4793
Free-Breathing Gadoxetic Acid-Enhanced Hepatobiliary Phase Imaging Using Stack-of-Stars Radial Sampling and Compressed SENSE
Tetsuro Kaga1, Yoshifumi Noda1, Nobuyuki Kawai1, Kimihiro Kajita2, Yu Ueda3, Masatoshi Honda3, Fuminori Hyodo4, Hiroki Kato1, and Masayuki Matsuo1
1Department of radiology, Gifu university, Gifu, Japan, 2Gifu university hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan, 4Institute for Advanced Study, Gifu university, Gifu, Japan
1Department of radiology, Gifu university, Gifu, Japan, 2Gifu university hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan, 4Institute for Advanced Study, Gifu university, Gifu, Japan
Synopsis
Keywords: Data Acquisition, Liver, Free breathing, Radial sampling
The gadoxetic acid-enhanced hepatobiliary phase imaging is an effective sequence for detecting hepatic lesions; however, degraded image quality is often observed due to poor breath holding. Free-breathing sequence using radial stack-of-stars acquisition (3D VANE) has been introduced and can provide diagnosable image quality. Recently, Compressed SENSE (CS), that is one of the acceleration techniques, has been applicable in 3D VANE. In this study, we evaluated the feasibility of 3D VANE with CS in hepatobiliary phase imaging. Our results showed that 3D VANE with CS at section thickness of 2 mm had almost comparable image quality as conventional breath-holding cartesian sampling.Purpose
The gadoxetic acid-enhanced hepatobiliary phase imaging is an effective imaging tool for detecting hepatic lesions1. However, degraded image quality is often observed due to poor breath holding, and thin slice data acquisition is difficult because of breath-holding acquisition sequence. The purpose of study was to evaluate the feasibility of newly adapted free-breathing sequence using radial stack-of-stars acquisition with spectral fat suppression (3D VANE)2 with Compressed SENSE (CS)3 in gadoxetic acid-enhanced hepatobiliary phase imaging.Materials and Methods:
This prospective study was approved by our Institutional Review Board, and written informed consent was obtained from all participants. Fourteen participants (10 men and 4 women, median age, 68 years; interquartile age range, 54–71 years) with suspected liver diseases underwent gadoxetic acid-enhanced MRI between June 2022 and September 2022 were included. Participants’ demographics are summarized in Table 1. All examinations were performed using a 3T MRI scanner (Ingenia 3.0T CX; Philips Healthcare) equipped with a 32-channel digital coil. The hepatobiliary phase imaging was scanned by conventional breath-holding sequence (BH group), 3D VANE with CS at section thickness of 4 mm (FB4mm group), and that of 2 mm (FB2mm group). Scanning parameters were detailed in Table 2. As navigator technique, the position of the diaphragm is automatically tracked, and the acquired data was corrected according to the monitored diaphragm positions in free-breathing sequence (track technique). The hepatobiliary phase image scanning was started after 15 minutes of contrast agent injection, and the order of the three sequences was randomly determined. For qualitative analysis, a radiologist, who was unaware of the scan sequence, randomly reviewed the images and assigned confidence scores for sharpness of the liver edge, visibility of intrahepatic vessels, motion artifacts, and overall image noise using a 5-point scale. For quantitative analysis, a radiologist measured mean signal intensity (SI) using region-of-interests (ROIs) placing on the liver parenchyma (SIliver) and paraspinal muscle (SImuscle). Standard deviation of SIliver (SDliver) was also measured. The signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated as SIliver/SDliver and (SIliver – SImuscle)/SDliver, respectively. The Freedman test for comparison among the three groups and Mann-Whitney U test with Bonferroni adjustment for post analysis were conducted. A P value of less than .05 for Freedman test and .017 for Mann-Whitney U test with Bonferroni adjustment were considered to be significant.Results
All qualitative and quantitative parameters were different among the three groups (P < .0001–.0021) (Tables 3 and 4). All qualitative parameters were higher in BH group than in FB4mm group (P < .0001–.016), but no difference was found between BH and FB2mm groups (P = .049–.38) and FB4mm and FB2mm groups (P = .027–.41). Median SIliver (P < .0001), SDliver (P < .0001), and SImuscle (P < .0001) were higher in FB4mm and FB2mm groups than in BH group, but no difference was found between FB4mm and FB2mm groups (P =.035–.52). Median SNR was higher in FB4mm group than in BH (P = .0003) and FB2mm groups (P = .0051), but no difference was found between BH and FB2mm groups (P = .14). The median CNR had no difference between each group (P = .017–.68).Discussion
Pseudo-golden-angle radial stack-of-stars acquisition comprised radial k-space sampling spaced at a constant azimuthal increment of approximately 111.25°. This angle related to the golden ratio with the added fine adjustment and causes radial lines to be very evenly spaced over time. Pseudo-golden-angle radial stack-of-stars acquisition could reduce motion artifacts compared with cartesian acquisition, but it led to prolonged acquisition time4. In this study, we applied 3D VANE with CS and track technique to the hepatobiliary phase scanning and as a result, it allowed shorter and within a fixed acquisition time (51 sec in FB4mm group and 81 sec in FB2mm group). In this study, qualitative scores were better in BH group than in FB4mm group, but FB2mm group showed almost comparable image quality to BH group. Additionally, we did not observe statistical difference in terms of the SNR and CNR between HB and FB2mm groups. Therefore, we believed that 3D VANE with CS at slice thickness of 2 mm could be applicable in clinical use and provides the usefulness for poor breath holding case.Conclusion
Free-breathing scanning using 3D VANE with CS and track technique was feasible in gadoxetic acid-enhanced hepatobiliary phase imaging. 3D VANE with CS at section thickness of 2 mm demonstrated almost comparable image quality compared with conventional breath-holding scans.Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
1. Joo I, Lee JM, Lee DH, et al. Retrospective validation of a new diagnostic criterion for hepatocellular carcinoma on gadoxetic acid-enhanced MRI: can hypointensity on the hepatobiliary phase be used as an alternative to washout with the aid of ancillary features? Eur Radiol 2019; 29: 1724–1732. 2. Winkelmann S, Schaeffter T, Koehler T, et al. An optimal radial profile order based on the golden ratio for time-resolved MRI. IEEE Trans Med Imaging 2007; 26:68–76. 3. Geerts-Ossevoort L, et al. Compressed SENSE Speed done right. Every time. The Netherlands: Philips Healthcare; 2018 Jan. Report No: 4522 991 31821. 4. Kajita K, Goshima S, Noda Y, et al. Thin-slice Free-breathing Pseudo-golden-angle Radial Stack-of-stars with Gating and Tracking T1-weighted Acquisition: An Efficient Gadoxetic Acid-enhanced Hepatobiliary-phase Imaging Alternative for Patients with Unstable Breath Holding. Magn Reson Med Sci 2019; 18; 4–11.Figures

Fugure 1. The case of 73 years old man hepatobiliary
phase images using (a) BH group, (b) FB4mm group, and (c) FB2mm
group. FB2mm group shows applicable image quality. FB4mm
group shows blurred liver edge and intrahepatic vessels. BH group shows good
image quality equivalent to FB2mm group.
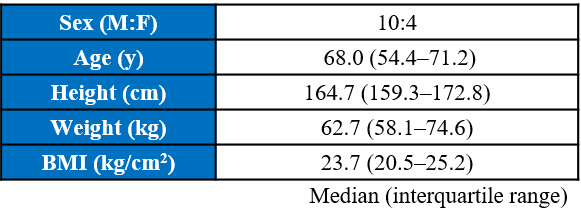
Table
1. Participants' demographics
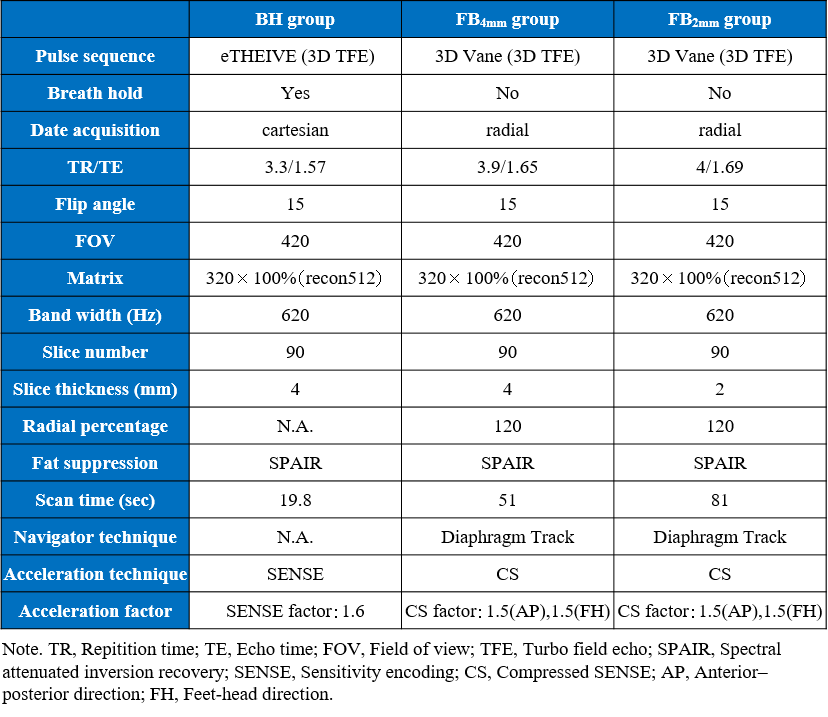
Table 2. MRI parameters for hepatobiliary phase imaging
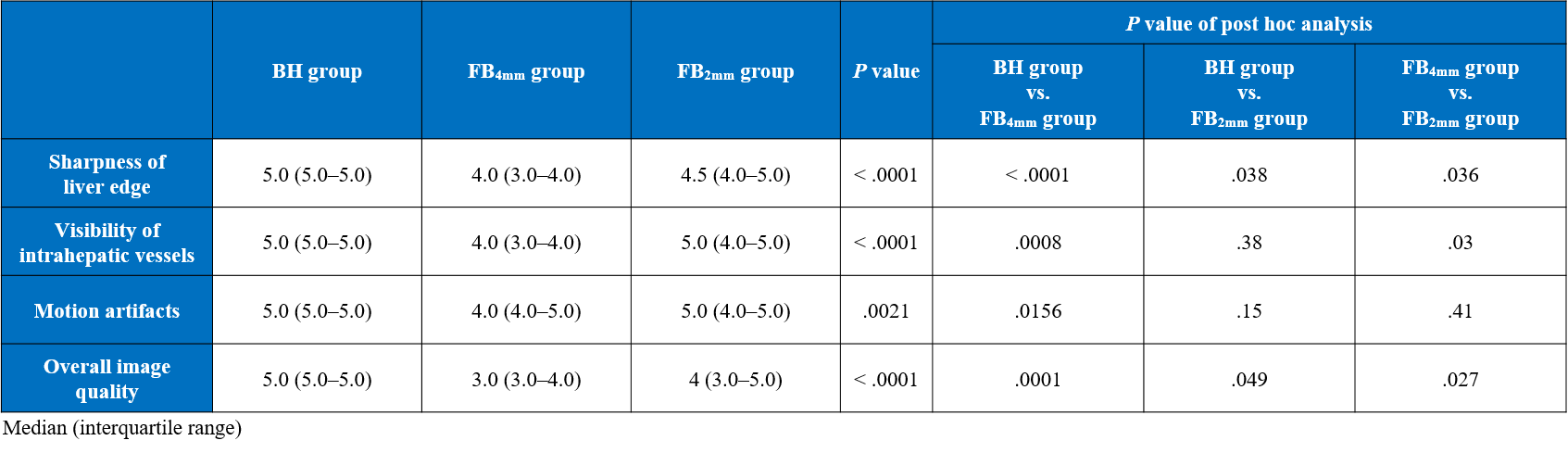
Table 3. Qualitative image analysis
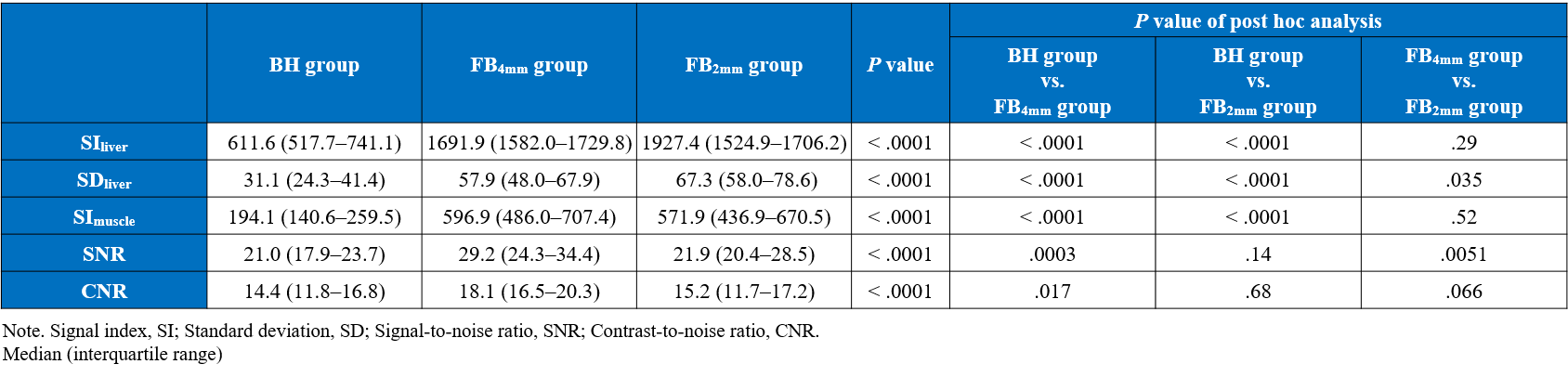
Table
4. Quantitative image analysis
DOI: https://doi.org/10.58530/2023/4793