4692
Performance of compressed-sensing cardiac MR in evaluating left ventricular function: a systematic review and meta-analysis1Radiology, Beijing Friendship Hospital, Capital Medical University, Beijing, China, 2Radiology, Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China, 3Heart Health Research Center, Beijing, China, 4Siemens Shenzhen Magnetic Resonance Ltd., Beijing, China
Synopsis
Keywords: Heart, Heart
SSFP-cine CMR imaging has been recommended to evaluate LV function and structure. However, a long scan time limited its widely application. A novel fast CS-cine CMR imaging might be an option, but its accuracy is inconclusive. Therefore, we conducted a systematic review and meta-analysis for it. We included 23 observational studies for pooling. There was no difference in LVEF, LVEDV, LVESV and LVmass, along with no heterogeneity across different subgroups by MR field intensity, breath-holding, children, and arrhythmia (all P for inter-subgroup heterogeneity <0.05). The quality of CS-cine images was acceptable and was superior to SSFP-cine images in arrhythmia patients.Introduction
Cardiac magnetic resonance (CMR) has been recommended as the gold standard for evaluating LV structure and function1. In current clinical practice, steady-state free precession (SSFP)-cine CMR sequence is widely used to evaluate LV characteristics, including LV ejection fraction (EF), end-diastolic volume (EDV), end-systolic volume (ESV), and mass. However, a long scan time requisite compromise its widely application. A novel fast compressed-sensing cine (CS-cine) CMR imaging might be an option. But the accuracy and applicability of CS-cine are still inconclusive2, 3.Methods
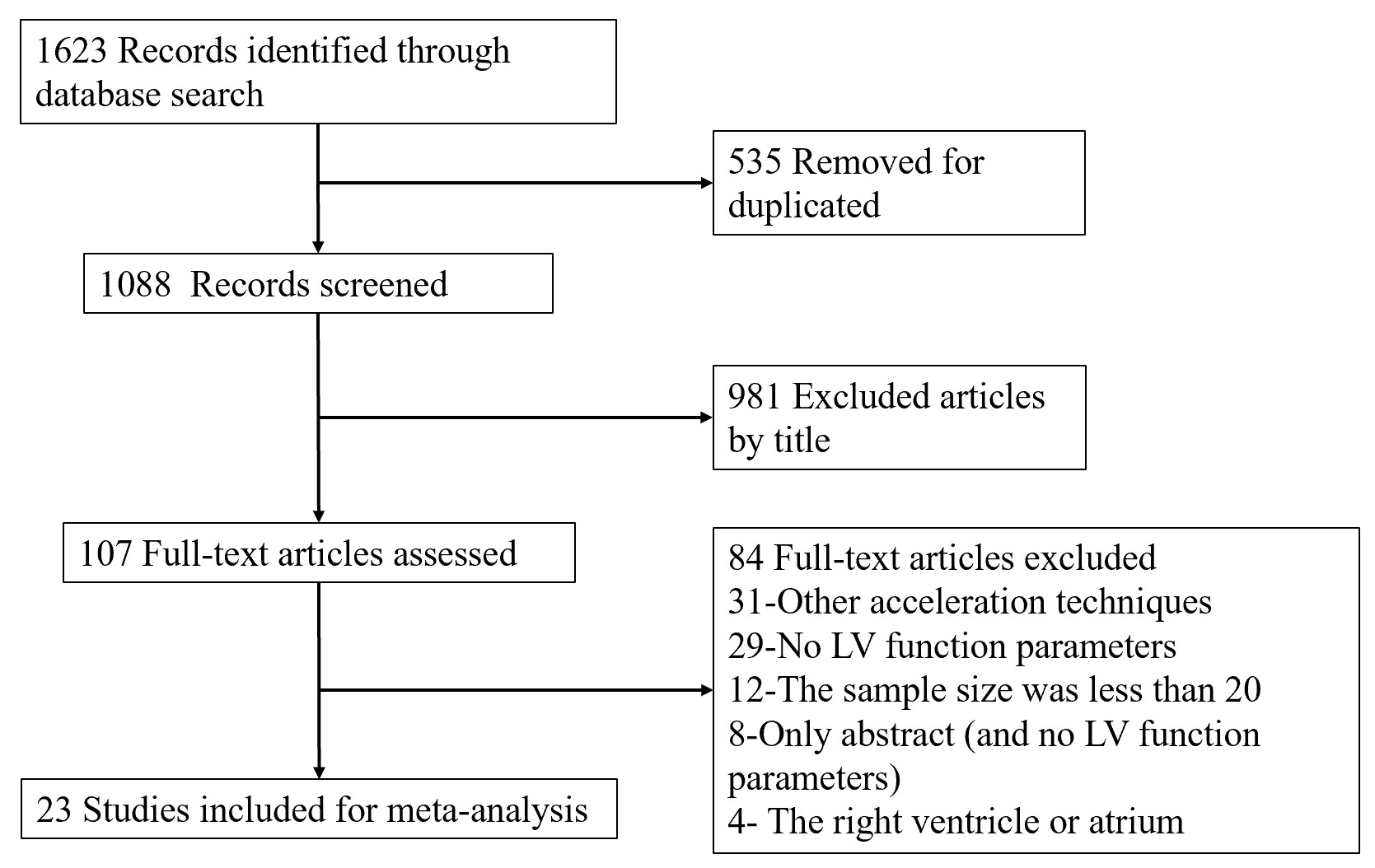
We conducted a systematic review and meta-analysis. Electronic databases were searched for studies where both CS-cine and SSFP-cine sequences were performed for individual participants. Furthermore, LV function or structure data from the two sequences were reported separately. Two investigators independently assessed the eligibility of retrieved studies and extracted data. Key outcomes included LV ejection fraction (LVEF), volume, mass, and image quality defined by a pre-specified ordinal 5-point scale (a higher point representing better quality). We performed subgroup analyses by children, breath control, arrhythmia, or MRI field intensity. Pooled standardized mean differences (SMD) with 95% CIs were estimated for LVEF and other continuous outcomes between CS-cine and SSFP-cine CMR sequences using the random-effects model weighted by inverse variance.Results
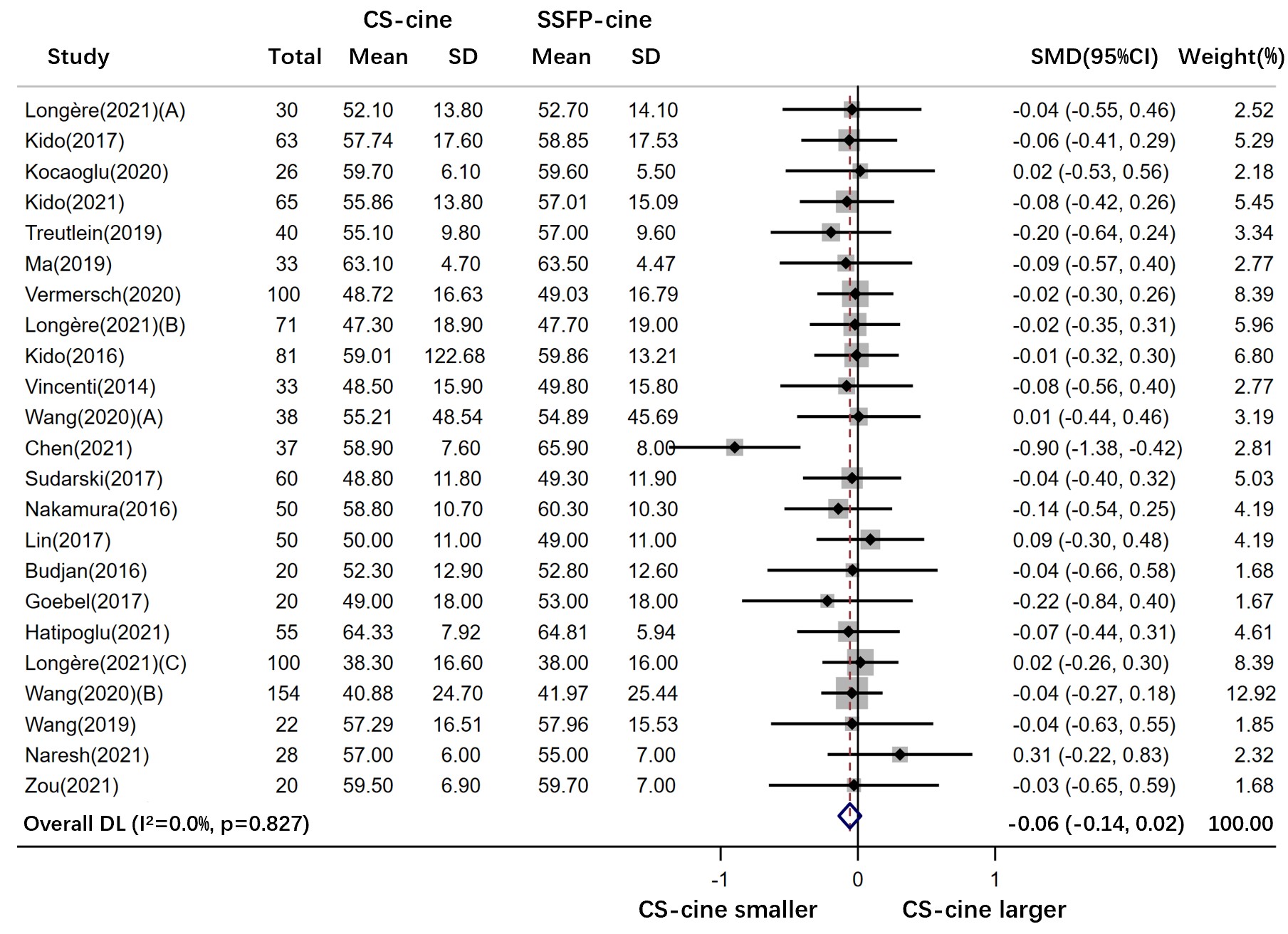
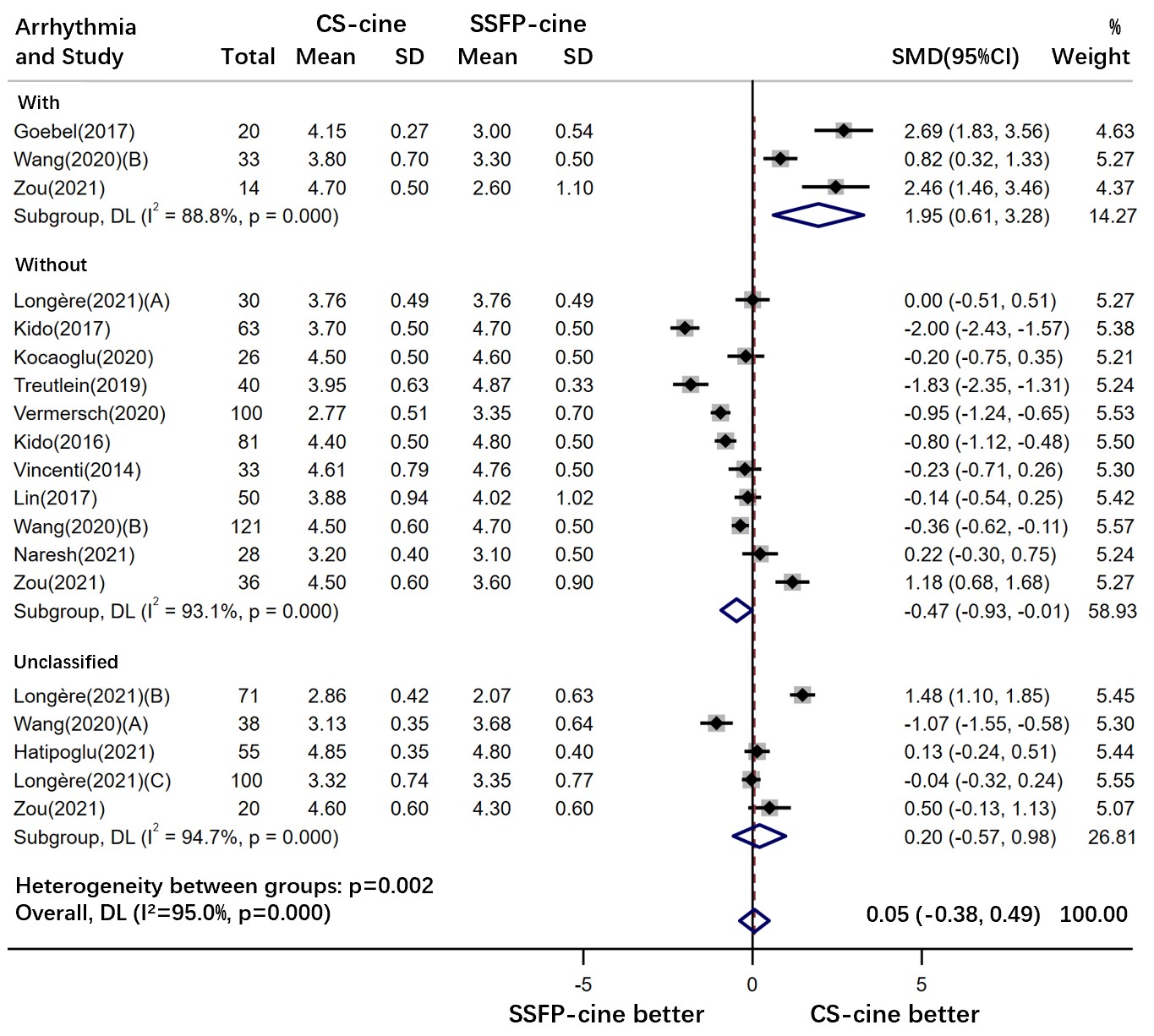
A total of 23 studies were included. There was no difference in LVEF obtained from CS-cine versus SSFP-cine imaging (SMD [95% CI]: -0.06 [-0.14, 0.02], P=0.16, I2=0.0%). So were other LV parameters (I2=0.0% to 0.0%), along with no heterogeneity across different subgroups by MR field intensity, breath-holding requirement, children, and arrhythmia (all P for inter-subgroup heterogeneity <0.05). Overall, the image quality was comparable between the two sequences (-0.19 [-0.63, 0.25], P=0.39, I2=94.7%). The high heterogeneity might be accounted by the difference across participants with arrhythmia (1.95 [0.61, 3.28], P=0.004, I2=88.8%) and without (-0.47 [-0.93, -0.01], P=0.045, I2=93.1%) or with no relevant information (0.20 [-0.57, 0.98], P=0.61, I2=94.7%).Discussion
Through a meta-analysis of existing studies, a sound method to reduce the possibility of any chance findings in individual studies, we identified a comparable performance of CS-cine versus the conventional SSFP-cine CMR imaging in LV evaluation with no differences in image quality between them as well. Our results favored the viewpoint that the CS-cine sequence could retain all essential MR signals that facilitate CMR images with sufficient sharpness and an acceptable noise level after Fourier transform, despite its rapidly incomplete MRI data acquisition by k-space undersampling4, 5. Accordingly, accurate endocardium and epicardium contours could be discriminated in the context of clear contrast between myocardium and the blood pool being achieved on CS-cine images6, the key to acquiring accurate LVEF and LV volume. Our subgroup analyses by breath control requirement and participant age confirmed the applicability of FB CS-cine imaging for them to evaluate LV function and structure with no deterioration of image quality compared with BH SSFP-cine sequence. Therefore, BH could be exempted and these people should have a more comfortable experience during the CMR examination on the basis of a CS-cine sequence.Conclusions
There were no differences across the fast CS-cine and conventional SSFP-cine imaging regarding LV characteristics evaluation. The quality of CS-cine images was acceptable and was superior to conventional cine images in the setting of arrhythmia.Acknowledgements
No acknowledgement found.References
1. Moon JCC, Lorenz CH, Francis JM, Smith GC, Pennell DJ. Breath-hold FLASH and FISP Cardiovascular MR Imaging: Left Ventricular Volume Differences and Reproducibility. Radiology. 2002;223(3):789-97.
2. Goebel J, Nensa F, Schemuth HP, Maderwald S, Quick HH, Schlosser T, et al. Real-time SPARSE-SENSE cine MR imaging in atrial fibrillation: a feasibility study. Acta Radiol. 2017;58(8):922-8.
3. Longère B, Allard PE, Gkizas CV, Coisne A, Hennicaux J, Simeone A, et al. Compressed sensing real-time cine reduces cmr arrhythmia-related artifacts. J Clin Med. 2021;10(15).
4. Vincenti G, Monney P, Chaptinel J, Rutz T, Coppo S, Zenge MO, et al. Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass. JACC: Cardiovascular Imaging. 2014;7(9):882-92.
5. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58(6):1182-95.
6. Kido T, Hirai K, Ogawa R, Tanabe Y, Nakamura M, Kawaguchi N, et al. Comparison between conventional and compressed sensing cine cardiovascular magnetic resonance for feature tracking global circumferential strain assessment. J Cardiovasc Magn R. 2021;23(1).
Figures