4698
Cardiac Power to Mass Assessment by MRI in Patients with Hypertrophic Cardiomyopathy and Normal Ejection Fraction1Beijing Anzhen Hospital, Beijing, China, 2Philips Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Cardiomyopathy, Cardiomyopathy, cardiac power; hypertrophic cardiomyopathy; ejection fraction
Cardiac power (CP) output in patients with heart failure has been studied, while its importance in hypertrophic cardiomyopathy (HCM) patients is yet unclear.
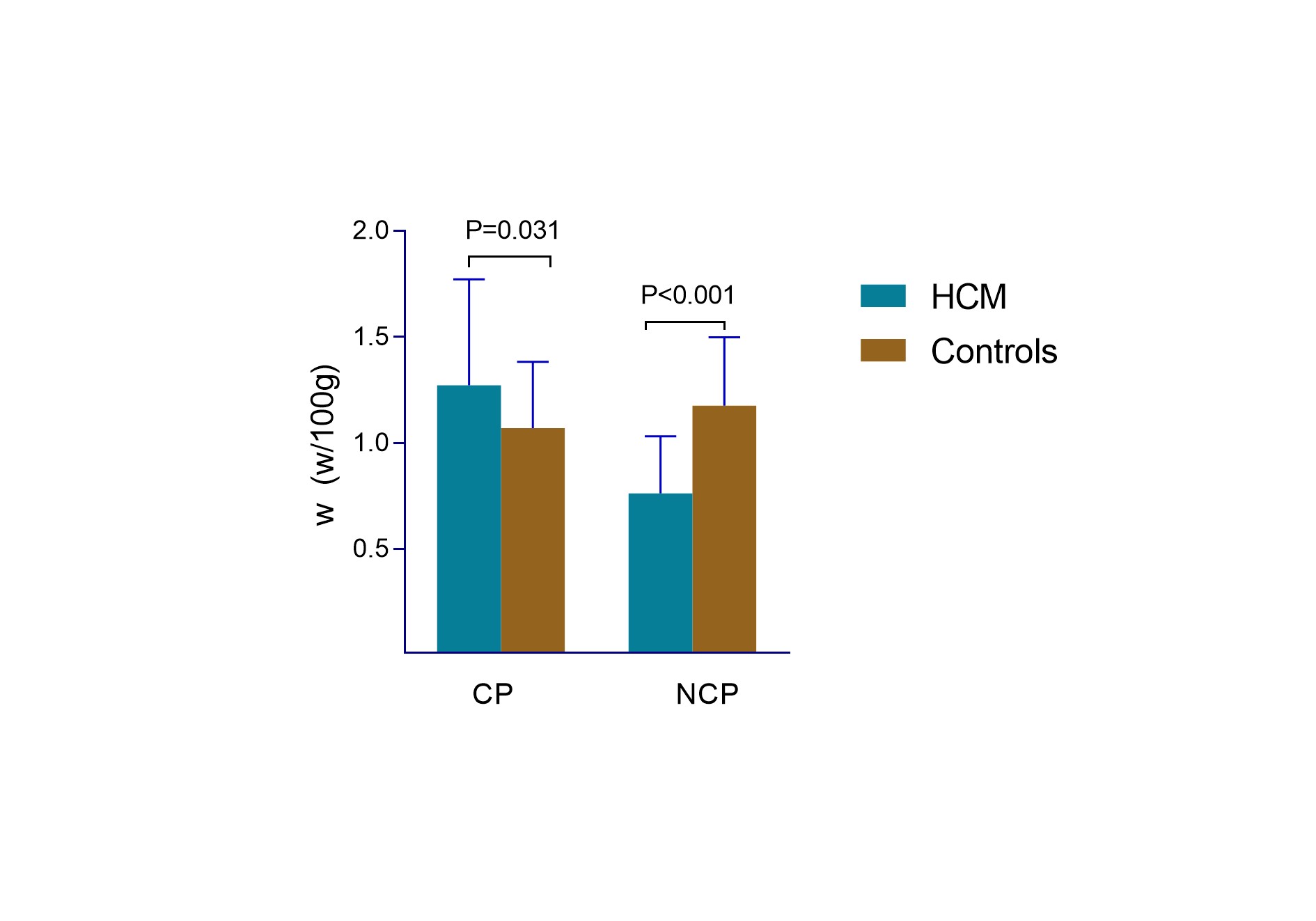
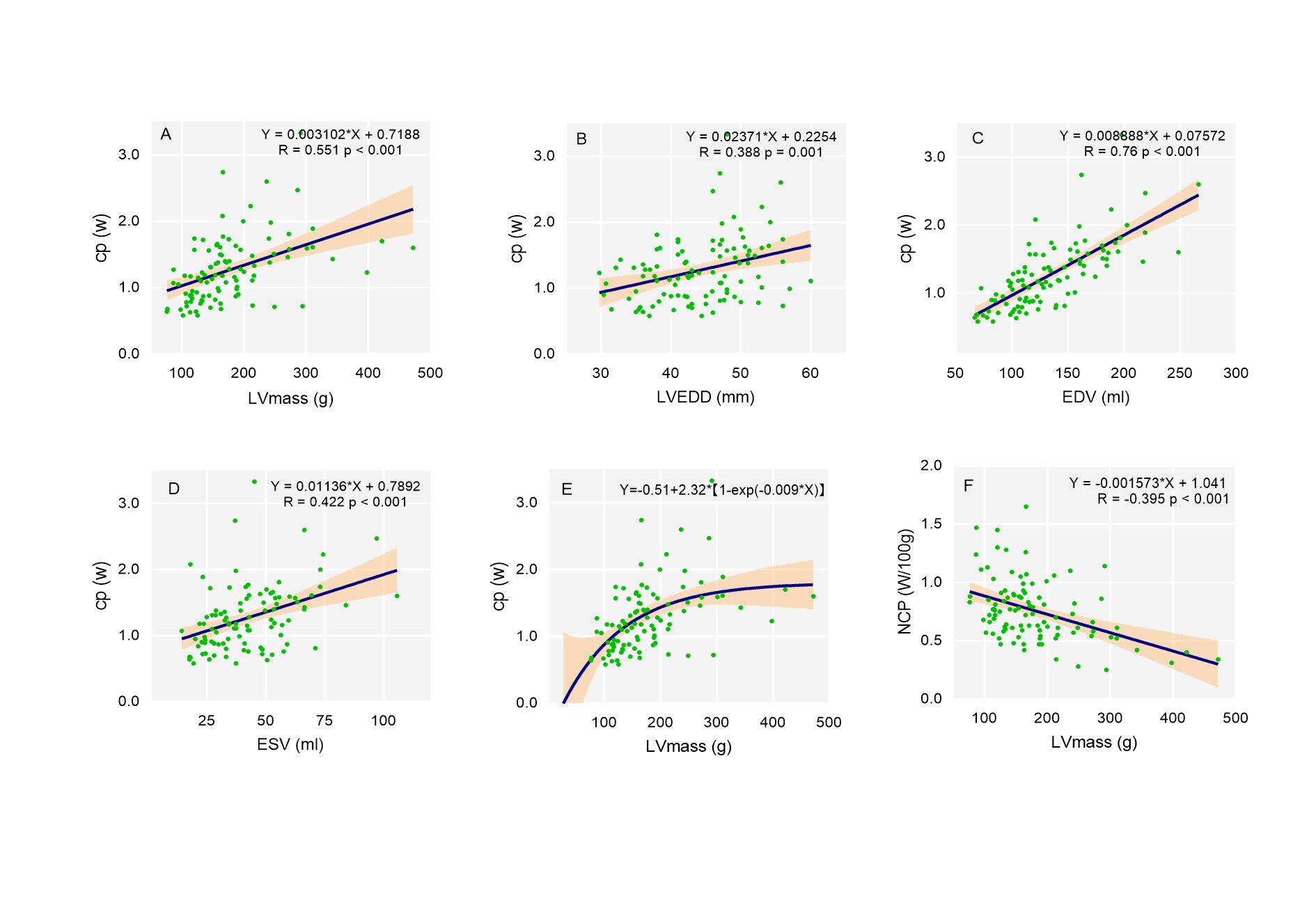
99 HCM patients and 65 gender- and age-matched controls with cardiac MR were included in the study. HCM patients showed significantly higher CP (p=0.031) but lowered NCP (p<0.001) than the controls. The correlation analysis of NCP and functional parameters revealed that NCP was inversely correlated with LV mass (R=-0.395, p<0.001) in HCM patients.
NCP decreased significantly in HCM patients and may continue to deteriorate with increasing LV mass.
Normalized cardiac power (NCP) represents the ability to generate energy by 100 g myocardium 1, 2. Previous studies have shown NCP is a robust indicator providing valuable prognostic information in patients with preserved or decreased ejection fraction (EF)1-3.
Pathological studies argue that the impaired systolic and diastolic function of HCM is caused by the abnormally thickened myocardium and chaotic myocardial fiber4. The disordered heart muscle cannot contract efficiently, leading to regional and global dysfunction, which is difficult to detect in the early stage5.
The role of NCP in assessing cardiac pump function in HCM patients with preserved EF is still unclear. The present study aimed to evaluate the role of CP normalized by LV mass in assessing cardiac pump function of HCM patients with preserved EF.
Methods
Study population
123 HCM patients who underwent cardiac magnetic resonance (CMR) and 87 healthy volunteers were enrolled in this study. 9/123 HCM patients with decreased EF and 15/123 HCM patients with myocardium surgery and valve disease were excluded; thus, 99 HCM patients and 65 gender- and age-matched controls were included in the analysis.
CMR scanning protocol
All patients underwent standardized CMR on a 3T CMR scanner. Steady-State Free Procession (SSFP) sequence was used to generate four-chamber, two-chamber, and short-axis cine imaging series. The late gadolinium enhancement (LGE) was performed by phase-sensitive inversion-recovery (PSIR) turbo field echo (TFE) sequence.
CMR image analysis for LV function
Commercial software cvi 42 (Circle Cardiovascular Imaging, Calgary, Canada) was used to analyze the CMR images. The left ventricular cardiac functional parameters, such as cardiac output(L/min), LVEF, and LV mass were estimated. LV maximal wall thickness and LV end-diastolic diameter (LVEDD) was acquired at the end-diastole.
Power/mass calculation
The formula of NCP at rest was as follows:
Power/mass=0.222 CO mean BP/LV mass
Mean BP=1/3 systolic BP+2/3 diastolic BP
0.222 in the formula is the transform constant to W/100 g of LV myocardium6.
Statistical analysis
All data were analyzed using SPSS (version 25.0, International Business Machines, Inc., Armonk, NY, USA). The chi-square test, two-sample T-test and Wilcoxon rank-sum test were used appropriately. Multivariate linear regression analysis was used to examine the correlation between relative factors and NCP. An optimized model was established by backward procedure. In HCM patients, Spearman’s correlation was used to evaluate the correlation between cardiac functional parameters and CP and NCP.
Results
Baseline clinical characteristics and CMR parameters in HCM patients and controls
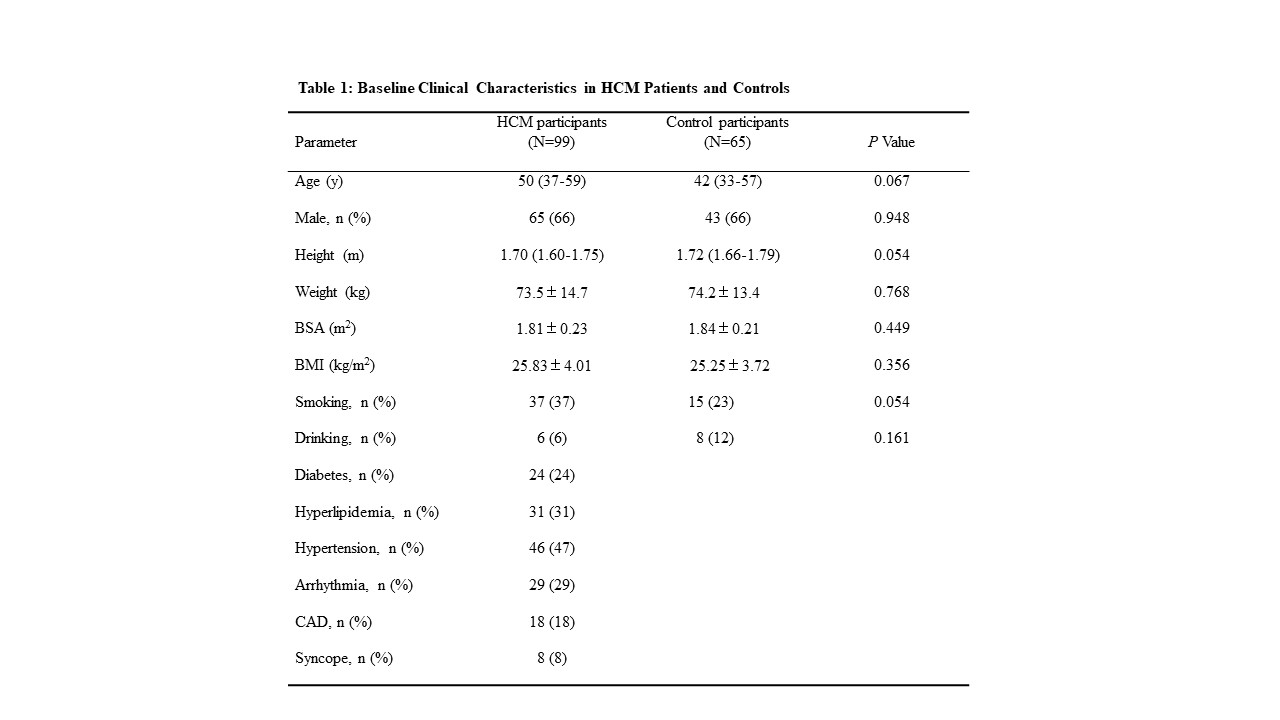
The study cohort consisted of 164 participants with median age 47 (range: 12–73) years: 99 HCM patients (60%, median age 50 years) and 65 age- and gender-matched controls (40%, median age 42 years). The HCM patients exhibited baseline clinical features similar to the controls (Table 1).
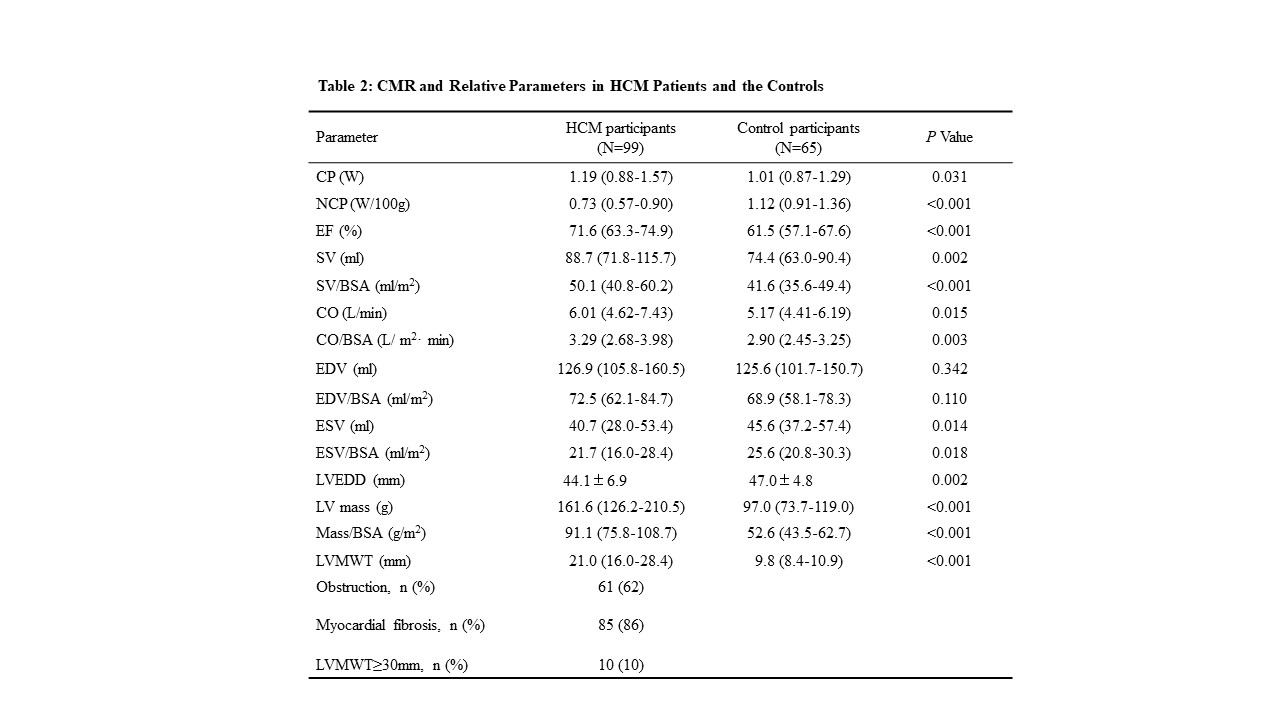
Compared to the controls, the HCM patients had a higher CP but significantly lower NCP (Table 2, Figure 1). HCM patients also had a higher EF (p<0.001), greater LV mass and LV mass/BSA (p<0.001 and p<0.001, respectively), and greater LVMWT (p<0.001). About 86% presented myocardial fibrosis, as assessed by LGE.
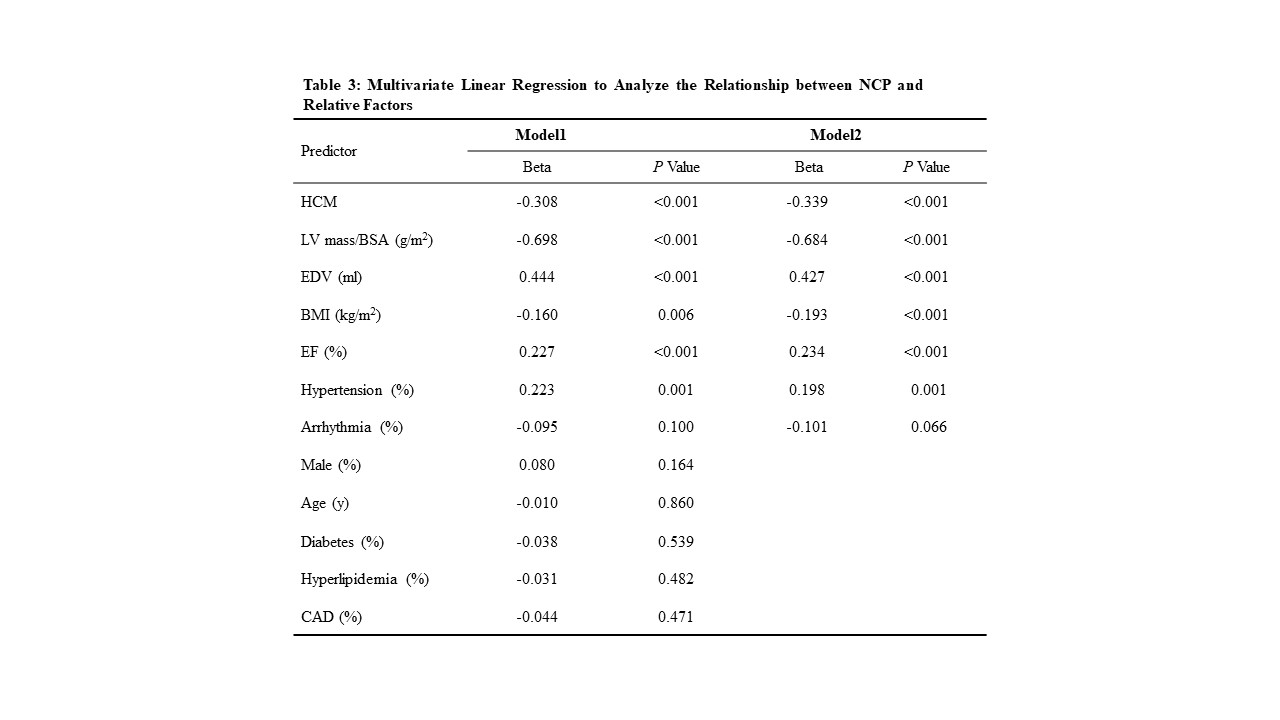
Multivariable analysis
In the final minimally adjusted model (following backward elimination), HCM (Beta=-0.339, p<0.001), LV mass/BSA (Beta=-0.684, p<0.001), EDV (Beta=0.427, p<0.001), BMI (Beta=-0.193, p<0.001), EF (Beta=0.234, p<0.001), and hypertension (Beta=0.198, p=0.001) were significantly associated with NCP (Table 3).
The correlation of CP and NCP with several key CMR parameters in HCM patients were showed in Figure 2.
Discussion
There are two key findings in the current study. First, HCM patients with normal LVEF have higher CP than the controls but lower NCP, which reflects the decreased power-generating capacity per unit mass of myocardium. Second, as the myocardial mass increases, NCP, power-generating capacity per unit mass of the myocardium, decreases significantly in HCM patients. These findings proved a major role of NCP in detecting ventricular dysfunction in HCM patients with preserved LVEF.
In the early stage of HCM, the increase in myocardial mass compensates for the decrease in work efficiency. Conversely, when comparing the myocardium efficiency by NCP, the power-generating capacity per unit mass of the myocardium decreased significantly. Pathological studies showed that HCM has hypertrophied myocardial cells and disorganized myocardial fiber, indicating that disorderly myocyte fibers replaced the well-organized muscle cells in the heart. This caused inefficient contraction and relaxation of the heart7, 8.
In general situation, CP depends on LV mass and its work efficiency, it will grow either mass augmentation or improved efficiency. The best physiological example of the former is the increase in LV mass in athletes, while in HCM patients, the myocardial fibers are impaired and deteriorate with increasing LV mass. Myocardial hypertrophy, disarray, and myocardial fibrosis result in impaired vertical inner fibers because these fibers are located in the sub-endocardium, which is most susceptible to myocardial disease, and followed by the circumferential and vertical outer fibers when the disease extends to mid-wall and sub-epicardial layers9. These features deteriorate the work efficiency of the myocardium gradually and decrease the NCP.
In conclusion, as a concise and non-invasive quantitative metric parameter of cardiac function, NCP plays a critical role in detecting and evaluating impaired cardiac pump function in HCM patients with preserved LVEF.
Acknowledgements
Funding:
This work was supported by the National Natural Science Foundation of China [U1908211]; and the Capital's Funds for Health Improvement and Research Foundation of China [2020-1-1052].
References
References
1. Anand V, Kane GC, Scott CG, et al. Prognostic value of peak stress cardiac power in patients with normal ejection fraction undergoing exercise stress echocardiography. European heart journal. 2021;42:776-785.
2. Cortigiani L, Sorbo S, Miccoli M, et al. Prognostic value of cardiac power output to left ventricular mass in patients with left ventricular dysfunction and dobutamine stress echo negative by wall motion criteria. European heart journal Cardiovascular Imaging. 2017;18:153-158.
3. Chen C, Zhao J, Xue R, et al. Prognostic significance of resting cardiac power to left ventricular mass and E/e' ratio in heart failure with preserved ejection fraction. Frontiers in cardiovascular medicine. 2022;9:961837.
4. Bluemke DA and Lima JAC. Using MRI to Probe the Heart in Hypertrophic Cardiomyopathy. Radiology. 2020;294:287-288.
5. Vigneault DM, Yang E, Jensen PJ, et al. Left Ventricular Strain Is Abnormal in Preclinical and Overt Hypertrophic Cardiomyopathy: Cardiac MR Feature Tracking. Radiology. 2019;290:640-648.
6. Dini FL, Mele D, Conti U, et al. Peak power output to left ventricular mass: an index to predict ventricular pumping performance and morbidity in advanced heart failure. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010;23:1259-65.
7. Reant P, Barbot L, Touche C, et al. Evaluation of global left ventricular systolic function using three-dimensional echocardiography speckle-tracking strain parameters. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2012;25:68-79.
8. Cameli M, Mondillo S, Solari M, et al. Echocardiographic assessment of left ventricular systolic function: from ejection fraction to torsion. Heart failure reviews. 2016;21:77-94.
9. Carasso S, Yang H, Woo A, et al. Systolic myocardial mechanics in hypertrophic cardiomyopathy: novel concepts and implications for clinical status. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2008;21:675-83.
Figures