4699
Reverse Remodeling of Left Atrium Assessed by Cardiac MR Feature Tracking in Hypertrophic Obstructive Cardiomyopathy after Septal Myectomy
Shujuan Yang1 and Shihua Zhao1
1Fuwai Hospital, Beijing, China
1Fuwai Hospital, Beijing, China
Synopsis
Keywords: Cardiomyopathy, Surgery
Eighty-eight patients with hypertrophic obstructive cardiomyopathy(HOCM) who received CMR before and after myectomy were retrospectively studied. Thier Pre- and postmyectomy left atrial (LA) parameters derived from CMR-feature tracking were compared. Patients with HOCM after septal myectomy showed LA reverse remodeling with a reduction in LA size and restoration in LA reservoir and booster function but unchanged LA conduit function. Among volumetric and functional changes, booster function had the greatest improvement postoperatively. Besides, preoperative LAVmin index and ΔLVOT might be potential factors associated with the degree of improvement in εa.Background
Assessing the structure and function of left atrium (LA) is crucial in hypertrophic obstructive cardiomyopathy (HOCM) because LA remodeling correlates with atrial fibrillation1,2. Cardiac magnetic resonance (CMR) has been established as the gold standard imaging modality for assessing LA structure and function because of its high spatial resolution and superior tissue contrast in providing an accurate anatomic definition of thin asymmetric LA wall. Using routine cine images, CMR feature tracking (FT) is capable of quantifying LA volume and deformation parameters in different phases during the cardiac cycle. However, few studies have investigated the potential effect of myectomy on LA phasic remodeling in HOCM after myectomy using cardiac magnetic resonance (CMR) feature tracking (FT). This study aims to evaluate the LA structural and functional remodeling with HOCM after myectomy by CMR-FT and to further investigate the determinants of LA reverse remodeling.Methods
In this single-center study, we retrospectively studied 88 patients with HOCM who received CMR before and after myectomy between January 2011 and June 2021. Preoperative and postoperative LA parameters derived from CMR-FT were compared(Figur 1A), including LA reservoir function (total ejection fraction [EF], total strain [εs], peak positive strain rate [SRs]), conduit function (passive EF, passive strain [εe], peak early negative strain rate [SRe]) and booster function (booster EF, active strain [εa], late peak negative strain rate [SRa]). Eighty-six healthy participants were collected for comparison. Typical LA deformation parameter curves in a healthy subject are depicted in Figur 1B.Univariate and multivariate linear regression identified variables associated with the rate of change of εa. Furthermore, we investigated the rates of change in LA parameters, as they had different units and baseline levels, to assess the extent of improvement following myectomy.Results
Preoperative CMR was performed at a median of 14 days (IQR, 6 to 33 days) before myectomy. The interval between the pre- and postmyectomy CMR was at a median of 1.14 years (IQR, 1.01 to 1.56 years). Compared with preoperative parameters, LA anteroposterior diameter, LA left-right diameter, LAVmin, LAVpac, and LAVmax were significantly decreased after myectomy (all P<0.001). When comparing phasic functions, the LA reservoir function (LA total EF, εs, SRs) and booster function (LA booster EF, εa, SRa) were significantly improved postoperatively (all P<0.05), but LA conduit function (LA passive EF, εe) was relatively preserved after myectomy, except for SRe [premyectomy, -0.48 (IQR, -0.32 to -0.74) s-1 vs. postmyectomy, -0.58 (IQR, -0.41 to -0.77) s-1, P=0.007]. A representative case of LA phasic deformation function curves before and after myectomy is shown in Figure 2. Although most LA indices improved after surgery, they were still worse than healthy controls (all P<0.05). In univariate analysis, systolic blood pressure, LAVmin index, ΔMR degree, and ΔLVOT pressure gradient were significantly associated with the rate of change of εa (all P<0.05). In multivariate analysis, LAVmin index (adjusted β =-0.39, P<0.001) and ΔLVOT pressure gradient (adjusted β =-0.29, P=0.003) were significantly and independently related to the rate of change of εa. As shown in Figure 3A, LA boost function, especially εa, showed the most dramatic improvement exceeding those seen in reservoir function, conduit function, and volume. After dividing patients into two subgroups according to whether ΔNYHA class was ≥2, the rate of change of εa in ΔNYHA class ≥2 group was significantly greater than the rate in ΔNYHA class <2 group (P=0.037). However, no statistical differences were observed when comparing other LA parameters (Figure 3B).Conclusions
Our study demonstrated the feasibility of CMR-FT in assessing LA remodeling in patients with HOCM after septal myectomy. After successfully eliminating LVOT obstruction, they benefited from the relief of symptoms and partially recovered LA remodeling with a reduction in LA size and improvement in LA reservoir and booster function, whereas the LA conduit function seemed to be preserved. The improvement in LA boost function was beyond the improvement in reservoir function, conduit function, and atrial size following myectomy. Besides, preoperative LAVmin index and ΔLVOT might be potential factors associated with the degree of improvement in LA active strain. Future studies are needed to verify whether septal myectomy prevents the progression of AF in HOCM patients with postoperative LA reverse remodeling.Acknowledgements
N/AReferences
1. Raman B, Smillie RW, Mahmod M, Chan K, Ariga R, Nikolaidou C, et al. Incremental value of left atrial booster and reservoir strain in predicting atrial fibrillation in patients with hypertrophic cardiomyopathy: a cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2021;23:109.
2. Kramer CM, DiMarco JP, Kolm P, Ho CY, Desai MY, Kwong RY, et al. Predictors of major atrial fibrillation endpoints in the National Heart, Lung, and Blood Institute HCMR. JACC Clin Electrophysiol. 2021;7:1376-1386.
Figures
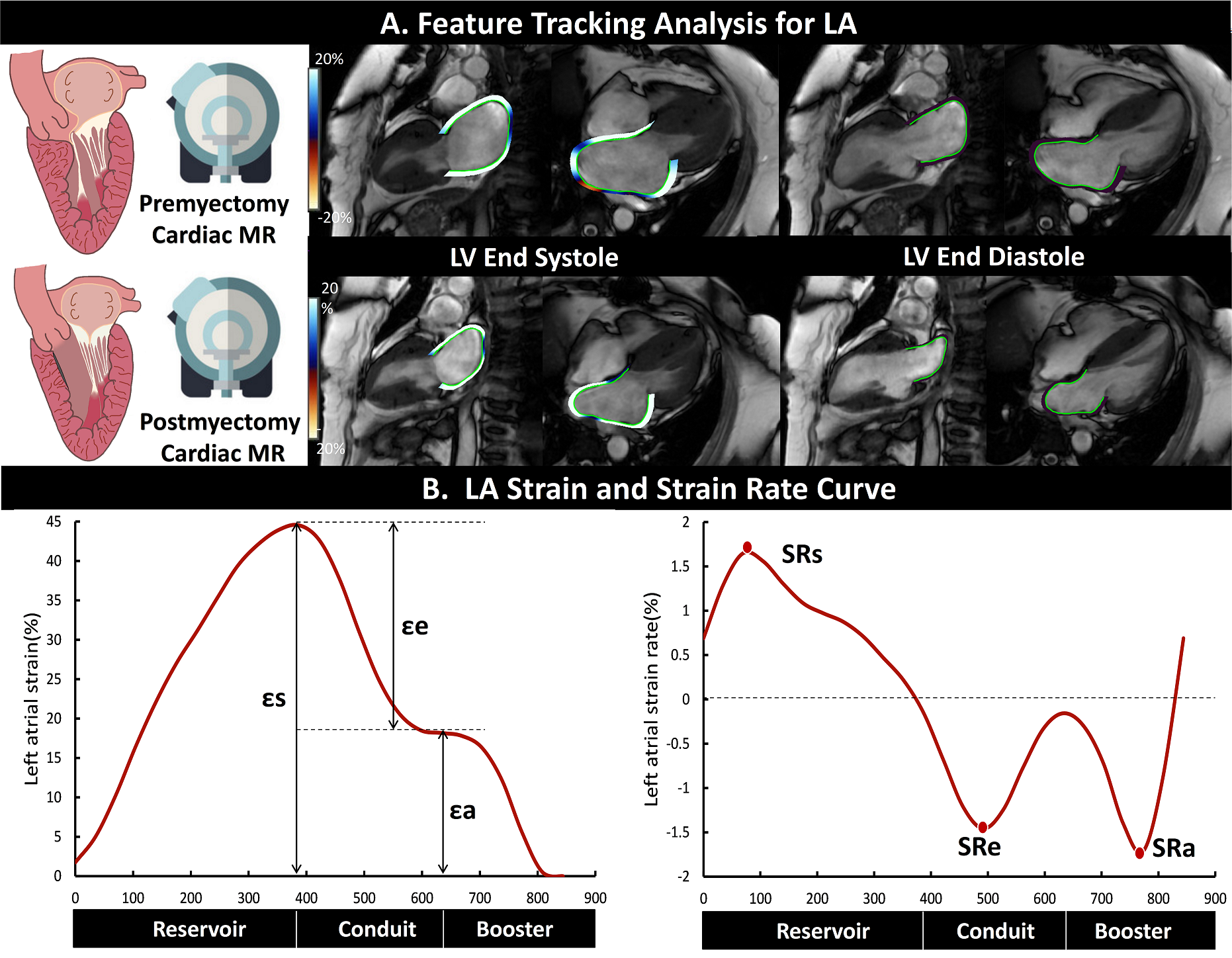
Figure 1: Example of measurement of LA phasic deformation function
by feature tracking (A): the LA contours were semi-automatically delineated
with manual adjustment at the phase of LV end-systole and end-diastole
on the two- and four-chamber cine images. Curves of feature
tracking-derived LA strain and strain rate in different phases during the
cardiac cycle in a healthy participant (B). LA = left atrial, LV = left
ventricular.
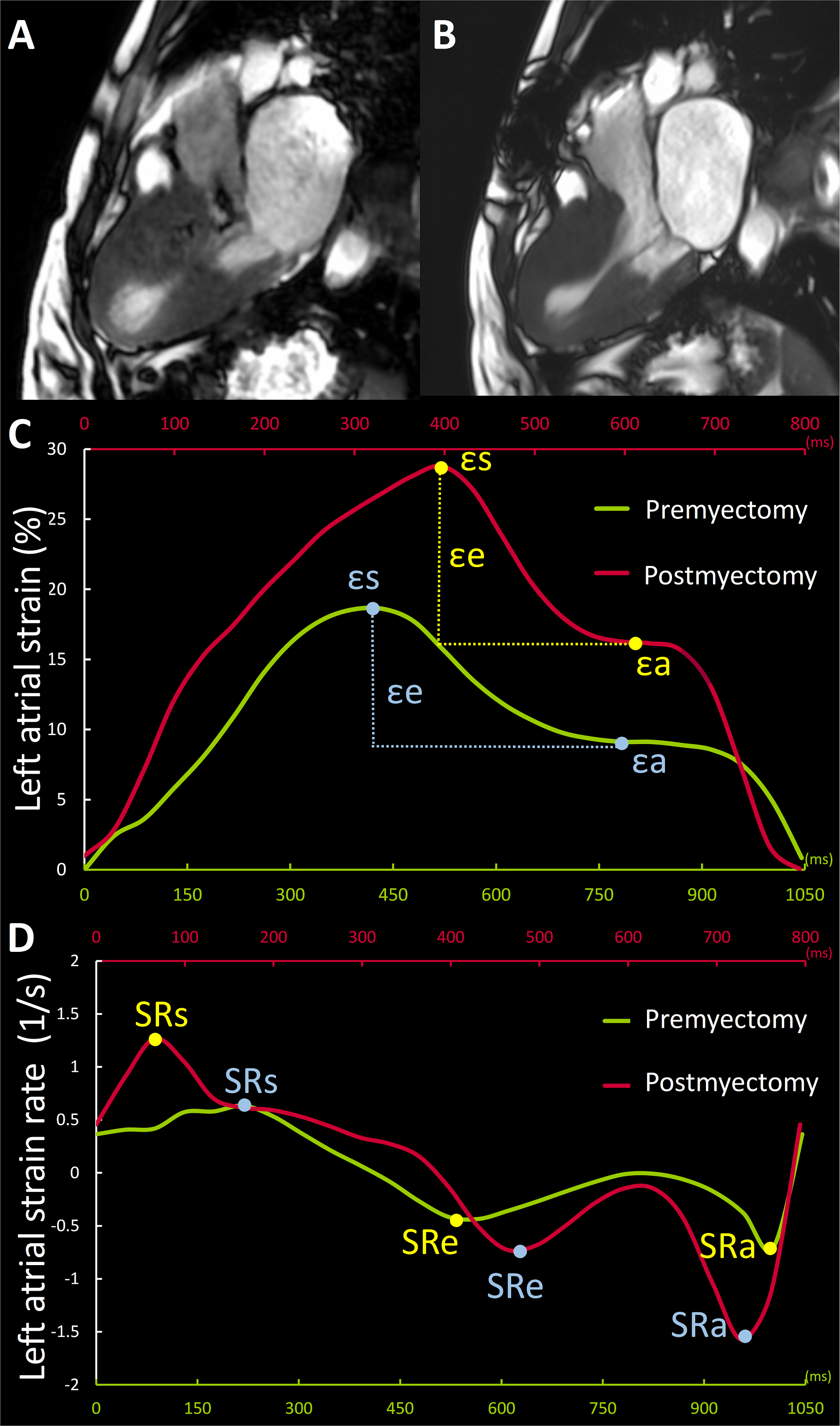
Figure 2: Representative case (52-year-old female) of a patient
with hypertrophic obstructive cardiomyopathy who underwent septal myectomy. Upper row displays the LVOT cine images at late
systole. SAM of mitral valve can be seen in preoperative cine (A). After
surgery, LVOT is unobstructed without SAM (B). Lower rows display the curves of
preoperative (in red) and postoperative (in green) left atrial strain (C) and
strain rate (D) over the cardiac cycle.
LVOT=left ventricular outflow tract, SAM=systolic anterior motion.
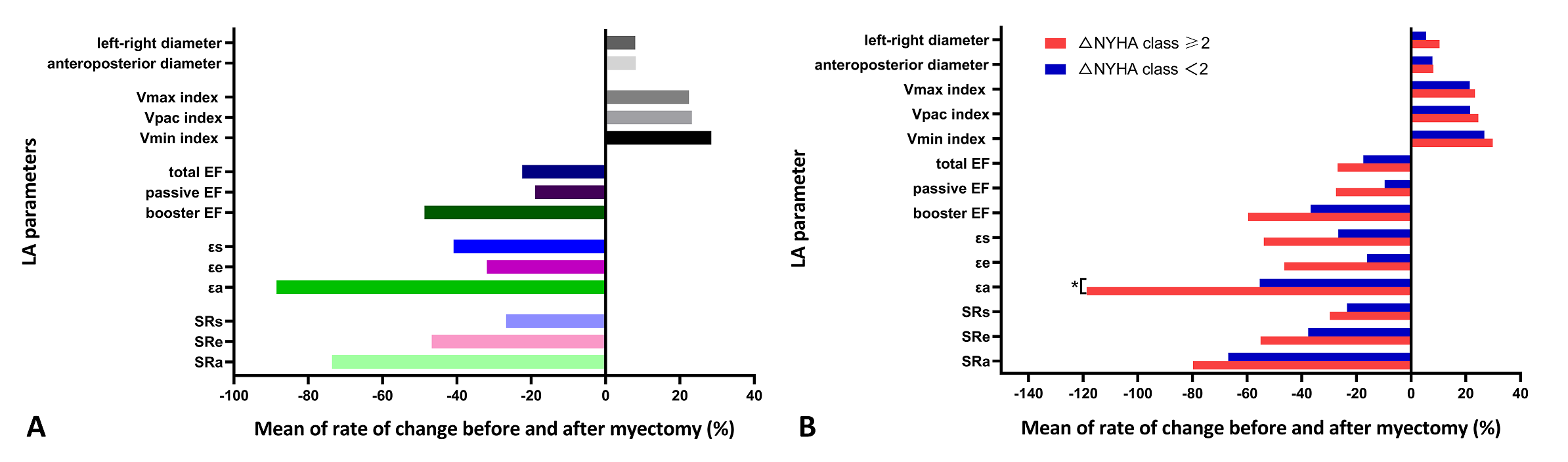
Bar graphs showing the rates of change of LA
structural and functional parameters in all patients with hypertrophic
obstructive cardiomyopathy after myectomy (A), and the comparisons for the
rates of change of LA parameters between two subgroups defined by whether ΔNYHA
function class was ≥ 2 after myectomy (B). EF = ejection fraction, LA = left
atrial, LAV = LA volume. Delta value (Δ) = preoperative
value – postoperative value, rate of change = delta value (Δ)/ preoperative
value × 100%.
DOI: https://doi.org/10.58530/2023/4699