very close to the chest wall, small areas in the left lung seem to be corrupted by through plane motion.
Discussion
The quantification of ventilation and perfusion is feasible in the simultaneous dual-slice acquisition. In a healthy volunteer, the ventilation is expected to be uniform in a coronal slice, which can be seen in the obtained ventilation maps.Perfusion maps, in correspondence to anatomical conditions, show strong inflow in large proximal vessels and lower but widely distributed signal in distal regions.
Employing a spiral trajectory allows for fast coverage of k-space resulting in a short overall measurement time. Whether the blurring in images with spiral trajectories is caused by the not sampled corners of the Cartesian k-space has to be determined in further studies.
Advantages of spiral acquisitions are general robustness towards motion and the intrinsic acquisition of the DC-signal in each readout. Additionally, it allows for acquisitions with ultrashort echo times, where the highly enhanced SNR, especially in the lung parenchyma, is beneficial for functional lung imaging.
In contrast to the more common 3D approach for UTE, the 2D acquisition allows the generation of perfusion related parameters. But, the necessity of slice selection limits minimum TE, such that a 2D sequence cannot achieve the same shortness of TE as a 3D approach. Additionally, through-plane motion (especially of the heart and large vessels) can cause difficulties in image registration and the determination of functional values. The proposed simultaneous dual-slice acquisition combines the benefit of acquiring perfusion information with short measurement times for whole lung coverage.
Future work should extend the evaluation against standard SENCEFUL imaging towards a larger cohort and different pathologies.
Conclusion
It has been shown here that SENCEFUL can be performed on a simultaneous dual slice acquisition. Functional information can be obtained from two slices simultaneously, thus doubling the anatomical coverage of a conventional 2D acquisition. In contrast to 3D approaches, perfusion can be evaluated in addition to ventilation, within the same measurement. Prospectively, acquisition times for functional imaging of the whole lung can thus be reduced by half.Acknowledgements
No acknowledgement found.References
1. Hirsch FW, Sorge I, Vogel-Claussen J, et al. The current status and further prospects for lung magnetic resonance imaging in pediatric radiology. Pediatr Radiol 2020;50:734–749 doi: 10.1007/s00247-019-04594-z.2. Serai SD, Rapp JB, States LJ, Andronikou S, Ciet P, Lee EY. Pediatric Lung MRI: Currently Available and Emerging Techniques. AJR Am J Roentgenol 2021;216:781–790 doi: 10.2214/AJR.20.23104.
3. Voskrebenzev A, Vogel-Claussen J. Proton MRI of the Lung: How to Tame Scarce Protons and Fast Signal Decay. J Magn Reson Imaging 2021;53:1344–1357 doi: 10.1002/jmri.27122.
4. Fischer A, Weick S, Ritter CO, et al. SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) using a quasi-random fast low-angle shot (FLASH) sequence and proton MRI. NMR in Biomedicine 2014;27:907–917 doi: 10.1002/nbm.3134.
5. Kunz A, Weng A, Wirth C, et al. Funktionelle native Lungen-MRT (SENCEFUL) zur Ermittlung pulmonaler Perfusionsdefizite bei Cystischer Fibrose. In: RöFo - Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren. Vol. 189. Georg Thieme Verlag KG; 2017. p. WISS 314.8. doi: 10.1055/s-0037-1600447.
6. Veldhoen S, Weng AM, Knapp J, et al. Self-gated Non–Contrast-enhanced Functional Lung MR Imaging for Quantitative Ventilation Assessment in Patients with Cystic Fibrosis. Radiology 2016;283:242–251 doi: 10.1148/radiol.2016160355.
7. Klimeš F, Voskrebenzev A, Gutberlet M, et al. 3D phase-resolved functional lung ventilation MR imaging in healthy volunteers and patients with chronic pulmonary disease. Magn Reson Med 2021;85:912–925 doi: 10.1002/mrm.28482.
8. Pereira LM, Wech T, Weng AM, et al. UTE-SENCEFUL: first results for 3D high-resolution lung ventilation imaging. Magnetic Resonance in Medicine 2019;81:2464–2473 doi: 10.1002/mrm.27576.
9. Stich M, Wech T, Slawig A, et al. Gradient waveform pre-emphasis based on the gradient system transfer function. Magnetic Resonance in Medicine 2018;80:1521–1532 doi: 10.1002/mrm.27147.
10. Eirich P, Wech T, Heidenreich JF, et al. Cardiac real-time MRI using a pre-emphasized spiral acquisition based on the gradient system transfer function. Magnetic Resonance in Medicine 2021;85:2747–2760 doi: https://doi.org/10.1002/mrm.28621.
Figures
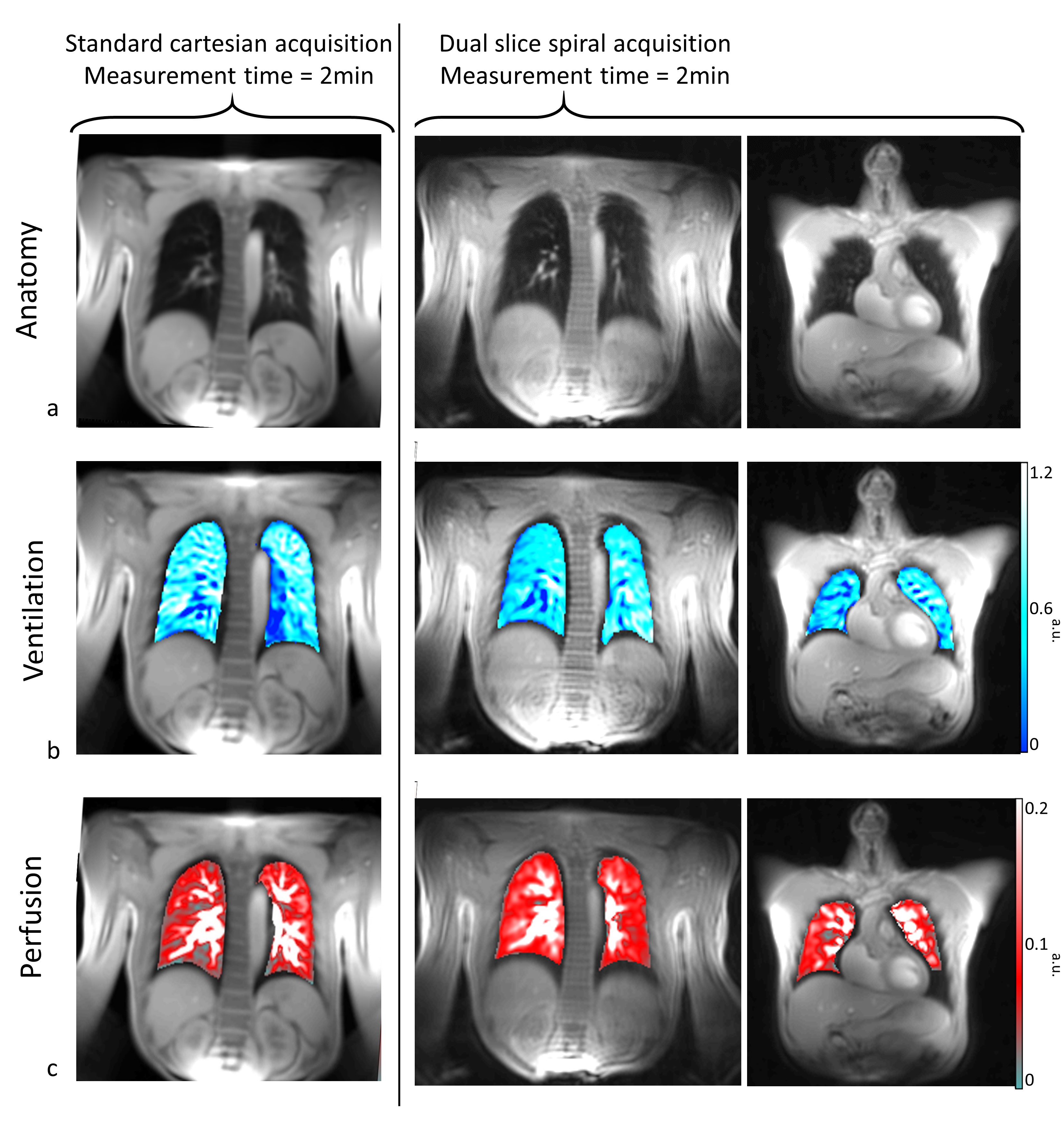
Figure 1: MR-images of the lung using a Cartesian single slice acquisition of slice 1 (left) and a spiral simultaneous multi-slice acquisition of slice 1 (center) and slice 2 (right). a) morphological overview b) ventilation maps as determined by SENCEFUL in MRI acquisitions. c) perfusion maps as determined by SENCEFUL.
DOI: https://doi.org/10.58530/2023/4815