4703
Heart Failure with Normal Natriuretic Peptide Levels and Preserved Ejection Fraction: A Prospective Clinical and CMR study1Fuwai hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Siemens Healthineers, Los Angeles, CA, United States, 3Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: Heart, Heart
The predisposed HFpEF has relatively unique clinical and CMR features, which indicates it may be an important subtype or precursor of HFpEF. However, the specific clinical significance of these features requires further prognostic studies.Abstract
PurposeDefining predisposed heart failure with preserved ejection fraction (HFpEF) with normal natriuretic peptide levels based on up-to-date ESC guidelines (reaching four points by HFA-PEFF score) using cardiovascular magnetic resonance (CMR) would be more accessible to understand its pathophysiology, yet scarcely been evaluated. This study therefore aimed to “phenomap” the clinical presentation and comprehensive CMR characteristics in patients with predisposed HFpEF.
Methods
We prospectively enrolled 464 participants including 213 patients with HFpEF, 151 patients with predisposed HFpEF, and 100 control subjects who underwent CMR. Participant data were obtained from electronic medical records or imaging post-processing. Comparisons of clinical- and CMR-based characteristics were made among three groups.
Results
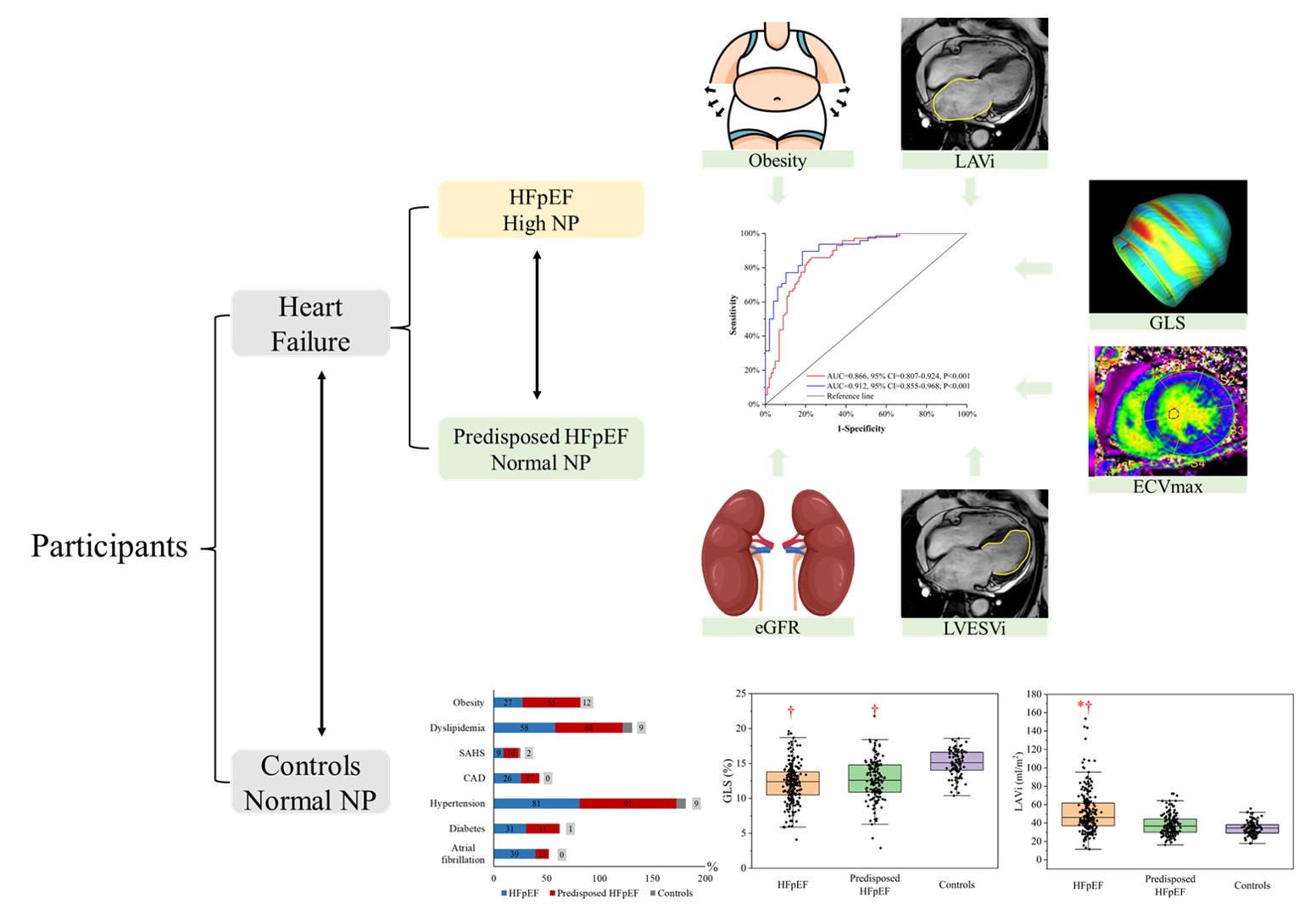
Compared with controls, patients with predisposed HFpEF were older, had higher body mass index, higher plasma volume, more comorbidities, and worse left ventricular (LV) remodeling and function. There were no differences in sex or NYHA functional class between patients with HFpEF and predisposed HFpEF. Compared with patients with HFpEF, patients with predisposed HFpEF were younger (50±14 vs 59±14 years), had higher plasma volume (2789.0±351.6 vs 2637.0±374.9 ml), higher prevalence of hypertension (91.4% vs 81.2%), and obesity (55.0% vs 27.2%), yet lower prevalence of atrial fibrillation (12.6% vs 39.4%), and less impaired LV global longitudinal strain (GLS, -12.2±2.8% vs -12.7±2.9%), lower left atrial maximal volume index (LAVi, 38.3±11.2 vs 52.0±23.1 ml/m2), and maximal extracellular volume fraction (ECVmax, 47.6±8.9% vs 52.5±10.7%, all p<0.05), which was much aligned with the propensity-score matching cohort. In a multivariable logistic model, obesity, LAVi, GLS, and ECVmax were independently associated with the identification of patients with predisposed HFpEF (AUC=0.866, p<0.001).
Discussion
This relatively large scale prospective observational study revealed several important facts existing in the real-world HFpEF: 1) Patients with predisposed HFpEF and normal natriuretic peptide levels accounted for an unneglectable part in overall heart failure cohort; 2) Compared with controls, the predisposed HFpEF patients manifested higher volume load, more comorbidities, worse cardiac remodeling and function; 3) Compared with typical HFpEF, predisposed HFpEF patients showed more prevalence of obesity, and CMR derived LAVi, GLS, and ECVmax were independently associated with the predisposed HFpEF cohort (Figure 4), holding the potential to monitor status of this important phenotype. However, the specific clinical significance of these features requires further prognostic studies.
Although the gold diagnostic standard of HFpEF was cardiac catheter examination, its main use is limited to the research setting with invasiveness and radiation. Hence, we introduced a new and clinical-based cohort of the predisposed HFpEF patients with normal NP levels on the non-invasive HFA-PEFF score in the latest ESC guidelines. This predisposed HFpEF cohort satisfied the cardiac diastolic dysfunction and cardiac remodeling, reaching 4 points in HFA-PEFF score. In the clinical setting, we found the predisposed HFpEF patients with normal NP were common in the HF cohort with preserved ejection fraction (42%), higher than the proportion (up to 20%) of patients with catheter proven HFpEF. This may be attributable to different diagnostic criteria of HFpEF patients by ESC guidelines in our study, and the inclusion of our participants were accessible and easy-to-implemented in the clinical setting. The clinical presentation, myocardial function and tissue features of these predisposed HFpEF patients were scarcely understood, hindering the specific treatment. Consistent to previous study, we found the predisposed HFpEF patients had higher volume load, more common comorbidities compared to controls. Compared to typical HFpEF patients, the predisposed HFpEF patients were younger, showed better renal dysfunction, more common prevalence of hypertension and obesity, yet less common of atrial fibrillation. This may be part of related to normal NP levels in the predisposed HFpEF patients. In addition, our study further demonstrated the independent association of obesity and renal function with the predisposed HFpEF, explaining the normal NP levels in patients with predisposed HFpEF and obesity, congruous to previous studies, and new markers or its combination were needed to diagnose HFpEF with normal NP levels without obesity.
Regarding to structural and functional alterations, CMR took unique advantages in demonstrating subclinical dysfunction and myocardial tissue characteristics through myocardial strain and ECV. The predisposed HFpEF patients showed significant LV enlargement, yet similar LVMi compared to HFpEF patients in the real cohort. According to previous studies, this might be explained by younger age and more prevalence of hypertension in the predisposed HFpEF patients, as only LVMi remained significantly different in the PSM cohort after adjusting age, atrial fibrillation, and hypertension. Besides, our study firstly illustrated the CMR imaging features of the predisposed HFpEF patients, who showed less impaired LAVi, GLS, sGLSR, and ECVmax compared to HFpEF patients, consistent to the results derived from the PSM cohort. Besides, the multivariable logistic regression model also proved the independent association of LAVi, GLS, and ECVmax and the predisposed HFpEF patients. Hence, we speculated that LAVi, GLS, and ECVmax would be reliable and sensitive markers to monitor the status of the predisposed HFpEF patients.
Conclusions
The predisposed HFpEF has relatively unique clinical and CMR features, which indicates it may be an important subtype or precursor of HFpEF. However, the specific clinical significance of these features requires further prognostic studies.
Acknowledgements
N/AReferences
1. Pokharel Y, Khariton Y, Tang Y, et al. Association of Serial Kansas City Cardiomyopathy Questionnaire Assessments With Death and Hospitalization in Patients With Heart Failure With Preserved and Reduced Ejection Fraction: A Secondary Analysis of 2 Randomized Clinical Trials. JAMA Cardiology 2017;2(12):1315-21.
2. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42(36):3599-726.
3. Clerico A, Zaninotto M, Passino C, Plebani M. Obese phenotype and natriuretic peptides in patients with heart failure with preserved ejection fraction. Clin Chem Lab Med 2018;56(7):1015-25.
4. Verbrugge FH, Omote K, Reddy YNV, Sorimachi H, Obokata M, Borlaug BA. Heart failure with preserved ejection fraction in patients with normal natriuretic peptide levels is associated with increased morbidity and mortality. Eur Heart J 2022;43(20):1941-51.
5. Pieske B, Tschöpe C, de Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J 2019;40(40):3297-317.
6. Rademakers FE. Magnetic resonance imaging in cardiology. Lancet 2003;361(9355):359-60.
7. He J, Sirajuddin A, Li S, et al. Heart Failure With Preserved Ejection Fraction in Hypertension Patients: A Myocardial MR Strain Study. J Magn Reson Imaging 2021;53(2):527-39.
8. Claus P, Omar AMS, Pedrizzetti G, Sengupta PP, Nagel E. Tissue Tracking Technology for Assessing Cardiac Mechanics: Principles, Normal Values, and Clinical Applications. JACC Cardiovasc Imaging 2015;8(12):1444-60.
9. DeVore AD, McNulty S, Alenezi F, et al. Impaired left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: insights from the RELAX trial. Eur J Heart Fail 2017;19(7):893-900.
10. He J, Yang W, Wu W, et al. Early Diastolic Longitudinal Strain Rate at MRI and Outcomes in Heart Failure with Preserved Ejection Fraction. Radiology 2021;301(3):582-92.
11. Roy C, Slimani A, de Meester C, et al. Associations and prognostic significance of diffuse myocardial fibrosis by cardiovascular magnetic resonance in heart failure with preserved ejection fraction. J Cardiovasc Magn Reson 2018;20(1):55.
12. Ling HZ, Flint J, Damgaard M, et al. Calculated plasma volume status and prognosis in chronic heart failure. Eur J Heart Fail 2015;17(1):35-43.
13. Xu J, Zhuang B, Sirajuddin A, et al. MRI T1 Mapping in Hypertrophic Cardiomyopathy: Evaluation in Patients Without Late Gadolinium Enhancement and Hemodynamic Obstruction. Radiology 2020;294(2):275-86.
14. Petersen SE, Khanji MY, Plein S, Lancellotti P, Bucciarelli-Ducci C. European Association of Cardiovascular Imaging expert consensus paper: a comprehensive review of cardiovascular magnetic resonance normal values of cardiac chamber size and aortic root in adults and recommendations for grading severity. Eur Heart J Cardiovasc Imaging 2019;20(12):1321-31.
15. D'Agostino RB, Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med 1998;17(19):2265-81.
16. Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J, Hannan EL. Everolimus-eluting stents or bypass surgery for multivessel coronary disease. N Engl J Med 2015;372(13):1213-22.
17. Shah SJ. BNP: Biomarker Not Perfect in heart failure with preserved ejection fraction. Eur Heart J 2022;43(20):1952-4.
18. Vaishnav J, Chasler JE, Lee YJ, et al. Highest Obesity Category Associated With Largest Decrease in N-Terminal Pro-B-Type Natriuretic Peptide in Patients Hospitalized With Heart Failure With Preserved Ejection Fraction. J Am Heart Assoc 2020;9(15):e015738.
19. Keyzer JM, Hoffmann JJ, Ringoir L, Nabbe KC, Widdershoven JW, Pop VJ. Age- and gender-specific brain natriuretic peptide (BNP) reference ranges in primary care. Clin Chem Lab Med 2014;52(9):1341-6.
20. Verbrugge FH, Borlaug BA. Heart failure with normal natriuretic peptide levels: more fat, and that is the main problem. Eur Heart J 2022;43(23):2248-9.
21. Olivella A, Méndez AB, Ferreira-González I. Mixing the fat with water: are normal natriuretic peptide heart failure with preserved ejection fraction patients just more obese? Eur Heart J 2022;43(23):2247-.
22. Zhuang B, Li S, Xu J, et al. Age- and Sex-Specific Reference Values for Atrial and Ventricular Structures in the Validated Normal Chinese Population: A Comprehensive Measurement by Cardiac MRI. J Magn Reson Imaging 2020;52(4):1031-43.
23. Yildiz M, Oktay AA, Stewart MH, Milani RV, Ventura HO, Lavie CJ. Left ventricular hypertrophy and hypertension. Prog Cardiovasc Dis 2020;63(1):10-21.
Figures