4701
Differential diagnosis for hypertrophic cardiomyopathy and hypertensive heart disease by layer-specific CMR strain analysis1Taiyuan Central Hospital of Shanxi Medical University, Taiyuan, China, 2Siemens Healthineers Ltd., Beijing, China
Synopsis
Keywords: Heart, Cardiomyopathy
This study evaluated the left ventricle (LV) and right ventricle (RV) layer-specific (endocardium=Endo, epicardium=Epi, myocardium=Myo) strain of hypertrophic cardiomyopathy (HCM) and hypertensive heart disease (HHD). We also evaluated the ability of left atrium (LA) to differentiate HCM and HHD. The strain and strain rate were calculated from CMR. The difference of LV between HCM and HHD was endocardium. The difference of RV was free wall epicardium. The difference of LA was LA strain at conduit phase (LAS-cd). Combining the LV global circumferential strain rate of endocardium (GCSR-Endo) and LASR-cd can better differentiate HCM and HHD.
Introduction
HCM is the most common inherited cardiomyopathy1. According to the guidelines of the European Society of Cardiology,HCM is diagnosed by unexplained left ventricular hypertrophy (LVH) and a maximum wall thickness ≥ 15 mm2. HHD is characterized by extensive structural remodeling and increased LV wall thickness (LVWT) due to the afterload 2,3. Before the late stage of the disease, HHD and HCM showed normal systolic function through routine measurements4,5. However, the early decline in myocardial mechanics measured by strain analysis has been observed in both6,7. HCM and HHD are both associated with LVH, which makes diagnosis difficult 5,8 .Accurate evaluation of cardiac anatomy by computed tomography, cardiac magnetic resonance, or 2D transthoracic echocardiography is essential to differential diagnosis of HCM and HHD. However, traditional tools are not sensitive enough to analyze the mechanism of structural and functional abnormalities at the level of hypertrophied myocardium. Cardiovascular magnetic resonance feature tracking (CMR-FT) is a solution for high-resolution assessment of global and regional myocardial strain analysis. CMR-FT tracks the epicardial and endocardial borders and has been evaluated in a wide range of cardiovascular diseases9. Myocardium can be divided into endocardial, mid myocardial and epicardial layers. Previous studies have demonstrated that global longitudinal strain can differentiate HCM from HHD 10. However, there is gradient in transmural myocardial strain, and the value from endocardium to epicardium decreases gradually11,12. The purpose of this study was to clarify detailed mechanisms of structural between HCM and HHD using layer-specific strain and combined it with LA strain to differentiate the two diseases.Methods
There were 29 patients of HCM, 11patients of HHD and 21 healthy volunteers were included. Cardiovascular MR was performed for all patients and volunteers with a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) and 18 channels phased array coil. Balanced steady state free precession sequence (bSSFP) and prospective ECG triggering was used to achieve short axis, two chamber, three chamber and four chamber cardiac cine (Figure 1). Typical imaging parameters were as follow: repetition time (TR)=45.64 ms, echo time (TE)=1.43 ms, flip angle (FA)=61°, slice thickness=8 mm, field of view (FOV)=340 mm × 274 mm, matrix=208 × 118, average=1. Medis Medical Imaging (Suite 4.0, Leiden, the Netherlands) was used to evaluate the strain of LV, RV and LA. We calculated the layer-specific strain and strain rate at both end systole (ES) and end diastole (ED) by CMR-FT. We also evaluated the strain and strain rate of RV and LA. The RV myocardium was additionally divided into septal and free walls. The strain of LA includes LA strain at booster-pump phase (LAS-bp), conduit phase (LAS-cd) and reservoir phase (LAS-r). Independent t-test or Mann Whitney U test was used to compare the myocardial strain between the two groups. Multiple regression analysis was used to test the diagnostic ability of CMR parameters for two diseases. The multivariate logistic regression analysis was calculated to test the diagnostic ability of CMR parameters for distinguishing the two diseases. The area under the curves (AUCs), specificity, sensitivity, and Youden’s index were analyzed by the receiver operating characteristic curve (ROC). All the data were calculated by SPSS (version 26.0.0, International Business Machines, Armonk, New York, USA). P<0.05 was considered as statistically significant.Results
The LV GCSR-Endo (2.4 ± 0.1), and the RV free wall strain rate of epicardium (FWSR-Epi) (1.2 ± 0.1) in HCM were statistically higher than that in HHD. The LAS-cd 10.8 (6.2~15.2) and the LASR-cd -0.4 (-0.6~-0.3) of HCM was statically lower than that of HHD (Table 1). The AUC of LAS-cd was the highest (AUC=0.806). When combined with the GCSR-Endo and LASR-cd, the diagnostic efficacy was the highest (AUC=0.871) (Table 2).Discussion
Previous study demonstrated that CMR-FT GLS can differentiate HHD from HCM 10. Combining Late Gadolinium Enhancement and GRS can better differentiates the two diseases 13.In our study, myocardial strain were divided into different layers to differentiate HCM and HHD. The difference of LV endocardium between HCM and HHD indicated that the change of endocardium in these two diseases is more obvious than that in epicardium and myocardial. The difference of RV free wall strain rate at epicardium indicated that the two diseases may affect the strain of the RV and have greater impact on epicardium. These two diseases can affect the strain of LA, and their differences is at conduit phase.Conclusion
Layer-specific CMR-FT can differentiate HCM and HHD, and LVH can affect the RV strain. Combining the LV GCSR-Endo and LASR-cd can better differentiate HCM and HHD.Acknowledgements
No acknowledgement found.References
1. Maron BJ. Clinical Course and Management of Hypertrophic Cardiomyopathy. N Engl J Med. 2018;379(20):1977.
2. Authors/Task Force members, Elliott PM, Anastasakis A, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(39):2733-2779.
3. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertens Dallas Tex 1979. 2003;42(6):1206-1252.
4. Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(24):2761-2796.
5. Jc R, Am A, Ag D, et al. Comprehensive characterisation of hypertensive heart disease left ventricular phenotypes. Heart Br Card Soc. 2016;102(20).
6. Kuruvilla S, Janardhanan R, Antkowiak P, et al. Increased extracellular volume and altered mechanics are associated with LVH in hypertensive heart disease, not hypertension alone. JACC Cardiovasc Imaging. 2015;8(2):172-180.
7. Kato TS, Noda A, Izawa H, et al. Discrimination of nonobstructive hypertrophic cardiomyopathy from hypertensive left ventricular hypertrophy on the basis of strain rate imaging by tissue Doppler ultrasonography. Circulation. 2004;110(25):3808-3814.
8. Giusca S, Steen H, Montenbruck M, et al. Multi-parametric assessment of left ventricular hypertrophy using late gadolinium enhancement, T1 mapping and strain-encoded cardiovascular magnetic resonance. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2021;23(1):92.
9. Schuster A, Hor KN, Kowallick JT, Beerbaum P, Kutty S. Cardiovascular Magnetic Resonance Myocardial Feature Tracking: Concepts and Clinical Applications. Circ Cardiovasc Imaging. 2016;9(4):e004077.
10. Neisius U, Myerson L, Fahmy AS, et al. Cardiovascular magnetic resonance feature tracking strain analysis for discrimination between hypertensive heart disease and hypertrophic cardiomyopathy. PloS One. 2019;14(8):e0221061.
11. Shi J, Pan C, Kong D, Cheng L, Shu X. Left Ventricular Longitudinal and Circumferential Layer-Specific Myocardial Strains and Their Determinants in Healthy Subjects. Echocardiogr Mt Kisco N. 2016;33(4):510-518.
12. Tanacli R, Hashemi D, Lapinskas T, et al. Range Variability in CMR Feature Tracking Multilayer Strain across Different Stages of Heart Failure. Sci Rep. 2019;9(1):16478.
13. Liu S, Li Y, Zhao Y, et al. The Combination of Feature Tracking and Late Gadolinium Enhancement for Identification Between Hypertrophic Cardiomyopathy and Hypertensive Heart Disease. Front Cardiovasc Med. 2022;9:865615.
Figures
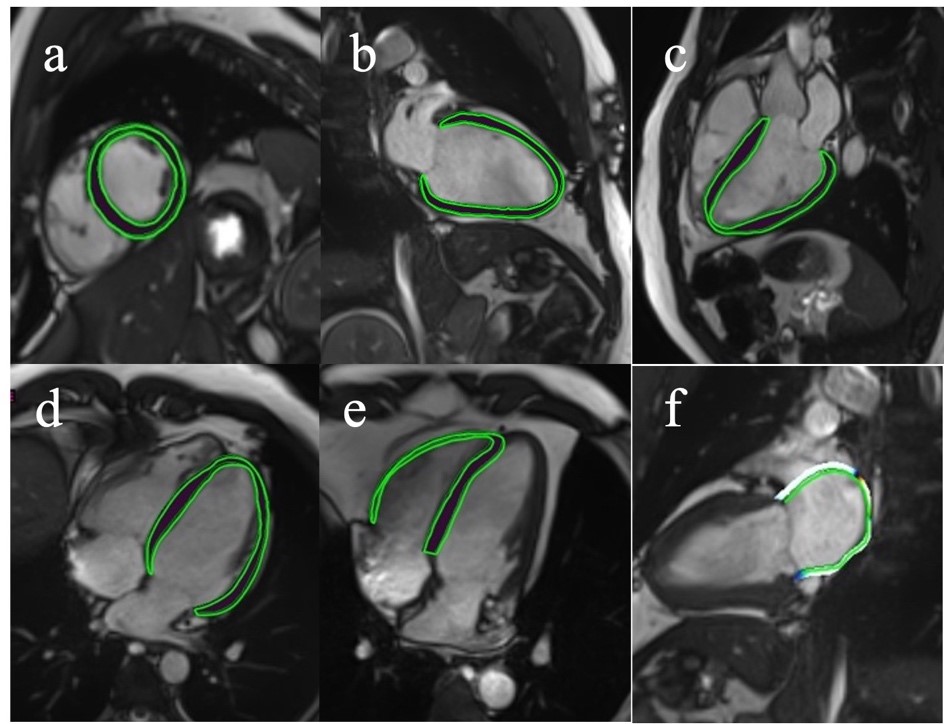
Figure 1. Feature-tracking biventricular strain analysis. Feature tracking was used to analyze the strain from short axis cine and two chamber, three chamber and four chamber cine views acquired with CMR. (a), (b), (c), (d) LV short axis cine and two chamber, three chamber and four chamber cine views acquired by CMR. (e) RV of four chamber cine view. (f) LA two chamber cine view.
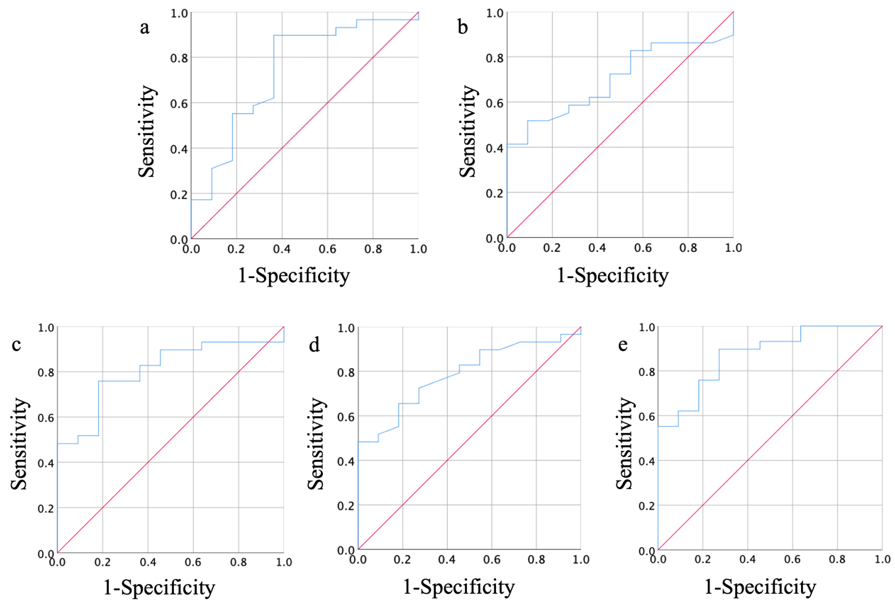
Figure 2. (a) AUC of GCSR-Endo, (b) AUC of FWSR-Epi, (c) AUC of LAS-cd, (d) AUC of LASR-cd, (e) AUC of GCSR-Endo and LASR-cd.
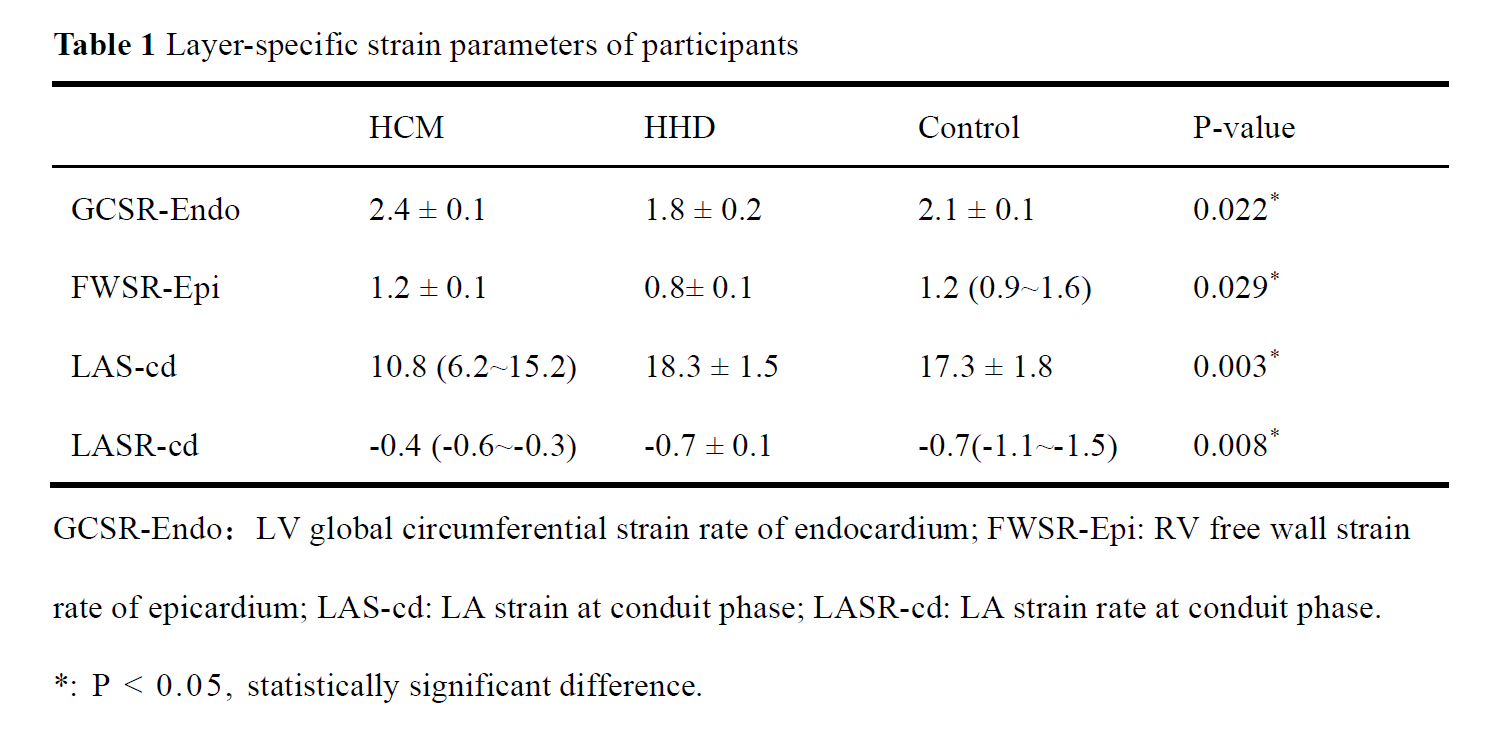
Table 1 Layer-specific strain parameters of participants.
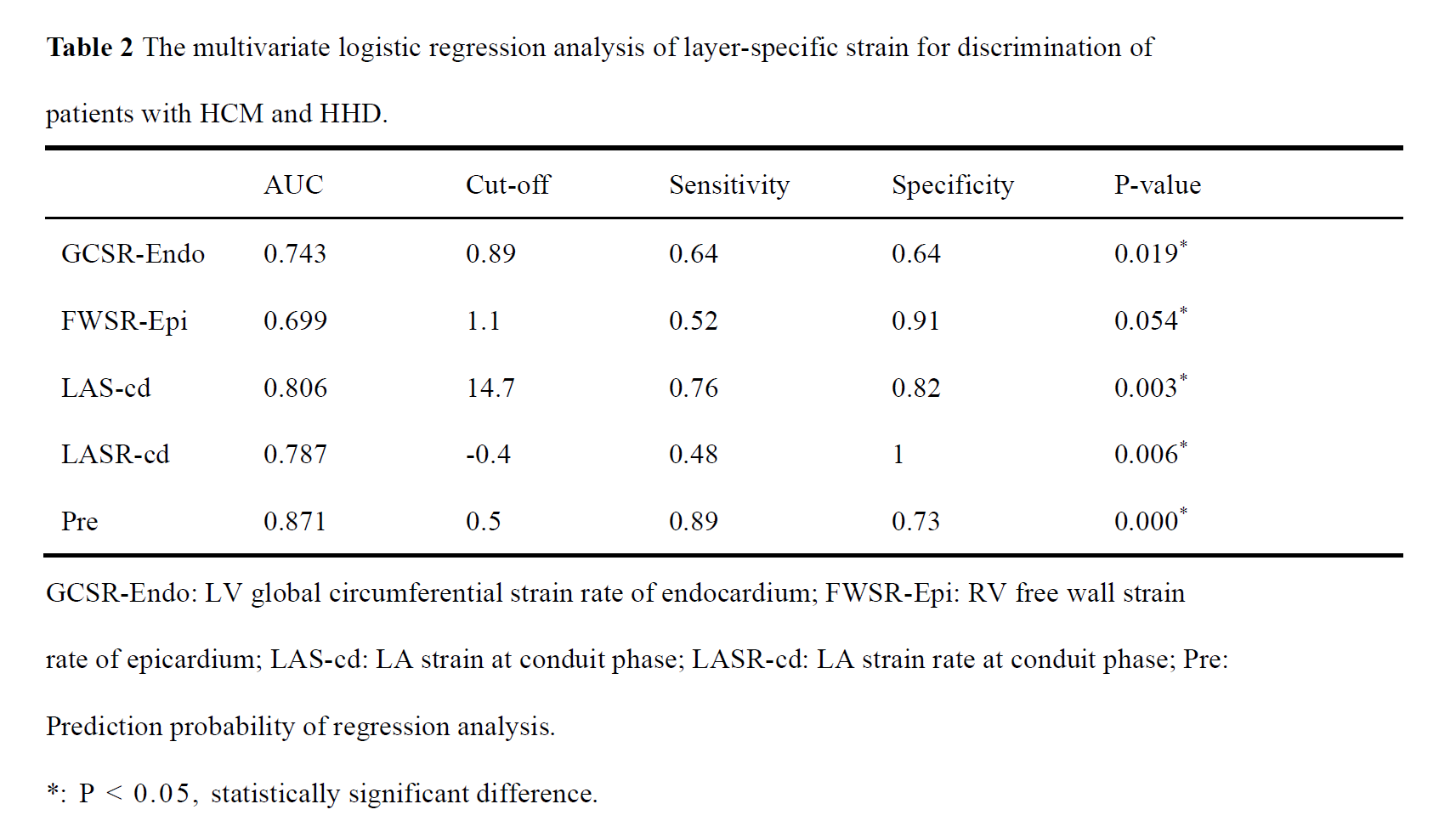
Table 2 The multivariate logistic regression analysis of layer-specific strain for discrimination of patients with HCM and HHD.