4805
Values of golden-angle radial-VIBE in DCE-MRI in laryngeal and hypopharyngeal squamous cell carcinoma: comparison with conventional VIBE1Department of Radiology, The First Affiliated Hospital of Guangxi Medical University, Nanning, China, 2MR Scientific Marketing, Siemens Healthineers Ltd., Wuhan, China, 3MR R&D Collaborations, Siemens Medical Solutions, Los Angeles, CA, United States
Synopsis
Keywords: Image Reconstruction, Head & Neck/ENT
This study aimed to investigate the value of a dynamic contrast-enhanced (DCE)-MRI with golden-angle radial volumetric‑interpolated breath‑hold examination (radial-VIBE) research application sequence by comparing with conventional VIBE in patients with laryngeal and hypopharyngeal squamous cell carcinoma (SCC) under free breathing conditions. Our results showed that compared with conventional contrast-enhanced VIBE images with single phase, the morphological radial-VIBE images of multitemporal synthesis had significantly higher image quality based on subjective (edge, artifact, and confidence) and objective (signal-to-noise ratio, contrast, and contrast-to-noise ratio) assessments. Therefore, radial-VIBE can be used in DCE‑MRI examination in laryngeal and hypopharyngeal SCC in the free breathing state.
Introduction
MR imaging and CT are used for staging of laryngeal and hypopharyngeal squamous cell carcinoma (SCC). Compared with conventional CT, MR imaging has higher soft-tissue contrast resolution and higher sensitivity in diagnosing the surrounding structure invasion by laryngeal or hypopharyngeal SCCs. However, motion artifacts are a serious problem with MR imaging in patients with difficulty in breathing and swallowing. Due to the high temporal resolution, lower motion sensitivity and no aliasing artifacts, Dynamic contrast enhanced (DCE) MRI with golden angle radial stack-of-stars volumetric‑interpolated breath‑hold examination (radial-VIBE) acquisitions has gained more and more interest, and has been applied to tumors, such as prostate, gastric, esophageal carcinoma [1,2]. The purpose of this study was to assess the value of radial-VIBE in patients with laryngeal and hypopharyngeal SCC through comparisons of morphological radial-VIBE images of multitemporal synthesis and conventional 3D-VIBE sequence with free breathing.Method
This prospective study was approved by the Institutional Review Board of our hospital. Twenty-three patients with laryngeal and hypopharyngeal SCC confirmed by pathology and without any treatment, were recruited between October 2021 and June 2022. All patients underwent MRI on a 3T system (MAGNETOM Prisma; Siemens Healthcare, Erlangen, Germany) equipped with 18-element body matrix coil and an inbuilt 32 element spine matrix coil. Besides conventional T1WI, T2WI and DWI, DCE images were acquired with a research application radial-VIBE sequence, followed by a conventional VIBE sequence to obtain contrast enhanced images with free breathing. The imaging parameters were as follows: radial-VIBE, TR 6.81 ms, TE 2.42 ms, flip angle 12°, FOV 180 mm × 180 mm2, slice thickness 2 mm, slices number 40, base resolution 320, radial views 1394, bandwidth 490Hz/Px, Temporal resolution 34, Temporal spacing 7.4s, total scanning time 302s, 0.4 ml/kg GD-DTPA was intravenously injected at a speed of 3.0 ml/s with an injector in the cubital vein; 3D-VIBE, TR 3.72 ms, TE 1.55 ms, flip angle 9°, FOV 180 mm × 180 mm2, slice thickness 2 mm, slices number 56, matrix 288 × 288, measurements 1, bandwidth 530Hz/Px, scanning time 64s.The image quality of the radial-VIBE image reconstructed by all k-space data and VIBE image were compared by subjective and objective assessments. The subjective image quality was assessed through the edge and detail of lesion, artifact, and diagnostic confidence based on a 5-Likert scale by two radiologists with more than 5 years of experience. Objective image quality was measured by signal-to-noise ratio (SNR), contrast (C) and contrast-noise ratio (CNR). The formulas were as follows: SNR = SId/SD, CNR = (SId − SIm)/ SD, and C = (SId- SIm)/(SId+SIm ). where SId and SIm were the signal intensity of the lesion and muscle at the maximum level of the lesion, respectively; SD was the standard deviation (SD) of the background signal.
Statistical analysis was performed using SPSS 24.0 (IBM, New York, USA). A Wilcoxon signed rank test was used to analyze the differences in subjective image quality classification between the radial-VIBE and conventional VIBE groups. The SNR, CNR, and C of the groups were analyzed by paired t test. A two-tailed p < 0.05 was considered significant.
Results
The image quality of radial-VIBE was significantly higher than that of VIBE (all p values < 0.05 in Table 1). Representative images are shown in Figure 1. Obvious breathing and swallowing motion artifacts were present in the conventional VIBE image, but were reduced in the corresponding radial-VIBE image.Radial-VIBE had significantly higher SNR, CNR and C than those of VIBE (p < 0.05, respectively), as shown in Table 2 and Figure 2.
Discussion
Compared to the conventional VIBE using Cartesian k-space sampling trajectories, radial-VIBE with radial k-space sampling trajections is insensitive to motion, and therefore motion artifacts can be effectively mitigated. In our study, the image quality of radial-VIBE was superior to that of VIBE, with clearer edge of lesions, less motion artifact, and higher confidence. The conventional VIBE sequence showed obvious breathing and swallowing motion artifacts in the image, which may hamper the clinical evaluation of laryngeal or hypopharyngeal lesions. When radial-VIBE was used, these artifacts were significantly reduced, and the laryngeal or hypopharyngeal lesions were better visualized. Improved image quality of radial-VIBE increased diagnosis confidence, and was more helpful in clinical application.We found that the radial-VIBE images had significant higher SNR, CNR and C than VIBE, which was consistent with previous research [3,4]. Radial-VIBE can reconstruct the acquired data at very high temporal resolution using only a small number of radial spokes for every temporal frame. This enables high resolution free-breathing perfusion imaging with higher in-plane spatial resolution and thinner partitions. In addition, the morphological radial-VIBE images with multitemporal synthesis used all radial sampling data and more data in k-space center was acquired, resulting higher SNR compared with Cartesian mode. Therefore, the lesion can be displayed better.
Conclusion
Radial-VIBE can provide higher-quality morphological images compared to the conventional high-resolution 3D-VIBE sequence in free breathing and can be applied in DCE-MRI for laryngeal and hypopharyngeal squamous cell carcinoma.Acknowledgements
No acknowledgement found.References
Reference
1. Li, H. H. et al. Feasibility of free-breathing dynamic contrast-enhanced MRI of gastric cancer using a golden-angle radial stack-of-stars VIBE sequence: comparison with the conventional contrast-enhanced breath-hold 3D VIBE sequence. Eur. Radiol. (2018). 28, 1891–1899.
2. Rosenkrantz, A. B. A. et al. Dynamic contrast-enhanced MRI of the prostate with high spatiotemporal resolution using compressed sensing, parallel imaging, and continuous golden-angle radial sampling: Preliminary experience. MRI (2015).41, 1365–1373.
3. Shin, H. J. et al. Comparison of image quality between conventional VIBE and radial-VIBE in free-breathing paediatric abdominal MRI. Clin. Radiol. (2016).71, 1044–1049.
4. Deng H.P. et al. DCE‑MRI of esophageal carcinoma using star‑VIBE compared with conventional 3D‑VIBE. Scientific Report (2021). 11:24091.
Figures
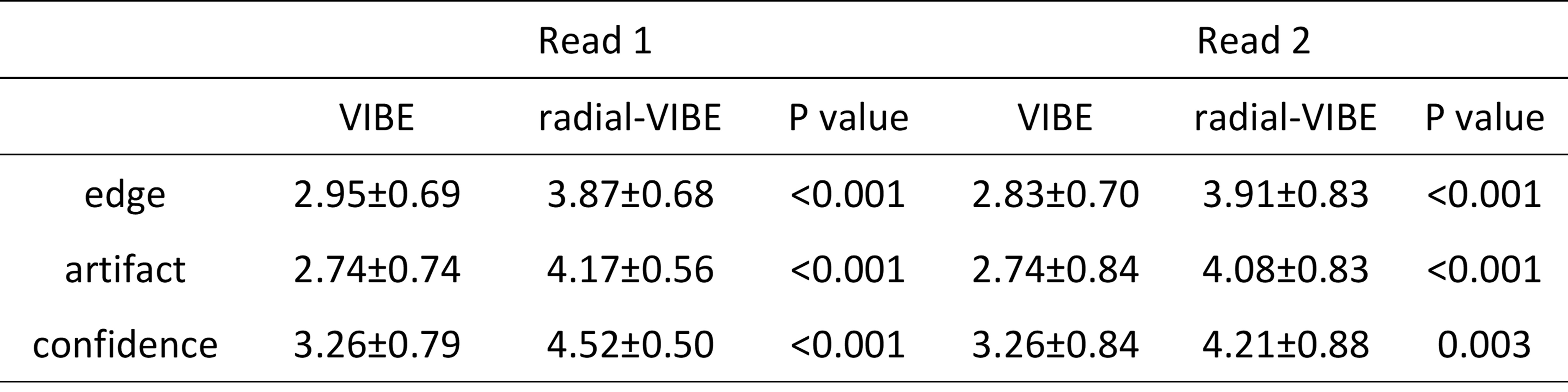
Table 1 Comparisons of edge of lesion, motion artifact, and diagnosis confidence between VIBE and radial-VIBE images.
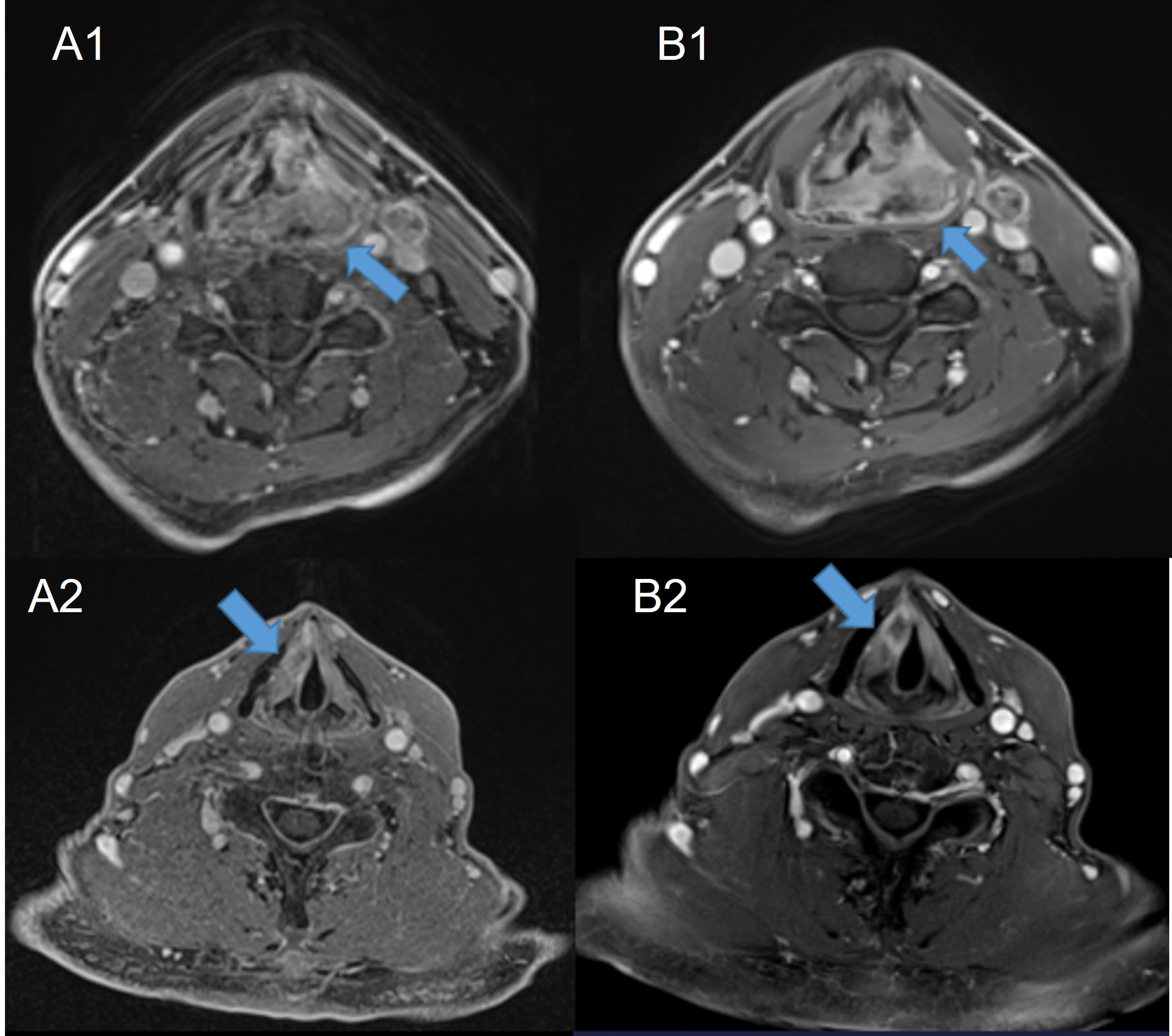
Figure 1. A1 and B1 are the conventional VIBE and radial-VIBE images for a 62-year-old male patient with hypopharyngeal carcinoma located in Left piriform fossa (arrow), respectively; A2 and B2 are the conventional VIBE and radial-VIBE images for a 73-year-old male patient with laryngeal carcinoma (arrow), respectively.
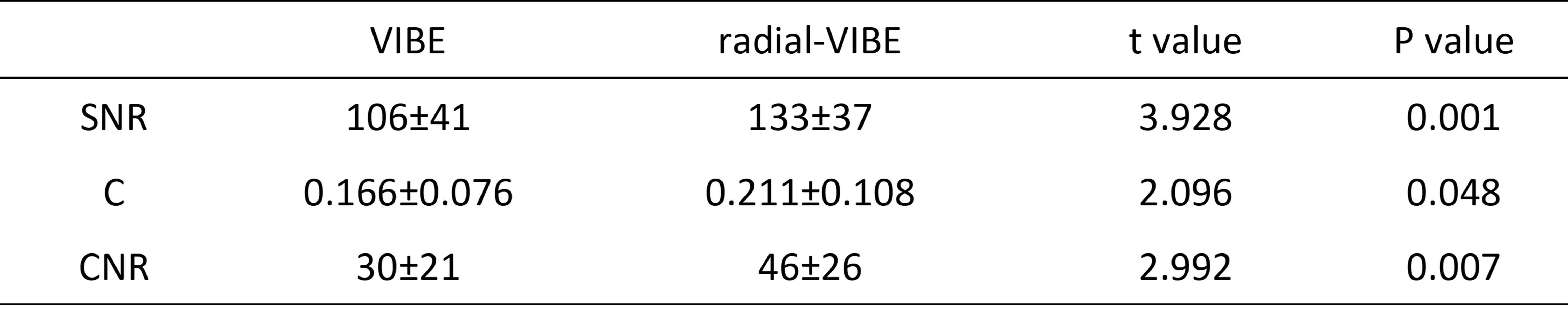
Table 2 Comparisons of SNR, C, and CNR between VIBE and radial-VIBE images.
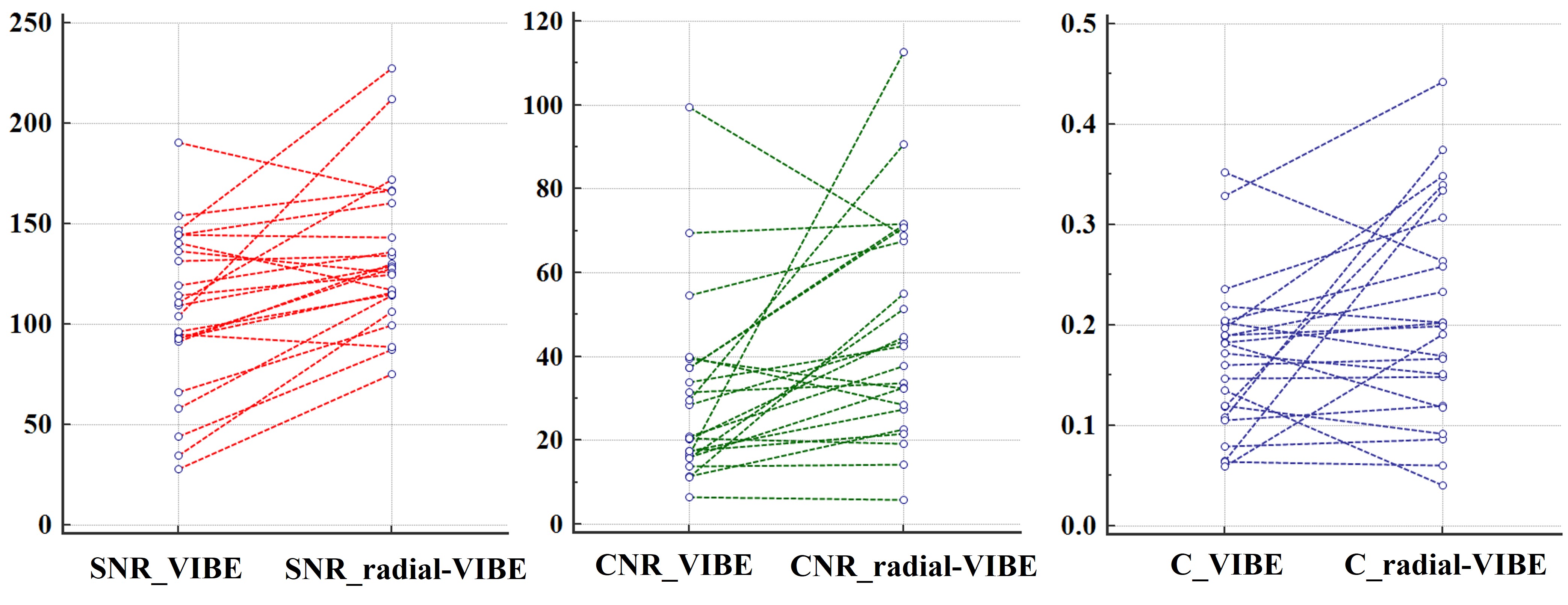
Figure 2. The scatter plot for SNR, C, and CNR between VIBE and radial-VIBE images.