4691
A Multi-Sequence SSFP-SPGR One-Breath-Hold Cine-Tag MR – Extent of Hybrid Artifact Interference1Biomedical Engineering, Illinois Institute of Technology, Chicago, IL, United States, 2Medicine - Cardiology, University of Chicago Medical Center, Chicago, IL, United States, 3Radiology, University of Chicago Medical Center, Chicago, IL, United States, 4Philips, Gainesville, FL, United States, 5Philips, Best, Netherlands, 6Medicine, University of Virginia, Charlotesville, VA, United States
Synopsis
Keywords: Myocardium, Preclinical
A single-breath-held (BH) cine and tag MRI offers a hybrid SSFP-SPGR contrast approach with potential to provide quantitative measures of regional myocardial wall motion. Such approaches overcome the need for inter-BH misregistration during conventional, multi-sequence acquisition. In this study, we examine the extent of artifact interferences that manifest by means of the bypassed pre-scan calibration steps for the less sensitive SPGR-tag scan. A consecutive cohort of 25 subjects that yielded ~400 cine- and tag-volumes were retrospectively analyzed to examine the prevalence of artifact, interference with motion assessment, and the rate of yielding assessable wall motion via the hybrid one-breath-hold approach.Introduction
In MR, multi-parametric and multi-contrast acquisition schemes are emerging, where unique combination of contrasts carry clinical value. Among well-recognized methods include MR fingerprinting1 and use of custom MR systems architecture such as Philips’ MISS2-4 for instantaneous switching and interleaved k-space acquisition from multiple pulse sequences at once, but these methods often require extensive research modifications that limit their uses to select advanced MR sites. One alternative approach with potential clinical scalability is the ‘pre-scan bypassed’ SSFP-SPGR method5 which minimizes the extent of modifications to the MR systems architecture by instead utilizing the default superimposed pre-scan calibration parameters for consecutive prescriptions of matched geometries. For this approach, we demonstrated initial feasibility in jointly tuning the calibrations of both bSSFP-cine and the subsequent SPGR-based MR-tag to the bSSFP-cine pre-scan, and overcame acquisition constraints of two typically mutually exclusive sequences in different breath-holds. However, under such loosened calibration conditions despite matched geometries, existence of scan trade-offs often manifest as acquisition artifacts – including those employed to aggressively accelerate both Cine and Tag to fit within a one-breathhold duration. In this study, we examine the extent of such manifested imaging artifacts through a retrospective analysis of all acquired bSSFP-cine and SPGR-tags, and determine the real-world utility of joint hybrid visualization approach in terms of: a) wall motion visualization, b) robustness against surgical implants/off-resonances, and c) improved functional depiction by hybrid image.Materials and Methods
Our examined acquisition5 was performed on 25 anesthetized swine subjects (13 pediatric ~30kg; 12 adult ~70kg with various surgical implants) under ventilator-controlled breathing as ‘add-on’ acquisitions to an ongoing MRI research study on a single scanner (Philips Ingenia 3T DDAS). Several pre-scan calibration steps (F0, shimming, B0 drift, etc.) were bypassed for the SPGR-Tag following bSSFP-cine, where these two pre-scans were matched. This was achieved by modifying the latter SPGR to employ: 1) a custom inverted bSSFP refocusing pulse in the readout direction to enable a pseudo-SPGR contrast (Cartesian), or 2) a manually optimized spiral-SPGR readout. A flip angle (FA) of 60°, small 240x240 mm2 reduced FOV, and default CS-SENSE acceleration R=2 were used for Cine, and the Tag employed FA=25° with matched CS-SENSE R=2 (Cartesian) or FA=15° (Spiral). All in-vivo scans were acquired by one of two technologists both blinded to our study design, whom were allowed to jointly modify both sequence parameters with one stipulation that the geometric prescriptions needed to be fully matched.Every dataset acquired in this consecutive subject cohort (Sept 2021-Nov 2022) were first randomized and scored by one blinded reader using a 5-point ordinal scale: [0=non-diagnostic; 1=poor/significant CS artifact present; 2=fair/some artifact; 3=good; 4=excellent] who assessed the volume slice throughout the full cardiac cycle per score (animated Fig 1). A representative slice in the 2-, 3-, 4- and short-axis prior to contrast injection were examined. The bSSFP and Tag scores were unblinded and the lowest scored data subsets were re-examined jointly with a second 4-point scale in terms of myocardium motion against per each separate image; i.e. [-1=non-diagnostic; 0=no improvement; 1=modest improvement; 2=significant improvement]. Inferences from these scores are reported below.
Results
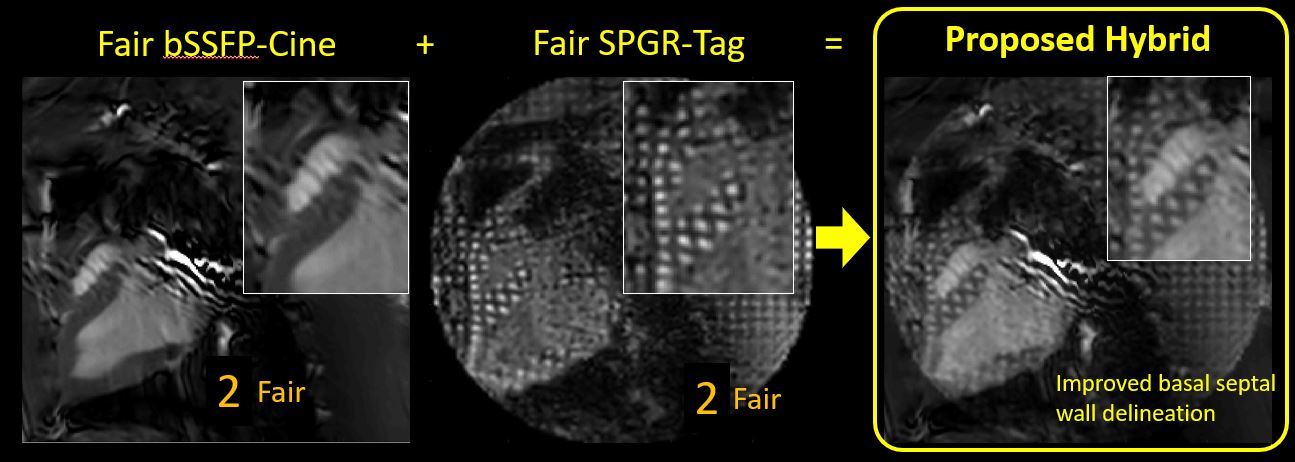
From approximately ~400 consecutively acquired functional CMR volumes (196 cines with 201 tags) at our site, 188 of these employed spiral Tags (versus 13 cartesian Tags) as the preferred acquisition by the designated imaging technologist. nbypass=134 of these were single-breath-held pre-scan ‘bypassed’ cine-tags, versus npartial=39 partially prepared, and nfull=14 fully prepared cine-tag acquisitions over separate breath-holds. nother=14 scans did not have a matching bSSFP-cine pair.In the subset of data where both the cine and tag scored ‘fair’ or worse (score=2 or less; n=43 such acquisition pairs were counted out of 186 cine-tag pairs, or 23%), the generated joint assessment of cine+tag for myocardial motion yielded a second score as follows: 0 cases were non-diagnostic, 7 of these did not improve after hybrid assessment, 10 yielded modest improvement, and 19 yielded notable improvement. Figure 2 contains one such example.
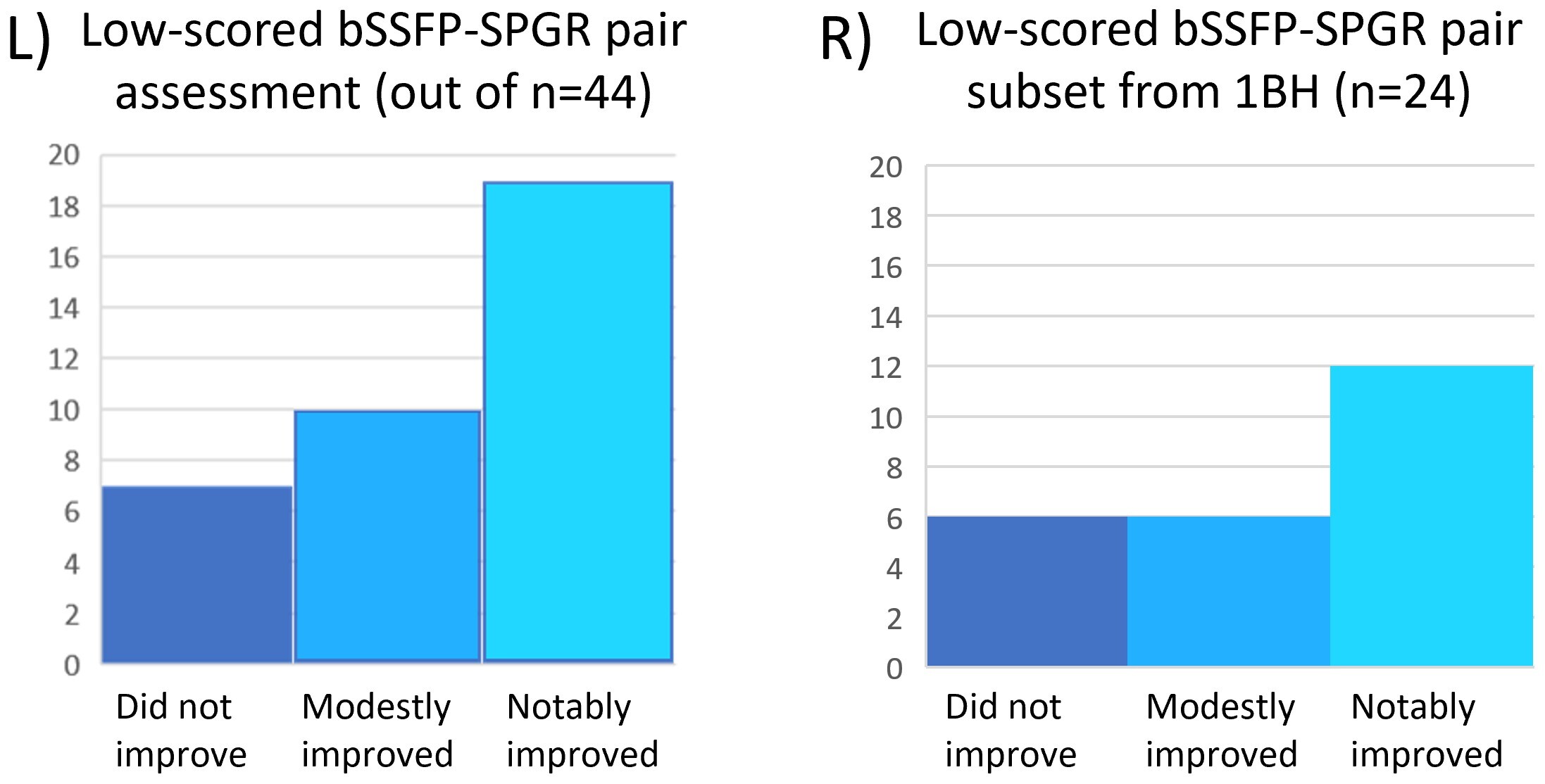
n=7 pairs were not scored due to VCG triggering error (n=6) that yielded considerable mismatch between the cine and tag frames, and n=1 case yielded geometric mis-prescription below the apex – and was only recognized through the joint assessment with both cine and tag. Of the 44 examined low-scoring pairs, 24 of these were among the nbypass=134 (or 14%); whose hybrid scores were notably improved against isolated assessment - 12 notably better; 6 modestly better; 6 did not improve (Fig 3). Additionally, in n=7 of such cases, the reader upon unblinding and joint assessment recommended reassessing the ‘fair’ Tag score as ‘good’. Thus, about 1 in 7 acquisitions warranted both poor cine and tag acquisitions that would normally warrant scan repeat, but when combined, can provide superior wall motion delineation.
Discussion
Our analysis showed that over 75% of our examined volumes yielded diagnostic quality images, both the employed rFOV+CS-SENSE cines with surgical implants and off-resonance artifacts in addition to the already sub-optimally calibrated SPGR-Tags led to diminished quality volumes. While such volumes may be ill-suited for myocardial wall motion assessment by themselves, their hybrid image improved the wall motion delineation in 18 out of the 24 single-BH cases – showing potential for clinical utility.Acknowledgements
This project was supported by NIH K25 HL141634 (Kawaji) and partially by NIH R01 HL143468 (Kawaji – subcontract).References
1. Ma D., Gulani V., Seiberlich N. et al. Magnetic Resonance Fingerprinting, Nature 2013; 495:187–192.
2. Henningsson M., Mens G. Koken P. et al. A new Framework for Interleaved Scanning in Cardiovascular MR: Application to Image-Based Respiratory Motion Correction in Coronary MR Angiography. MRM 2015, 73(2):692-6.
3. Nazir N., Patel AR., Narang A. et al. Scan-Time Reduction by Improved Utilization of Idle Times by Permuting Pre-Scan Ordering: Feasibility Demonstration of a Single Breath-Hold Strain-Encoded CMR. Washington DC. P332.
4. Wang H., Lanier M., Kawaji K. et al. Acquisition of bSSFP and Tagged Cines in a Single Breath-Hold for Myocardial Wall Motion Assessment: A Feasibility Study. ISMRM CMR Workshop 2017. New York, NY. pp20.
5. Goes J., Nguyen V., Gorre D. et al. An SSFP-SPGR Multi-sequence Cardiac Cine-Tag Acquisition Approach in One Breath-hold, ISMRM 2022 London UK.
Figures