4814
Evaluation of a Patient with Interstitial Lung Disease Using 3D Perfusion Maps Based on 3D Ultrashort Echo-time Imaging1Department of Biomedical Engineering, Sungkyunkwan University, Suwon, Korea, Republic of, 2Department of Intelligent Precision Healthcare Convergence, Sungkyunkwan University, Suwon, Korea, Republic of, 3Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea, Republic of, 4Department of Pulmonary and Critical Care Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea, Republic of
Synopsis
Keywords: Lung, Perfusion, Interstitial lung diseases
Since vascular abnormalities are common features of interstitial lung disease, not only structural images but also functional images such as perfusion maps are required to accurately evaluate vascular abnormalities including pulmonary hypertension. In this preliminary study, we proposed a method of evaluating an interstitial lung disease (ILD) patient particularly with idiopathic interstitial pneumonia (IIP) using 3D perfusion maps as well as high-resolution 3D structural images, both of which were obtained from 3D ultrashort echo-time imaging. Fibrotic areas were well identified in the structural UTE images as well as in the perfusion maps showing increased perfusion signals in the corresponding lesions.Introduction
Interstitial lung disease (ILD) includes a large group of complex parenchymal lung diseases that cause various patterns of inflammation and fibrosis throughout the alveolar, interstitial, and vascular compartments of the lung1. Vascular abnormalities are a common feature of ILD, and these inflammatory and granulomatous disorders can cause the development of pulmonary hypertension by affecting small pulmonary vessels. Idiopathic interstitial pneumonia, particularly idiopathic pulmonary fibrosis (IPF), and connective tissue disease-associated ILD have a profound impact on lung microcirculation2-4. However, vascular changes in ILD, to date, have been difficult to quantify in the absence of overt pulmonary hypertension. Therefore, it is important to have regional functional information of the lungs along with structural information in the diagnosis of ILD patients, and this is expected to enable more objective assessment of functional characteristics and size of lesions, as well as prediction of future exacerbations. In recent studies, MRI techniques such as ultrashort echo-time (UTE) imaging showed the possibility to image ILD structural changes at greater resolution5, 6, and contrast-enhanced imaging provided a means of pulmonary perfusion assessment7. In this preliminary study, we investigated the functional characteristics of an ILD patient with idiopathic interstitial pneumonia (IIP) using 3D pulmonary perfusion maps obtained from 3D non-contrast enhanced UTE images as well as 3D UTE images themselves for structural information.Methods
The study protocol was approved by the Institutional Review Board of Asan Medical Center (2021–0787). Lung perfusion was assessed in one ILD patient using 3T MRI (Magnetom Skyra, Siemens).Experiment: A volume-selective 3D UTE sequence (VS-UTE) was used with fat suppression (10). Scan parameters were: TR/TE = 3.3/0.12ms, FOV = 360mm, number of projections = 150k, matrix size = 440×440×440, isotropic resolution = 0.8mm, and flip angle = 5°. A self-navigation method developed by our group was used to trace respiratory and cardiac motion8-10.
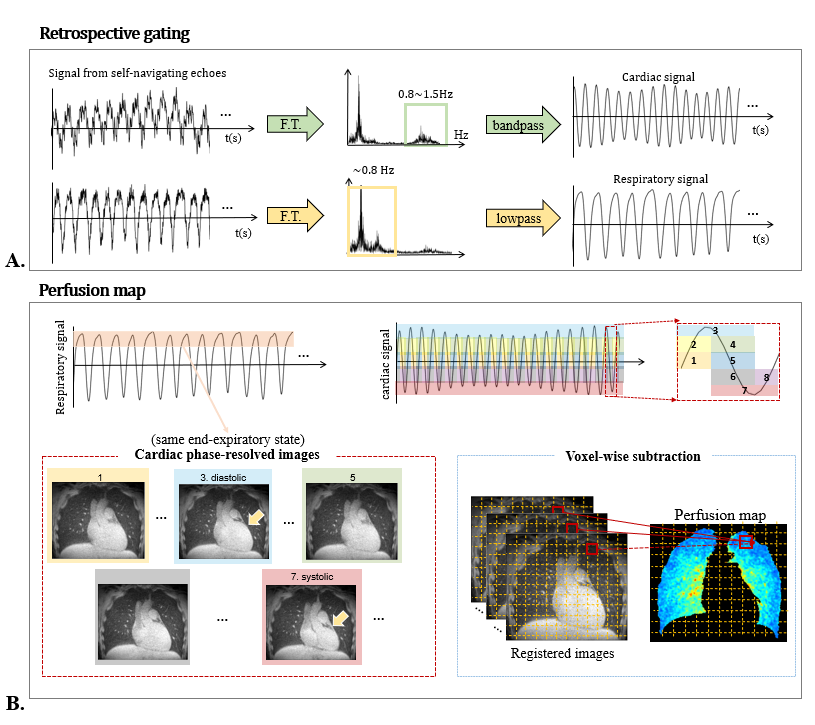
Perfusion map: To create perfusion maps, retrospective cardiac gating was performed at the end-expiration respiratory phase to acquire cardiac phase-resolved images. Cardiac signals were extracted from respiration signals with bandpass filtering (0.8-1.5Hz) (Fig. 1A) and eight cardiac phase-resolved images were reconstructed from common projections for each cardiac phase and end-expiratory phase. The number of projections used for each cardiac-phase image reconstruction was set equal to 18k. Then, a difference image was calculated by subtracting the minimum from the maximum of each voxel from eight cardiac phase-resolved images after image registration11, and the perfusion map was finally obtained by dividing the difference image by the mean value of the region-of-interest (ROI) in the pulmonary trunk (Fig. 1B)12. Image registration was performed using the nonrigid image registration tool ANTs.
Results
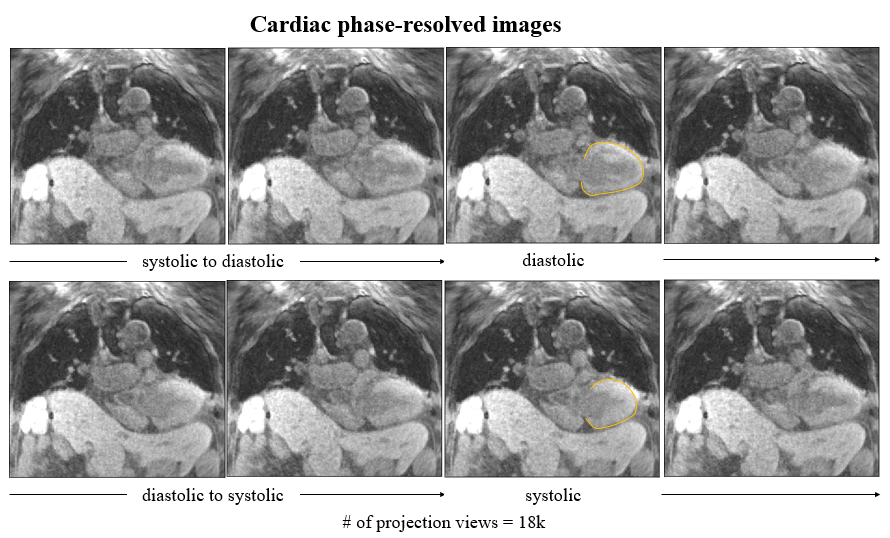
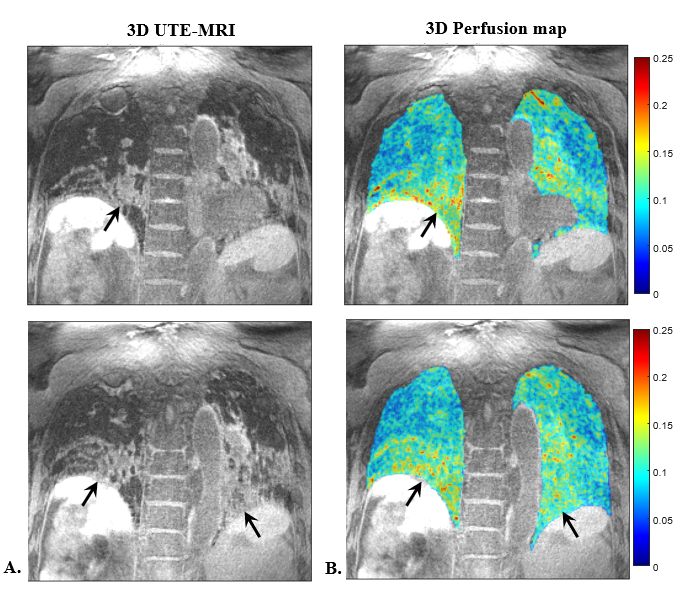
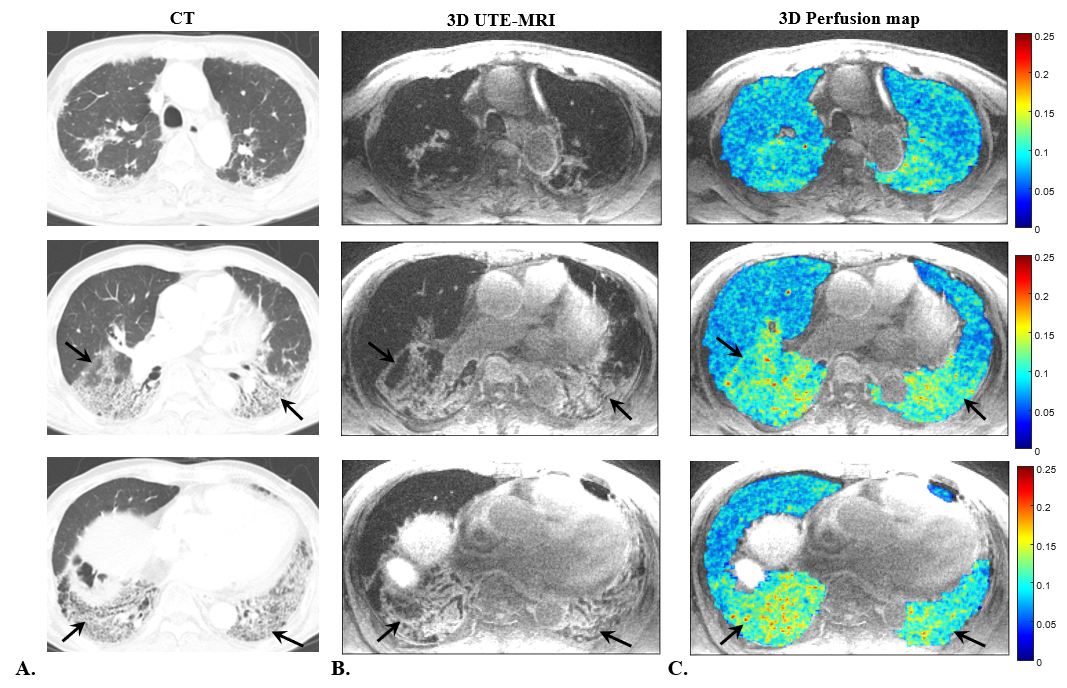
Figure 2 shows the eight cardiac phase-resolved images reconstructed from retrospective gating of the 3D UTE-MRI data. Despite the under-sampled reconstruction via retrospective respiratory and cardiac gating, they clearly represent cardiac motions, including systolic and diastolic, during the cardiac cycle. Figure 3 shows representative coronal slices of structural UTE images and UTE-based perfusion maps of an ILD patient. Figure 4 shows representative axial slices of structural CT images, structural UTE images, and UTE-based perfusion maps of the same ILD patient. Consistent with CT images, structural UTE images well-identified areas of fibrosis in the lower lobes of both lungs (Fig. 3A, Figs. 4A, B, red arrows). UTE-based perfusion maps also showed distinctively increased signal intensity in basal lung lesions (Fig. 3B, Fig 4C, red arrows).Discussion and Conclusion
In this preliminary study, we analyzed one ILD patient with IIP using 3D UTE-based perfusion maps as well as 3D UTE images. The fibrotic areas were well identified in the structural UTE images as well as in the perfusion maps demonstrating clearly high perfusion signals in the corresponding lesions. There are some possibilities for increased perfusion signals in the basal lesion of ILD patients. First, this patient has traction bronchiectasis and ground-glass opacity in the peripheral portion of both lower lungs, and they usually appear when active inflammation or subtle fibrosis is in progress. In this case, the inflammation process may accompany vascular development, increasing the perfusion signal of the lesion. Second, this patient was treated with corticosteroids, which can also increase the perfusion signal of the lesion because corticosteroids can facilitate blood supply by dilating peripheral blood vessels, increasing cardiac output, and reducing platelet aggregation. Since only one ILD patient with IIP was considered, a large cohort of ILD patients is needed to confirm the clinical utility of the proposed method. Despite this limitation, this preliminary study shows that the proposed method is promising for more accurate diagnosis of ILD patients in that it can utilize anatomical information and perfusion information at the same time.Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT): NRF-2020R1A2B5B02002676, NRF-2021R1A4A5032806, and NRF-2021R1C1C2008365References
1) Wallis A, Spinks K. The diagnosis and management of interstitial lung diseases. Bmj. 2015;350.
2) Nathan SD, Shlobin OA, Ahmad S, et al. Serial development of pulmonary hypertension in patients with idiopathic pulmonary fibrosis. Respiration. 2008;76(3):288-294.
3) Nathan SD, Noble PW, Tuder RM. Idiopathic pulmonary fibrosis and pulmonary hypertension: connecting the dots. American journal of respiratory and critical care medicine. 2007;175(9): 875-880.
4) Diaz-Guzman E, Farver C, Parambil J, Culver DA. Pulmonary hypertension caused by sarcoidosis. Clinics in chest medicine. 2008;29(3):549–563.
5) Ohno Y, Nishio M, Koyama H, et al. Pulmonary MR imaging with ultra-short TEs: utility for disease severity assessment of connective tissue disease patients. European journal of radiology. 2013; 82(8):1359–65.
6) Park JY, Moeller S, Goerke U, et al. Short echo‐time 3D radial gradient‐echo MRI using concurrent dephasing and excitation. Magnetic resonance in medicine. 2012;67(2): 428-436.
7) Swift AJ, Telfer A, Rajaram S, et al. Dynamic contrast-enhanced magnetic resonance imaging in patients with pulmonary arterial hypertension. Pulmonary circulation. 2014;4(1):61–70.
8) Park J, Park J-Y. Reducing Streak Artifacts in 3D Radial Imaging Using Volume-Selective Signal Acquisition. Proc. Intl. Soc. Mag. Reson. Med. 28. 2020.
9) Park J, Lee S, Shin T, Oh S-H, Park J-Y. A Robust Self-navigation for Respiratory Gating in 3D Radial Ultrashort Echo-time Lung MRI using Concurrent Dephasing and Excitation. Journal of the Korean Physical Society. 2018;73(1):138-44.
10) Park J, Shin T, Yoon SH, Goo JM, Park JY. A radial sampling strategy for uniform k‐space coverage with retrospective respiratory gating in 3D ultrashort‐echo‐time lung imaging. NMR in Biomedicine. 2016;29(5):576-87.
11) Kim H, Lee S, Park J, Park J-Y. 3D Pulmonary Perfusion Mapping Using 3D Ultrashort Echo-time Imaging. Proc. Intl. Soc. Mag. Reson. Med. 30. 2022.
12) Kjørstad Å, Corteville DM, Fischer A, Henzler T, Schmid‐Bindert G, Zöllner FG, et al. Quantitative lung perfusion evaluation using Fourier decomposition perfusion MRI. Magnetic Resonance in Medicine. 2014;72(2):558-6.
Figures